
Abstract
Introduction:
This study aimed to evaluate the efficacy and safety of limus-based drug-eluting stent (DES) implanted in medium or small coronary vessels during a very long-term follow-up period.
Methods:
A total of 2383 patients treated with 2916 limus-based DES between April 2003 and March 2015 were evaluated. The enrolled patients were stratified into 3 groups according to the reference vessel diameter: group A: ≤2.5 mm; group B: 2.51 to 3.00 mm; group C: 3.01 to 3.50 mm.
Results:
Group A had a significantly higher loss index and binary restenosis rate than the other 2 groups at 9 months of angiographic follow-up. Group A also had a significantly higher rate of target lesion revascularization and a lower rate of major adverse cardiovascular event–free survival than the other 2 groups after a follow-up period of 68 ± 59 months. The long-term cardiovascular event–free survival curves based on a Cox regression model showed large vessel size, and second-generation DES had better outcomes.
Conclusion:
An inverse relationship between vessel size (≤3.5 mm) and clinical outcomes was noted in patients who received limus-based DES implantation.
Introduction
Coronary vessel size is an important determinant of outcomes in patients who undergo percutaneous coronary interventions (PCIs), irrespective of bare metal stent (BMS) or drug-eluting stent (DES) implantation. 1,2 Furthermore, a small vessel diameter has been associated with higher restenosis and event rates. 3
An inverse relationship between vessel size and restenosis rate following BMS implantation may be caused by the limited ability of small vessels to accommodate lumen renarrowing after stenting. 4 This inverse relationship has also been noted with DESs, although not as obviously as with BMSs. 2,5 However, different DESs have been shown to have different performance rates. Several studies have shown that sirolimus-eluting stents (SESs) have significantly lower rates of angiographic restenosis and major adverse cardiovascular events (MACEs) than paclitaxel-eluting stents (PESs). 6 –9 In this study, we aimed to evaluate the efficacy and safety of first- and second-generation limus-based DESs in medium and small coronary vessels during a very long-term follow-up period.
Materials and Methods
Patients
The Cardiovascular Atherosclerosis and Percutaneous TrAnsluminal INterventions registry is a prospective, physician-initiated, single-center observational database that has been maintained since November 1995. This is an ongoing registry and includes the data of 7200 consecutive patients who underwent elective and emergency PCIs with stenting at our hospital from November 1995 to July 2015. We enrolled 2383 consecutive patients from this registry who underwent DES implantation between April 2003 and March 2015. The vessel diameters of all of these patients were ≤ 3.5 mm. Ethical approval for this study was obtained from the institutional review board of Chang Gung Medical Foundation. All of the patients provide informed consent to undergo the procedure and follow-up protocol, as well as consent to publish case details. The inclusion criteria for stenting were evidence of myocardial ischemia and >50% stenosis in a native coronary artery or in a bypass vein graft that was suitable for stenting. The exclusion criteria were severe multivessel disease requiring bypass surgery, contraindications for the use of aspirin, clopidogrel, or ticagrelor, and patients who refused to undergo the procedure. Dual antiplatelet therapy with aspirin and clopidogrel/ticagrelor was administered to all of the included patients for at least 9 months. The enrolled patients were stratified into 3 groups according to the reference vessel diameter (RVD; group A: ≤2.5 mm, group B: 2.51-3.00 mm, group C: 3.01-3.50 mm). We then analyzed immediate and late outcomes among these 3 groups.
Interventional Procedures and Clinical Follow-Up
The stent implantation procedures were performed through the femoral or radial artery according to standard techniques. Predilation was performed using an undersized balloon if the lesion was very tight (>70% stenosis). The choice of the type of stent was made by the operator, mainly on the basis of the available stent size. After initial stent deployment, high-pressure balloon inflation (≥14 atm) was applied. Cardiac isoenzymes were measured in all of the patients immediately and 6 hours after the procedure. Data on clinical status, medical management, and occurrence of any adverse events were obtained from the patients’ medical records. The patients were clinically followed up through outpatient visits or telephone contact. Clinical follow-up visits were scheduled at 1, 2, 3, 6, 9, and 12 months after the procedure and every 3 months thereafter. Angiographic follow-up was recommended as routine after 9 months or earlier in cases of suspected recurrent myocardial ischemia. If a patient developed chest pain with evidence of myocardial ischemia and greater than 50% stenosis in a native coronary artery or a bypass vein graft angiographically, further PCI with stenting was performed where appropriate. Cypher (Johnson and Johnson, Warren, New Jersey) was classified as first-generation DES; Endeavor and Resolute (Medtronic, Minneapolis, Minnesota), Xience (Abbott Vascular, Santa Clara, California), and Promus (Boston Scientific, Natick, Massachusetts) were classified as second-generation DES.
Angiographic Analysis
Quantitative angiographic analysis was conducted with a selected end-diastolic cine frame that showed stenosis in its most severe and nonforeshortened view. A contrast-filled guidance catheter was used as reference for calibration. Random measurements were performed by 2 blinded experienced angiographers. The interobserver correlation coefficient (r) was .93 (P < .01), and the intraobserver correlation coefficient was .95 (P < .01). The minimal luminal diameter (MLD), RVD, percentage of diameter stenosis, and balloon diameter were measured using the automatic edge detection or digital calibration method (DCI or Integris BH3000; Philips, Eindhoven, the Netherlands). Binary restenosis was defined as ≥50% stenosis of the luminal diameter in the target lesion at the time of follow-up angiography. Acute gain was defined as the difference between baseline and final MLD, late loss as the difference between final poststenting and follow-up MLD, net gain as the difference between acute gain and late loss, and loss index as the ratio of late loss to acute gain. The left ventricular ejection fraction was measured from the left ventricular angiogram obtained at a right anterior oblique projection with an angle of 30°.
Definitions
We defined an in-hospital MACE as death, ST-segment elevation myocardial infarction (STEMI) or non-STEMI (NSTEMI), the need for emergency bypass surgery, or a cerebrovascular accident (CVA). The cardiovascular events during the follow-up period included cardiac death, reinfarction (STEMI or NSTEMI), target lesion revascularization (TLR), stenting in a new lesion, or necessitation of coronary bypass surgery. The STEMI was diagnosed according to standard methods if the patient experienced prolonged chest pain (longer than 30 minutes) that could not be relieved by nitroglycerin, showed an ST-segment elevation of ≥0.2 mV in at least 2 contiguous electrocardiographic (ECG) leads, and had significantly elevated creatine kinase (CK)-MB enzyme levels. The definition of NSTEMI is that patient had ischemic chest pain or chest tightness with an elevation of serum cardiac markers (CK-MB or troponin) and may be associated with ECG changes, such as ST-segment depression.
Statistical Analysis
We used STATA statistical software (version 10) for all statistical analyses. The final results were presented as mean ± standard deviation or as percentages, and categorical data were presented as numbers. The normality of all variables was analyzed. Multivariable Cox proportional hazards model was used to identify the independent predictors of long-term cardiovascular event. Adjusted survival curves were conducted for independent predictors with the Cox proportional hazard models and methods for calculating adjusted survival. A P value <.05 was considered to be statistically significant.
Results
Patient Characteristics
There were a total of 138 patients in group A, 1066 patients in group B, and 1179 patients in group C. There were no significant differences among the 3 groups in terms of age, gender, hypertension, dyslipidemia, recent infarction, or left ventricular function. More patients in group A than the other 2 groups had diabetes mellitus (49%, 46%, and 28%, respectively; P < .001), multivessel disease (75%, 71.5%, and 65.2%, respectively; P < .001), and lower rate of current smokers (23%, 30%, and 36%, respectively; P = .020; Table 1).
Patient Characteristics.
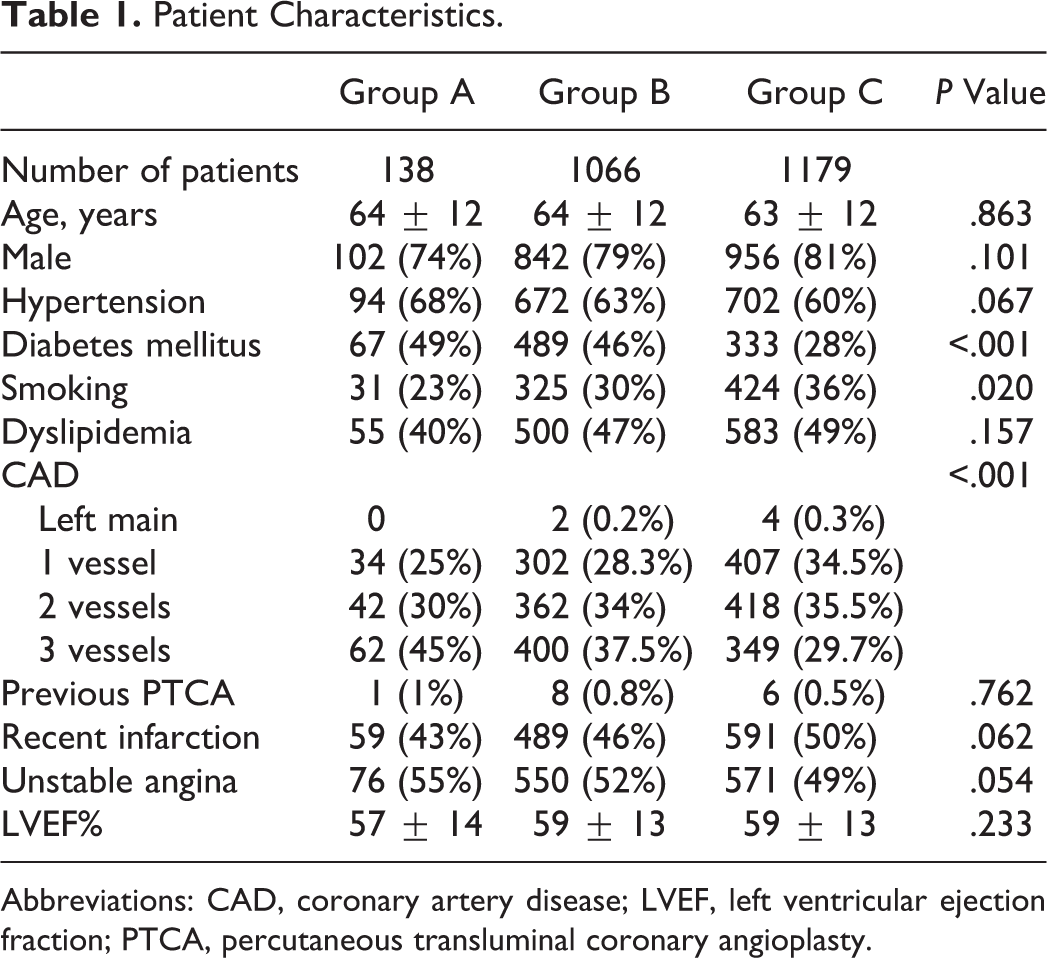
Abbreviations: CAD, coronary artery disease; LVEF, left ventricular ejection fraction; PTCA, percutaneous transluminal coronary angioplasty.
Lesion Characteristics
There were a total of 140 lesions in group A, 1187 lesions in group B, and 1275 lesions in group C (Table 2). Most lesions were located in the left anterior descending artery and the middle part of the treated artery among all 3 groups. The mean length of the lesions in group A was shorter than in the other 2 groups (19 ± 8 mm, 23 ± 11 mm, and 23 ± 12 mm, respectively; P < .001). With respect to lesion morphology, group C had a significantly higher incidence of eccentric lesions (39%, 34%, and 31%, respectively; P < .001) and thrombus-containing lesions (15%, 4%, and 9%, respectively; P = .018) than the other 2 groups.
Lesion Characteristics.
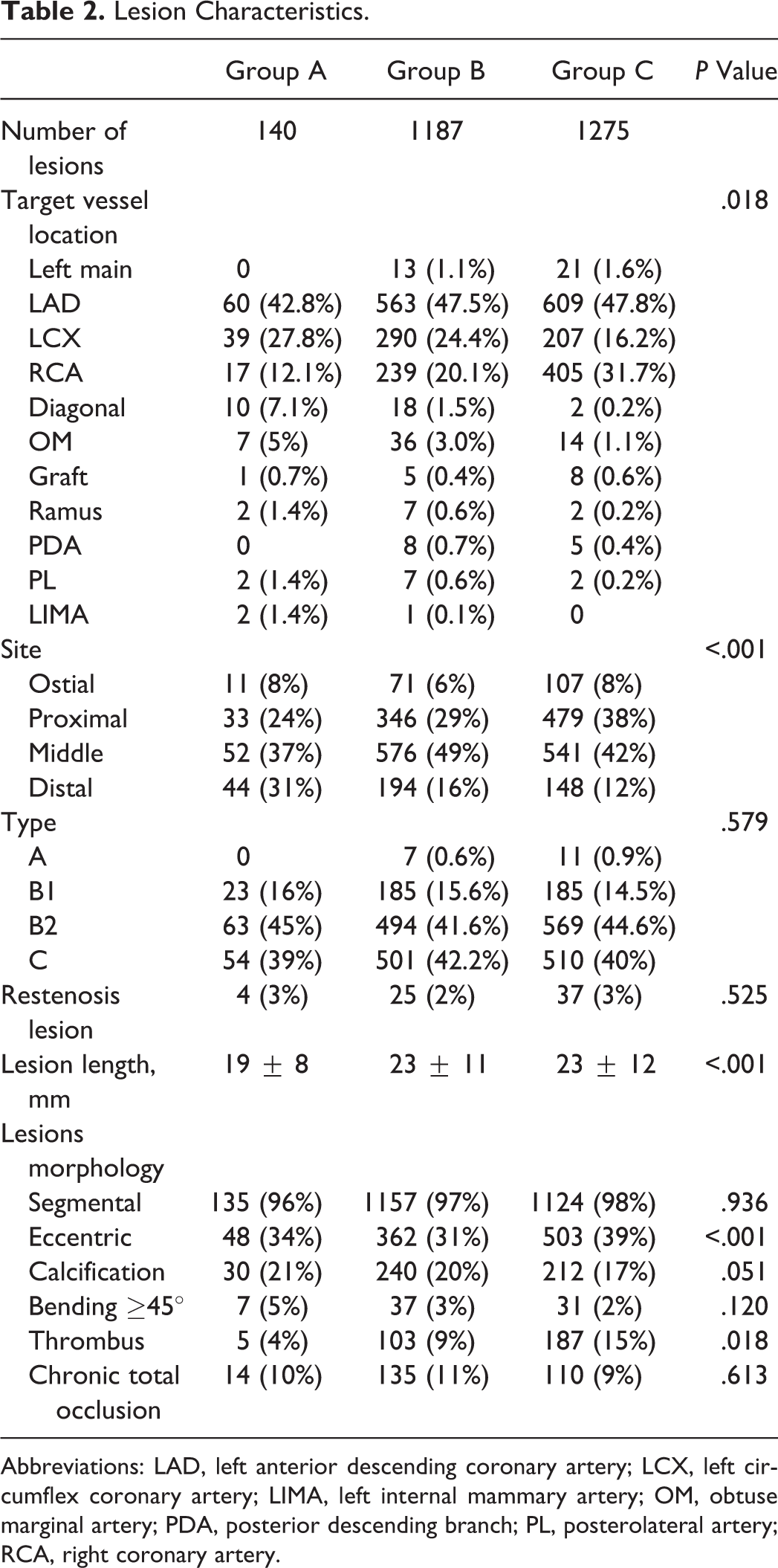
Abbreviations: LAD, left anterior descending coronary artery; LCX, left circumflex coronary artery; LIMA, left internal mammary artery; OM, obtuse marginal artery; PDA, posterior descending branch; PL, posterolateral artery; RCA, right coronary artery.
Procedural Results and In-Hospital Events
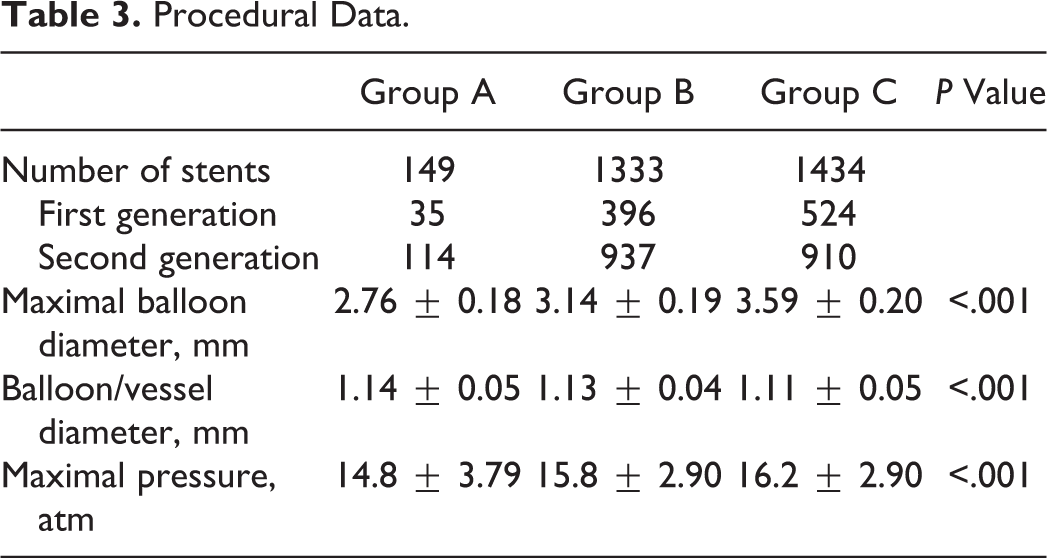
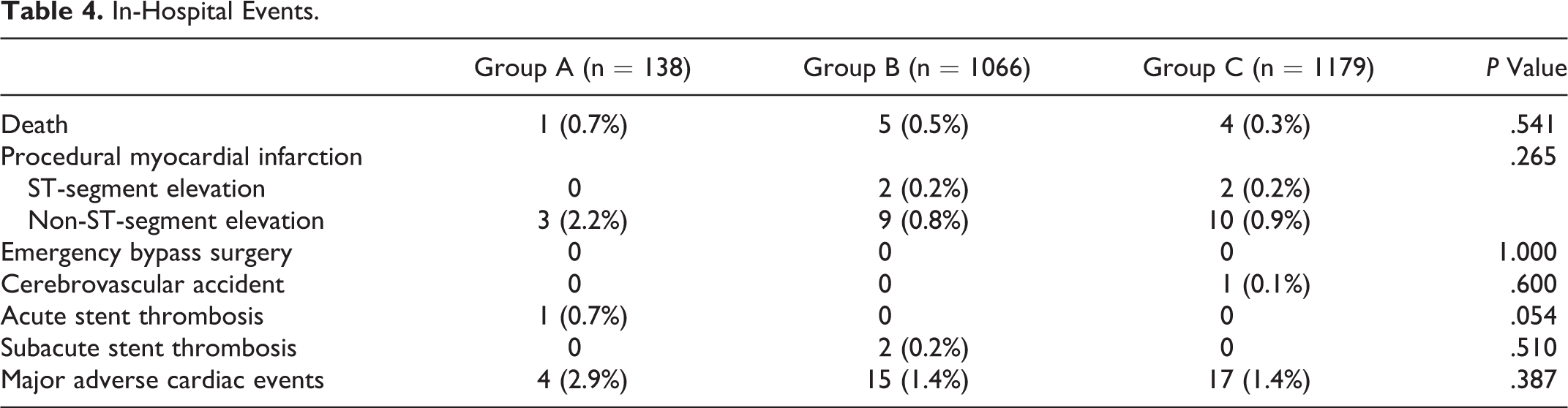
In total, 149 stents (35 first generation and 114 second generation) were implanted in group A, 1333 (396 first generation and 937 second generation) in group B, and 1434 (524 first generation and 910 second generation) in group C. Group C patients had a larger maximal balloon diameter (3.59 ± 0.20 mm, 2.76 ± 0.18 mm, and 3.14 ± 0.19 mm, respectively; P < .001), a lower ratio of balloon to vessel diameter (1.11 ± 0.05, 1.14 ± 0.05, and 1.13 ± 0.04, respectively; P < .001), and a higher maximal inflation pressure (16.2 ± 2.90 atm, 14.8 ± 3.79 atm, and 15.8 ± 2.90 atm, respectively; P < .001) than the other 2 groups (Table 3). One patient in group A, 5 in group B, and 4 in group C died in the hospital. Two patients in group B and 2 in group C developed STEMI, and 3 patients in group A, 9 in group B, and 10 in group C developed NSTEMI. One patient in group A developed acute stent thrombosis, and 2 patients in group B developed subacute stent thrombosis. The in-hospital MACE rates were not different among the 3 groups (2.9%, 1.4%, and 1.4%, respectively; P = .387; Table 4).
Procedural Data.
In-Hospital Events.
Angiographic Analysis
Follow-up angiography was performed in 101 patients with 103 lesions in group A (follow-up rate: 80%), 300 ± 88 days after stenting, 673 patients with 743 lesions in group B (follow-up rate: 75%), 284 ± 69 days after stenting, and in 782 patients with 838 lesions in group C (follow-up rate: 77%), 286 ± 66 days after stenting. Group A had the smallest MLD and RVD before stenting, after stenting, and in follow-up angiography, followed by group B and then group C (Table 5). After 9 months of follow-up, group A had a higher percentage of the diameter of stenosis than the other 2 groups (28%, 20%, and 17%, respectively; P < .001). In addition, group A had the smallest acute gain, followed by group B and group C (1.90 ± 0.33 mm, 2.21 ± 0.40 mm, and 2.49 ± 0.49 mm, respectively; P < .001), as well as net gain (1.54 ± 0.68 mm, 1.85 ± 0.69 mm, and 2.15 ± 0.79 mm, respectively; P < .001). Consequently, there was a significant difference in the loss index among the 3 groups (0.25 ± 0.33, 0.17 ± 0.28, and 0.14 ± 0.28, respectively; P = .001). The lesion restenosis rate was higher in group A than in groups B and C (12.6%, 6.3%, and 5.5%, respectively; P = .021).
Quantitative Angiographic Measurements.
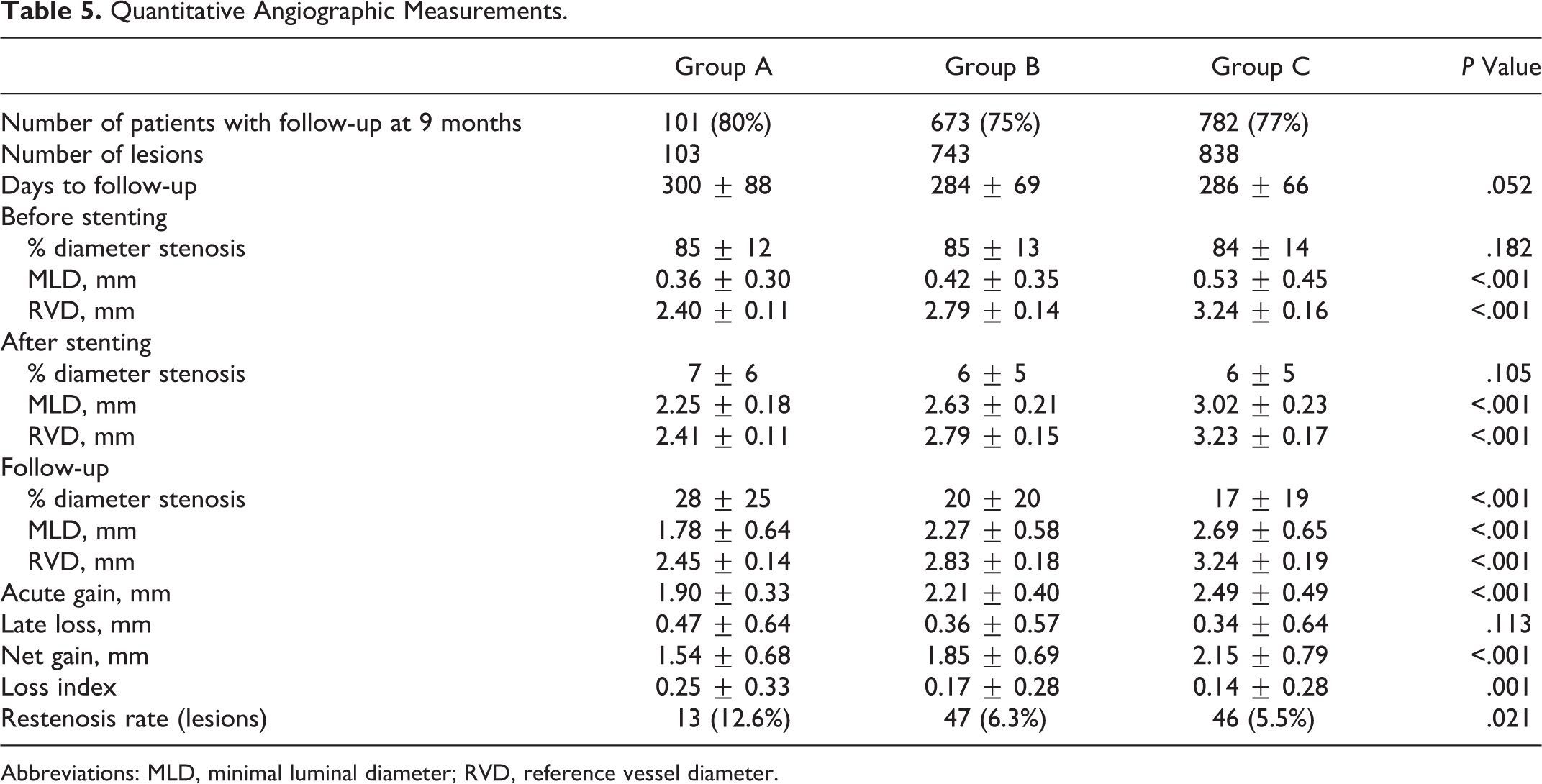
Abbreviations: MLD, minimal luminal diameter; RVD, reference vessel diameter.
Long-Term Outcomes
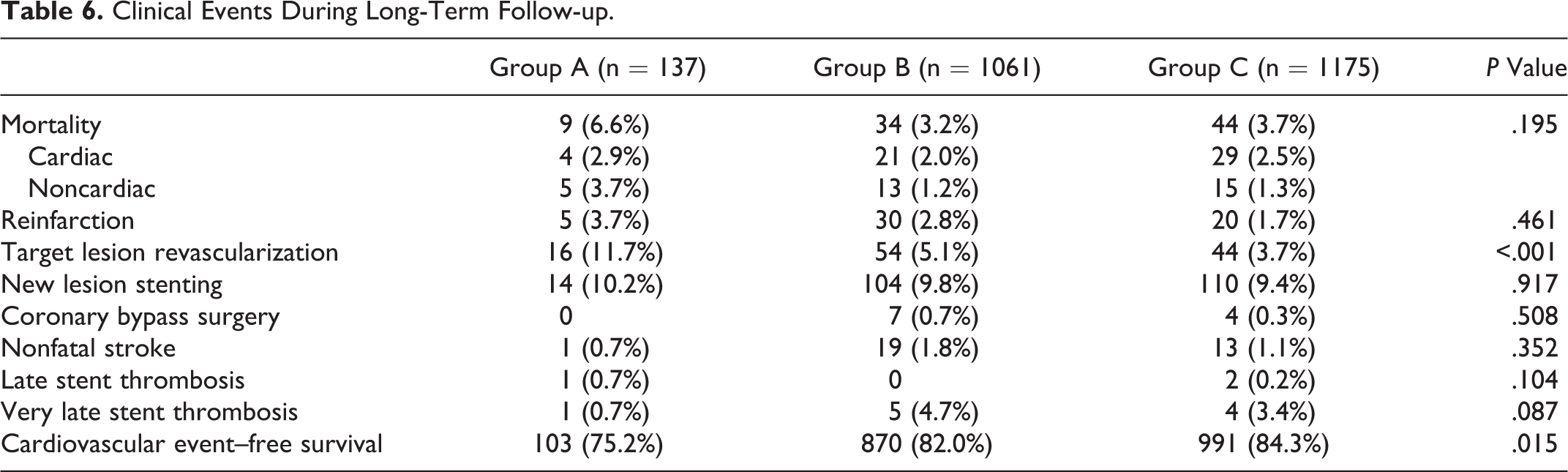
The long-term follow-up rates were 98%, 98%, and 97% for groups A, B, and C, respectively. There were no significant differences in the mortality rate, occurrence of reinfarction, appearance of new lesions requiring stenting, coronary bypass surgery, or nonfatal stroke during the follow-up period of 68 ± 59 months (median 48 months). However, group A had a higher rate of TLR than the other 2 groups (11.7%, 5.1%, and 3.7%, respectively; P < .001). One patient in group A and 2 patients in group C developed late stent thrombosis. Furthermore, 1 patient in group A, 5 patients in group B, and 4 patients in group C developed very late stent thrombosis. Group A had a lower cardiovascular event–free survival rate than the other 2 groups (75.2%, 82.0%, and 84.3%, respectively; P = .015; Table 6). The multivariable model considered 13 potential covariates as independent predictors of long-term outcomes: age > 55 years, gender, hypertension, diabetes mellitus, smoking, hyperlipidemia, family history of coronary artery disease, chronic kidney disease, old CVA, multivessel disease, left ventricular ejection fraction <40%, acute coronary syndrome, and generation of DES. The independent prognostic predictors of long-term cardiovascular events were diabetes mellitus (hazard ratio [HR]: 1.25; 95% confidence interval [CI]: 1.00-1.55; P = .046), multivessel disease (HR: 2.05; 95% CI: 1.59-2.64; P < .001), chronic kidney disease (HR: 1.63; 95% CI: 1.23-2.61; P = .001), vessel size: group C versus group A (HR: 0.66; 95% CI: 0.44-0.98; P = .04), and second-generation versus first-generation DES (HR: 0.61; 95% CI: 0.49-0.76; P < .001; Table 7). The long-term cardiovascular event–free survival curves based on a Cox regression model for patients who underwent first- or second-generation DES implantations in 3 vessel size groups showed that large vessel size and second-generation DES were associated with better outcomes than small vessel size and first-generation DES (P < .001; Figure 1).
Clinical Events During Long-Term Follow-up.
Multivariate Cox Proportional Hazard Analysis of Prognostic Factors for Long-Term Cardiovascular Events.
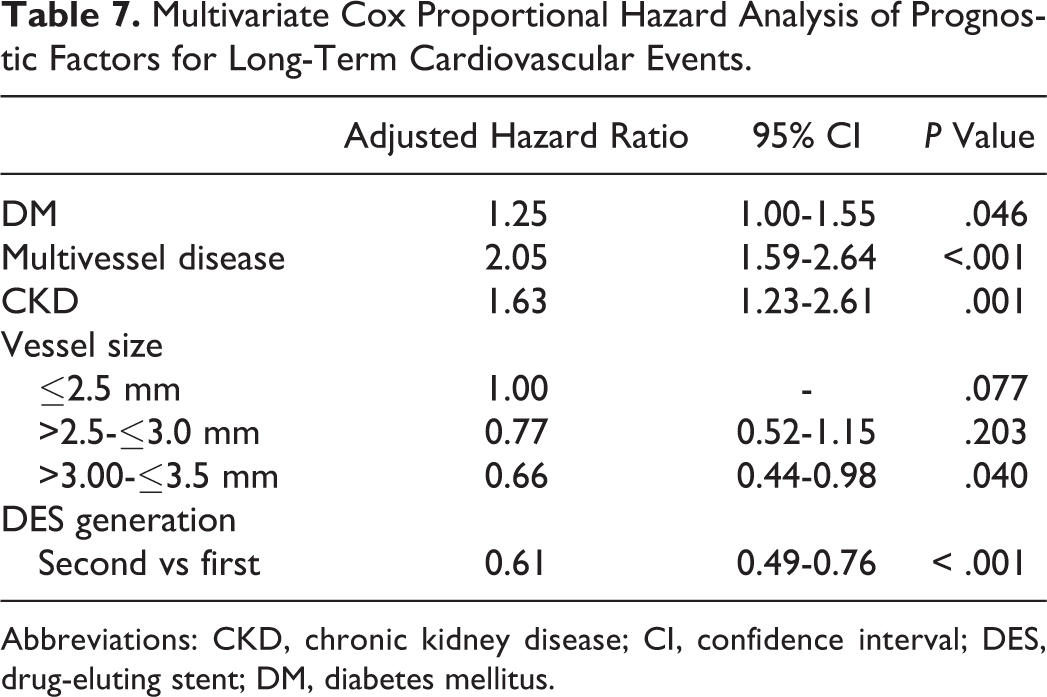
Abbreviations: CKD, chronic kidney disease; CI, confidence interval; DES, drug-eluting stent; DM, diabetes mellitus.
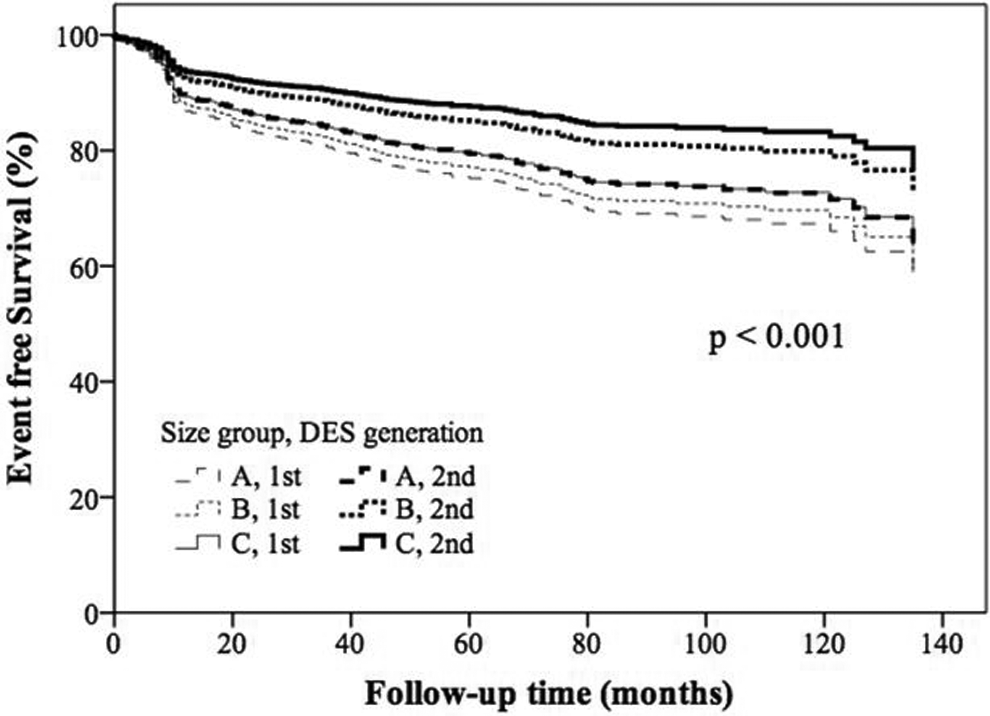
The adjusted long-term cardiovascular event–free survival curves according to the vessel size and generation of DES using Cox proportional hazards model.
Discussion
The major findings of this study are that the patients who received limus-based DES with vessels ≤2.5 mm were associated with (1) a higher incidence of diabetes mellitus and multivessel disease, (2) similar in-hospital results, (3) higher loss index and restenosis rate at 9-month angiographic follow-up, and (4) lower cardiovascular event–free survival rate during a very long-term follow-up period (68 ± 59 months) than the patients with larger vessels.
Previous studies have shown that vessel diameter is a factor determining long-term outcomes after PCIs with stenting and that a smaller vessel diameter is associated with a higher restenosis and cardiovascular event rate. 1 –3 Moreover, atherosclerotic coronary involvement often extends to small caliber and distal coronary arteries, and more than 30% of coronary interventions have been reported to involve small vessels. 10 In addition, previous studies have shown that the clinical outcomes of patients with DESs are not significantly different from those of patients with BMSs in large coronary arteries. 11,12 Therefore, in this study, we focused on medium and small diameter vessels and divided the patients into 3 subgroups according to the size of the currently available stents (≤2.5 mm, >2.5-≤3.0 mm, and >3.00-≤3.5 mm). A meta-analysis regarding small vessel (<3 mm) stenting reported that rates of restenosis and MACEs in patients with BMSs were 27.8% and 17.6%, respectively. 13 The inverse relationship between vessel diameter and restenosis after BMS implantation has been reported because even a small volume of neointimal hyperplasia can induce diameter stenosis of more than 50% in small vessels more easily than in large vessels. 14 The recent development of DESs has improved outcomes due to their potent antiproliferative effect and early and midterm safety in a broad spectrum of lesions, including lesions located in small coronary vessels. 15 Two randomized trials demonstrated that patients receiving SESs, 16,17 PESs, 18 and zotarolimus-eluting stents 19 had lower angiographic restenosis and MACE rates than patients receiving BMSs in the setting of small vessel stenting. Moreover, the inverse relationship between vessel size and angiographic restenosis rate in patients with BMS implantation may also be applicable to those with DESs. The Sirolimus-Eluting Stent in De-Novo Native Coronary Lesions (SIRIUS) study reported angiographic restenosis rates in large (>3.3 mm) and small (<2.3 mm) SES-treated vessels of 1.9% and 18.6%, respectively. 20 In the TAXUS-IV study, the 9-month restenosis rates for small (≤2.5 mm) and large (>3.5 mm) vessels were 8.8% and 5.5%, respectively. 21 However, new-generation DESs (everolimus-eluting stents) have shown conflicting results, with decreasing efficacy in neointimal proliferation regardless of vessel size. 22 Future studies regarding the inverse relationship between vessel size and outcomes/restenosis with new-generation DES implantation are needed to assess their efficacy.
Comparing first-generation DESs (SESs and PESs), the Sirolimus- and Paclitaxel-Eluting Stents for Small Vessels (ISAR-SMART) 3 trial of 360 patients with RVD <2.75 mm reported a significantly lower rate of restenosis (11.4% vs 19.0%; P = .047) and repeat revascularization (6.6% vs 14.7%; P = .008) in the SES group than in the PES group. 7 In addition, subgroup analysis of the SIRTAX trial evaluated 370 patients with RVD <2.75 mm and found a significantly lower MACE rate in the SES group compared with the PES group (10.4% vs 21.4%; P = .004). 8 Sirolimus-eluting stents have shown consistent advantages over PESs in both angiographic and clinical outcomes. Therefore, in this study, we evaluated only limus-based DES-treated vessels and excluded PES-treated vessels to allow for a more homogenous background. In addition, only limus-based DESs are currently available in daily practice around the world. Furthermore, we only enrolled patients with medium- and small-sized vessels (≤3.5 mm) and evaluated the relationship between vessel size and clinical outcomes during a very long-term follow-up period (68 ± 59 months), which, to the best of our knowledge, is the longest follow-up period reported to date. With both first- and second-generation limus-based DESs, an inverse relationship between vessel size and clinical outcomes was noted. The patients with smaller vessel stenting had higher percentage diameter stenosis and binary restenosis rate owing to equivalent late lumen loss as in patients with larger vessels, which translated into higher TLR and MACE rates. In addition, the frequency of diabetes in this study was higher in patients with small vessels than in those with large vessels, which is consistent with a report by Elezi et al 2 but in contrast to a report by Togni et al. 8
Limitations
There are several limitations to this single-center, prospective, observational study. First, this is a real-world registry, and the number of patients in the small vessel subgroup was relatively small. Furthermore, this was not a randomized comparison, which may have caused bias in the results, and therefore, our findings should be interpreted with caution. Second, we lacked routine intravascular ultrasound data, which is the most accurate method for measuring vessel diameter. Third, the follow-up angiographic data were not complete, although the follow-up rate was high (75%-80%).
Conclusion
An inverse relationship between medium or small vessel size (≤3.5 mm) and clinical outcomes was noted in patients receiving limus-based DESs, which was used exclusively in daily practice. Patients with smaller vessels (≤2.5 mm) had higher loss index and binary restenosis angiographically, which translated into higher TLR and MACE rates during a very long-term follow-up period. The outcomes of second-generation DES implantations were better than first-generation DES irrespective of vessel size.
Footnotes
Authors’ Note
Chang Gung Memorial Hospital, Research project, I-Chang Hsieh: CORPG3C0162.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.