
Abstract
Transcutaneous oxygen tension measurement (TcPO2) is widely applied for the evaluation of chronic limb-threatening ischemia (CLTI). Nevertheless, studies that focused on the clinical value of TcPO2 have shown varying results. We identified factors that potentially play a role in TcPO2 measurement variation such as probe placement, probe temperature, and the use of a reference probe. In this review of the current literature, we assessed the application of these factors. A systematic search was conducted. Parameters that were assessed were probe placement, probe temperature, and mentioning and/or use of a reference probe. In total, 36 articles were eligible for analysis. In 24 (67%) studies, probes were placed on specific anatomical locations. Seven (19%) studies placed probes, regardless of the location of the ulcer, adjacent to an ischemic lesion or ulcer (perilesion). Selected temperature setting of the probe differed; in 18 (50%), a default probe temperature of 44°C was selected, and in 13 (36%), a different temperature was selected. In 31 (84%) studies, the use of a reference probe was not reported. Transcutaneous oxygen tension measurement is applied diversely in patients with CLTI. Homogeneity in TcPO2 protocols is warranted for reliable clinical application and to compare future TcPO2 research.
Keywords
Introduction
Chronic limb-threatening ischemia (CLTI) is an increasing major health-care problem worldwide with a large impact on quality of life, morbidity and mortality, and health-care expenses. 1 –3 The main treatment goals of CLTI management are wound healing, prevention of amputation, and preservation of ambulation. 1 Transcutaneous oxygen tension measurement (TcPO2) has been proposed as a promising noninvasive tool for the diagnosis and evaluation of CLTI, especially in diabetes. 4,5
The measurement of local oxygen pressure is believed to reflect the status of underlying vascularization of the skin. With the use of the so-called “Clark electrode,” PO2 is measured by a platinum cathode and a silver anode covered with a thin membrane which is permeable for oxygen. 6 The electronical reduction of oxygen allows a current to flow which is proportional to the partial pressure of oxygen. 6 To ensure dermal permeability for oxygen, the electrode is heated creating local hyperthermia liquefying the crystalline structure of the stratum corneum. Furthermore, hyperthermia creates underlying capillary vasodilatation allowing more oxygen diffusion. 7,8
Despite the use of TcPO2 in clinical practice, its added value for the diagnosis and evaluation of therapy in patients with CLTI is strongly debated as studies have shown poor to moderate reliability and reproducibility. 9 –13 A recent review on TcPO2 reported a sensitivity ranging from 0.61 to 0.82 for the prognosis of diabetic foot ulcer (DFU) healing. 12 Moreover, reported TcPO2 threshold values for the detection of ischemia or potential non-healing DFUs differ significantly. 10,14 –24
Recently, the Society of Vascular Surgery proposed the “Wound, Ischemia, and foot Infection, (WIfI)” classification system to assess the risk of limb amputation and chance of successful revascularization in patients with CLTI. 25 Moreover, the European Society for Vascular Surgery has adopted and implemented the WIfI in their most recent guideline on the management of peripheral artery disease (PAD). 26 Based on the aggregate of grades determined by wound presence, level of ischemia, and severity of infection, a treatment strategy can be proposed as well as an estimation of the prognosis can be made. The WIfI recommends that if arterial calcification precludes reliable ankle–brachial index or toe pressure measurement, ischemic grade should be classified with TcPO2.
Since WIfI scores should ideally translate into treatment decisions, it is essential that TcPO2 results are reliable and reproducible. This underlines that TcPO2 measurement should be conducted homogenously and factors that may interfere with the test should be kept to a minimum. We assume that the discrepancies between reported threshold values in studies on TcPO2 are, at least partially, due to differences in protocols for measurement. Our objective is to review methods of TcPO2 measurement and explore potential factors that influence these values in patients with CLTI.
Methods
For this review, we conducted a systematic search on PubMed, EMBASE, and the Cochrane Library for peer-reviewed publications on TcPO2 in patients with CLTI using synonyms for “transcutaneous –oximetry, -oxygen or TcPO2” and “critical limb or peripheral arterial disease and ischemia” and reviewed references of reviews. All observational studies and clinical trials on CLTI and TcPO2 were included. Exclusion criteria were lack of TcPO2 measurement, absence of CLTI, for example, DFUs without ischemia, nonhuman studies, language other than English, or if no full text was available. All eligible articles were analyzed for the protocol used to measure TcPO2 and—if available—the relation of TcPO2 values and outcomes. The following potential parameters were assessed: probe placement, probe temperature, and mentioning and/or use of a reference probe. All studies were reviewed by two researchers (B.L. and J.W.) independently.
Results
A flowchart of the systematic search is shown in Figure 1. A total of 437 publications were screened. After exclusion, 36 articles remained eligible for analysis. An overview of the study characteristics and results is demonstrated in Table 1. A total of 13 studies involved an experimental intervention, 8 studies on success of percutaneous transluminal angioplasty (PTA), 7 observational studies, 6 studies on experimental diagnostics, and 2 studies on wound healing after amputation.
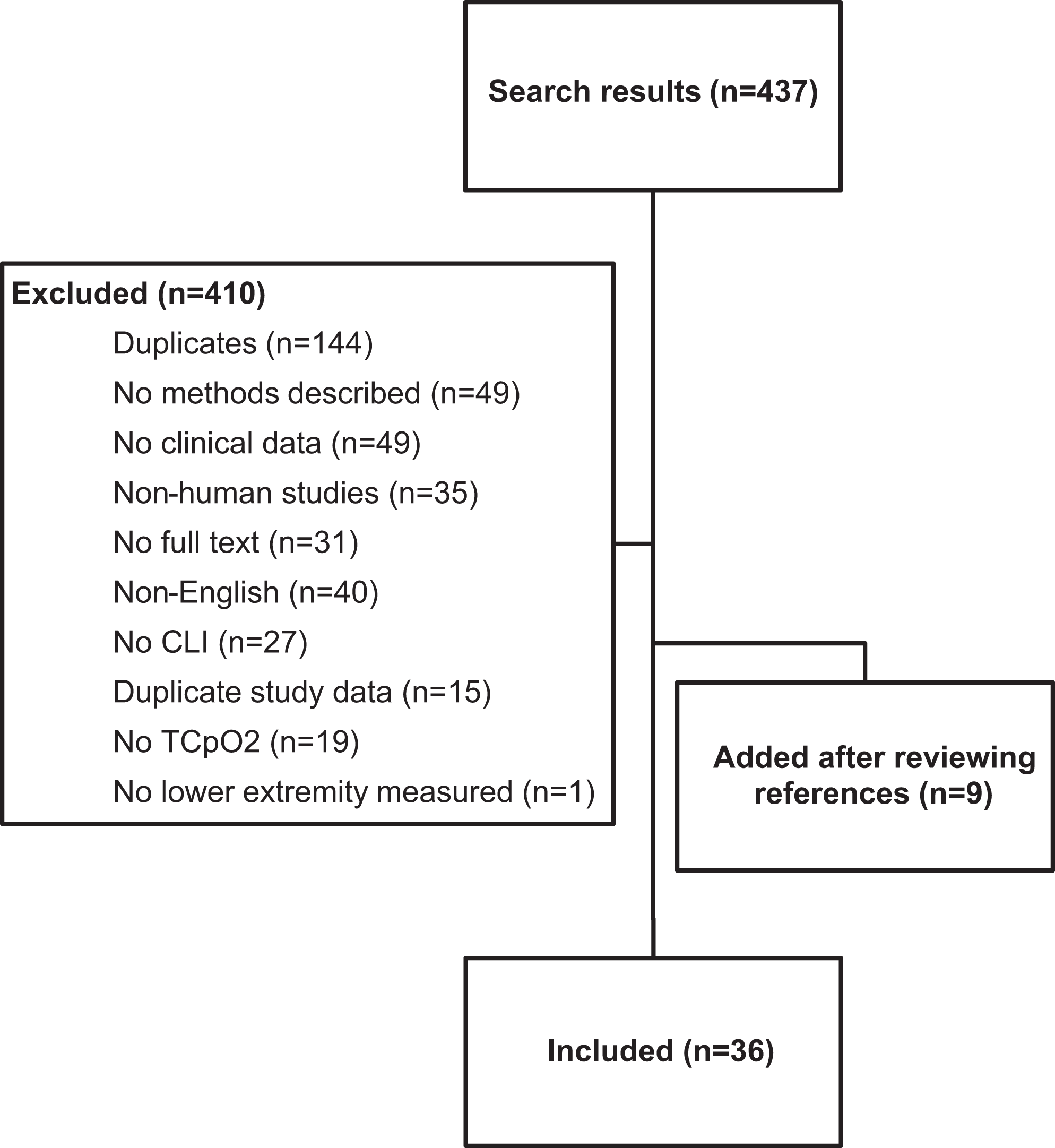
Overview of study selection.
Overview of Included Studies.
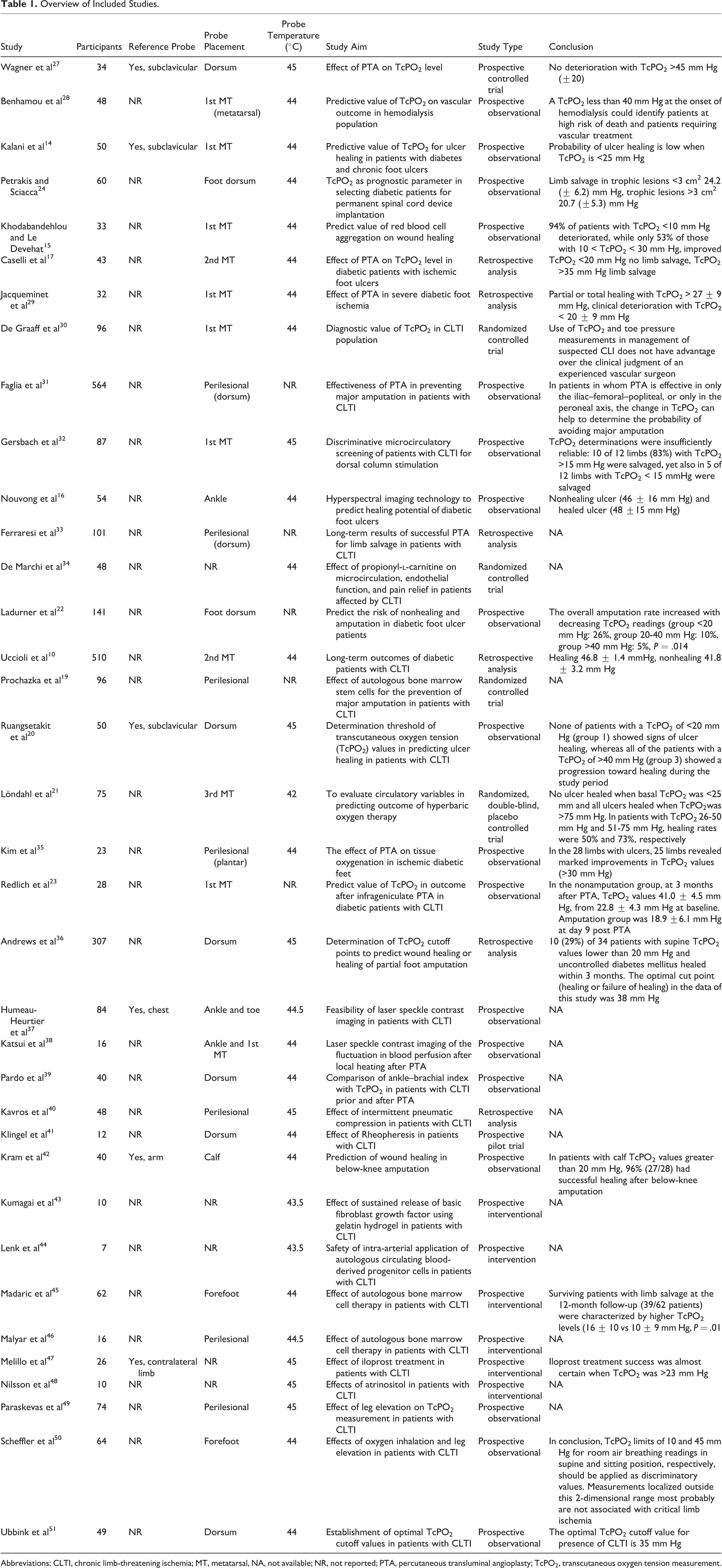
Abbreviations: CLTI, chronic limb-threatening ischemia; MT, metatarsal, NA, not available; NR, not reported; PTA, percutaneous transluminal angioplasty; TcPO2, transcutaneous oxygen tension measurement.
Probe Placement
In 24 (67%) studies, probes were placed on specific anatomical locations. These locations were on the dorsum of the foot (n = 20, 54%), ankle (n = 3, 8%) and calf (n = 1, 3%; Table 1). A total of 7 (19%) studies placed probes adjacent to an ischemic lesion or ulcer (perilesion) irrespective of the location of the lesion. In 5 (14%) studies, the specific location was not reported (Table 1).
Probe Temperature
Among the selected temperature settings of the probe, the following was noted: in 18 (50%) studies, a default probe temperature of 44°C was selected, in 8 (22%) studies 45°C, in 2 (5%) studies 43.5°C, in 2 (5%) studies 44.5°C, and in 1 (3%) study 42°C. In 5 (14%) studies, probe temperature was not reported.
Reference Probe
In 31 (84%) studies, the use of a reference probe was not reported. In 4 (11%) studies, the reference probe was applied at the chest (eg, subclavicular) region, in 1 (3%) study on the arm, and in 1 (3%) on the contralateral limb. Only one study used reference probe values for the interpretation of systemic oxygenation.
Relation of TcPO2 and Outcome
As apparent from the studies shown in Table 1, ulcer healing and limb prognosis were in general poor if TcPO2 is <20 mm Hg and were in general good if >40 mm Hg; however, even these values varied between studies.
Discussion
We found substantial differences in probe placement, probe temperature, and reference probe application in studies on TcPO2 use in CLTI. Moreover, cutoff values for wound healing and limb prognosis varied between studies.
It is known that the abovementioned variations in TcPO2 protocols affect the obtained values. For example, in general, the lower extremity has different oxygen tension levels influenced by local factors, such as skin thickness. 52 Hence, the selected probe site affects TcPO2 value. Although ischemic lesions may occur on different anatomical locations on the lower extremity, 53 standardization of TcPO2 probe location is crucial to reduce the intra- and interpatient variability.
Furthermore, TcPO2 measurement using the Clark electrode is influenced by the selected probe temperature. 54 -57 Cutaneous warming of, for example, the diabetic foot has shown a profound effect on TcPO2 values showing a 40.8 ± 23.8 mm Hg difference between a probe temperature of 37°C and 44°C. 54 The TcPO2 manuals suggest a probe temperature between 43°C and 45°C, 58 44°C and 45°C, 59 or 45°C 60 ; hence, the majority of studies used 44°C as default temperature. However, a consensus statement of an expert panel proposed a default temperature of 45°C. 61 Since studies on the effect of TcPO2 probe temperature on TcPO2 values in CLTI and its relation with prognosis are lacking, the optimal probe temperature in CLTI remains unknown.
Finally, it is suggested that TcPO2 values are influenced by the systemic oxygen level. Therefore, the placement of a reference probe on the thorax is recommended to correct for systemic hypoxia. We found that 6 studies mentioned the use of a reference probe. However, in 2 of these studies, values or interpretation of the reference probe remained unclear. An indicator which takes into account the systemic oxygen influence is the regional perfusion index (RPI), 62,63 which is calculated by dividing the TcPO2 values of the limb by TcPO2 thorax values. The RPI has been successfully applied to evaluate vascularization of the extremities, 64 -66 which is also recommended by TcPO2 measurement device manufacturers. However, thorax TcPO2 values are subject to the same variability as for the limb; hence, the ratio of the two could mathematically result in a greater variability than that of each factor separately. Therefore, more comparative research is required to validate and determine accurate thresholds for RPI and their added value in comparison to absolute cutoff TcPO2 values in CLTI for usage in clinical practice. Another proposed strategy is to add pulse oximetry (SO2) to rule out arterial hypoxemia. 58 -60 However, studies on SO2 and its correlation with TcPO2 values of the lower limb are lacking.
A major limitation in this review is the impossibility to address the specific impact of probe location, probe temperature, and use of reference probe on the measured TcPO2 values due to the fundamental differences in study aim and therefore patient population in the individual studies. Moreover, the study design of the included studies was very heterogeneous: 13 studies involved an experimental intervention, 8 studies on success of PTA, 7 observational studies, 6 studies on experimental diagnostics, and 2 studies on wound healing after amputation. Still, we demonstrate that the method of TcPO2 use differs undoubtedly and point out the sensitivity of TcPO2 measurement in general. Hence, it might be suggested that heterogeneity in method of use alters TcPO2 values.
With the recently introduced WIfI classification system in the current ESC guidelines, 26 TcPO2 plays a role in grading ischemia and the determination of the treatment strategy in patients with CLTI. For example, if a patient has a shallow ulcer on the foot without gangrene and no signs of infection and TcPO2 measurement is 40 mm Hg, the patient is categorized as having a very low risk of limb amputation and low requirement for revascularization. However, if the same patient has a TcPO2 of 29 mm Hg, there is a moderate risk of limb amputation and a high requirement for revascularization. 26 This indicates a prominent role for TcPO2 to determine treatment strategy. Moreover, the usefulness of the ankle systolic pressure, imbedded in the WIfI classification, to predict the risk of major amputation in CLTI is currently under debate. 67 Especially in patients with CLTI with concomitant diabetes mellitus or chronic renal failure, TcPO2 seems more reliable in comparison to current macrovascular diagnostics. 68 Furthermore, other factors in method of TcPO2 use should be addressed to provide an adequate risk stratification scheme for TcPO2, such as positioning of the patient (supine vs sitting) and additional oxygen inhalation, both methods have proven to increase the predictive value of wound healing prognosis. 69,70 All these factors underline the importance of a standardized method of TcPO2 measurement and careful interpretation of these values. The effect of altering specific variables during TcPO2 assessment remains unclear. Therefore, we are currently conducting an observational study to investigate the influence of probe location and the added value of the RPI on wound healing prognosis. Also, in our vascular laboratory, we are conducting experimental TcPO2 studies to investigate a new photo-optical form of TcPO2. It has been suggested that photo-optical TcPO2 is not affected by probe temperature compared with the standard electrochemical TcPO2.
Conclusions
Transcutaneous oxygen tension measurement for the evaluation of limb perfusion in patients with CLTI is applied in standard clinical practice and is included in WIfI and international guidelines on PAD management, therefore affecting treatment decisions. However, there is a strong heterogeneity in methods used to assess TcPO2. A substantial diversity in probe temperature, probe location, and the use of a reference probe was found among studies regarding TcPO2 in CLTI. The varying values and different conclusions of the reviewed studies underline the importance of a homogeneous protocol in order to interpret and possibly compare measurement values and use these values to guide treatment decisions. Prior to the implementation of TcPO2 as part of treatment guidelines, it is mandatory that (international) TcPO2 measurement protocols become available and are validated to guarantee reliable and reproducible TcPO2 results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.