
Abstract
Introduction:
Eccentric vessel wall enhancement (EVWE) and high-sensitivity C-reactive protein (hs-CRP) are inflammatory biomarkers associated with atherosclerotic disease. We investigated their prognostic value in patients with acute ischemic stroke receiving guideline-adherent medical treatment.
Patients and methods:
In this prospective observational cohort study, patients with acute ischemic stroke attributed to intracranial arterial disease (ICAD) underwent vessel wall MRI and hs-CRP testing. The study included intracranial cases of both large artery atherosclerosis (LAA) and small vessel occlusion (SVO). The primary outcome was subsequent ischemic stroke during the follow-up period. The median follow-up duration was 21 months. Kaplan-Meier survival and Cox regression analysis was used to determine the associations between EVWE, hs-CRP levels, and subsequent ischemic stroke.
Results:
Among 191 patients, 81 (42.4%) had EVWE. EVWE positivity showed a trend toward a lower risk of subsequent ischemic stroke compared to EVWE negativity (HR 0.32, 95% CI 0.12–0.87; p = 0.061). Hs-CRP levels were not associated with recurrent stroke risk. The combination of EVWE positivity and low hs-CRP levels (<1.25 mg/l) was associated with a favorable outcome, while EVWE negativity and high hs-CRP levels (⩾1.25 mg/l) were associated with an unfavorable outcome (HR 0.143, 95% CI 0.04–0.50; p = 0.031).
Discussion:
In this observational study of patients with intracranial atherosclerotic stroke receiving optimal medical therapy, EVWE positivity appeared to be associated with a trend toward lower risk of recurrent stroke, though this relationship requires further validation.
Conclusion:
The combination of EVWE and hs-CRP status might potentially offer prognostic information, with preliminary data suggesting that EVWE positivity and low hs-CRP levels could be associated with more favorable outcomes in patients receiving guideline-adherent medical treatment. These preliminary findings suggest a possible role for combining imaging and serum inflammatory biomarkers in risk stratification, though larger prospective studies are needed to confirm these associations.
Introduction
Inflammation plays a crucial role in the development of atherosclerosis, a major risk factor for acute ischemic stroke. Recent clinical trials, such as the COLCOT trial and LoDoCo2 trial, have demonstrated the significance of targeting inflammation in reducing cardiovascular events in patients with coronary artery disease.1,2 These studies highlight the potential benefits of anti-inflammatory therapies in the prevention and management of atherosclerotic diseases, including ischemic stroke.
Intracranial black blood vessel wall magnetic resonance imaging (VW-MRI) has emerged as a valuable tool in detecting inflammatory changes of the intracranial arteries.3,4 This imaging technique provides insights into the pathophysiology of acute ischemic stroke and may aid in identifying patients at higher risk for recurrent events. Typical VW-MRI findings of intracranial atherosclerotic disease (ICAD) plaques include focal and eccentric enhancement.5–7 In patients with recent stroke, this enhancement has been reported to be associated with the symptomatic status of the ICAD plaque. 3 However, the long-term clinical implications of ICAD enhancement remain largely unknown, particularly in the era of advanced medical management, which includes high-potency dual antiplatelet therapy and rigorous management of hypertension, diabetes mellitus, dyslipidemia and cigarette smoking.
High-sensitivity C-reactive protein (hsCRP), an another biomarker marker of inflammation, has been robustly associated with cardiovascular outcomes. A recent collaborative analysis of three randomized trials demonstrated that elevated hsCRP levels were predictive of cardiovascular events, even among patients receiving statin therapy. 8 This finding underscores the importance of considering inflammatory biomarkers in the risk stratification and management of patients with acute ischemic stroke.
Given the growing evidence supporting the role of inflammation in the pathogenesis and prognosis of cardiovascular events and acute ischemic stroke, the aim of this study is to evaluate the association between radiological (vessel wall enhancement) and serological (hs-CRP) biomarkers of inflammation and long-term cerebrovascular outcomes in patients with acute ischemic stroke attributed to intracranial atherosclerosis. In contrast to most previous cross-sectional studies on vessel wall enhancement, the current prospective study evaluated inflammatory biomarkers and followed up with acute ischemic stroke patients to assess their future cerebrovascular outcomes. By investigating the relationship between these biomarkers and clinical outcomes, we aim to provide insights into the prognostic value of inflammation in the context of acute ischemic stroke and inform future strategies for risk stratification and targeted interventions.
Methods
Ethical approval
This prospective observational cohort study was approved by the Institutional Review Board of The Catholic University of Korea (OC23RISI0149), and written informed consent was obtained from all participants or their legally authorized representatives prior to enrollment. The study adheres to the reporting guideline of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 9 All methods were carried out in accordance with relevant guidelines and regulations.
Study population and design
We enrolled consecutive patients who admitted to our hospital’s emergency department from November 2021 to October 2022 with acute ischemic stroke. Patients were classified according to the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) stroke classification criteria. 10 The study population comprised patients with acute ischemic stroke caused by intracranial arterial disease (ICAD), specifically those classified as either large artery atherosclerosis (LAA) or small vessel occlusion (SVO). We excluded patients with stroke caused by symptomatic extracranial carotid artery stenosis, cardioembolic stroke, or stroke of other determined or undetermined etiologies (including cases with multiple potential causes, negative workup, or incomplete evaluation). Additionally, patients who received intraarterial endovascular treatment were also excluded to eliminate the potential effect of post-procedural contrast enhancement on VW-MRI results. All participants underwent both vessel wall MRI and high-sensitivity C-reactive protein (hs-CRP) testing. They were then classified into subgroups based on the presence or absence of eccentric vessel wall enhancement (EVWE) or whether their hs-CRP levels were above or below the median value (1.25 mg/l).
Clinical data regarding age, sex, history of hypertension, diabetes mellitus (DM), dyslipidemia, previous ischemic or hemorrhagic stroke, coronary artery disease (CAD), congestive heart failure (CHF), and current cigarette-smoking status were obtained. All patients underwent detailed clinical evaluations, including neurological examinations, laboratory tests, chest radiography, 12-lead electrocardiography, 24-h Holter monitoring, echocardiography, MRI, and contrast-enhanced MR angiography or computed tomography (CT) angiography from the aortic arch to the intracranial vessels. Demographic, clinical, and neuroimaging data were collected for each participant at enrollment.
Black blood vessel wall MRI
All subjects underwent MRI scans, which included high-spatial resolution three-dimensional MRI with a black blood effect. The scans were acquired using a Siemens MAGNETOM Skyra 3 Tesla MRI scanner with a T1 SPACE (Sampling Perfection with Application optimized Contrasts using different flip angle Evolution) 3D fast spin-echo sequence. The imaging parameters were as follows: sagittal slice thickness, 0.9 mm; repetition time, 500 ms; echo time, 25 ms; flip angle, 120°; voxel size, 0.56 × 0.625 × 0.9 mm.
A neuroradiologist (S-H Kim) reviewed the patients’ vascular neuroimaging studies and confirmed the presence of eccentric vessel wall enhancement on VW-MRI in the vessel relevant to the index stroke (Figure 1).

Representative case of eccentric vessel wall enhancement (EVWE) in the left middle cerebral artery of a patient with acute ischemic stroke.
Primary exposure
In accordance with current stroke guidelines, all patients received aspirin and clopidogrel for at least 21 days, unless antithrombotic therapy was contraindicated due to complications such as active bleeding. 11 After this period, the decision to maintain monoantiplatelet or dual-antiplatelet therapy was at the discretion of the treating physician. All patients were treated with high-dose statin therapy, 12 and other vascular risk factors, such as hypertension and diabetes mellitus, were managed according to current guidelines. 12
Clinical outcomes
The primary outcome was a subsequent ischemic stroke during the follow-up period, defined as new or worsening neurological symptoms lasting for at least 24 h, or lasting less than 24 h but accompanied by imaging evidence of new or enlarging acute infarction in the territory of the affected artery.
Statistical analysis
Statistical analyses were performed using SPSS for Windows version 28.0 (IBM Corporation, Armonk, NY, USA). Values are expressed as mean ± standard deviation, median with interquartile range, or percentage.
Baseline characteristics were compared between patients with versus without EVWE using the chi-square test (or Fisher’s exact test) for categorical variables and the independent-samples t-test for continuous variables.
Kaplan-Meier survival analysis was used to assess the subsequent occurrence of ischemic stroke. Unadjusted and adjusted Cox proportional hazards regression models were used to determine the associations between EVWE, hs-CRP levels, and subsequent ischemic stroke. Models were adjusted for prespecified variables known or thought to potentially alter stroke risk and treatment choice, including age, diabetes, hypertension, dyslipidemia, prior stroke, coronary artery disease, active smoking, and chronic kidney disease.
Exploratory subgroup analyses compared ischemic stroke risk between patients with EVWE+ and hs-CRP < 1.25 mg/l versus those with EVWE− and hs-CRP ⩾ 1.25 mg/l. Baseline characteristics were compared between these subgroups using chi-square tests (or Fisher’s exact test) for categorical variables and t-tests for continuous variables.
Two-sided p-values <0.05 were considered statistically significant.
Results
Baseline characteristics
A total of 191 patients with acute non-cardioembolic ischemic stroke who underwent black blood vessel wall MRI were included in the analysis (Figure 2). Of these, 81 (42.4%) had EVWE+ on MRI, while 110 (57.6%) did not (EVWE−). The baseline demographic and clinical characteristics of the two groups were generally similar (Table 1). The mean and median hs-CRP levels were also comparable between the two groups (p = 0.945 and 0.649, respectively). The TOAST classification showed differences between groups, with LAA predominating in the EVWE+ group and SVO being more prevalent in the EVWE- group (p = 0.013). Within the LAA subgroup, 51.6% (n = 50) of patients demonstrated symptomatic EVWE+, while 48.5% (n = 47) showed no enhancement. Notably, in the SVO subgroup, although 67.0% (n = 63) of patients had no EVWE+, a substantial proportion, 33.0% (n = 31), demonstrated focal enhancement without any stenosis. Among patients with EVWE+, the middle cerebral artery (MCA) was most frequently affected (45.7%, n = 37), followed by the basilar artery (29.3%, n = 24), posterior cerebral artery (PCA; 14.8%, n = 12), anterior cerebral artery (ACA; 4.9%, n = 4), vertebral artery (2.5%, n = 2), and distal internal carotid artery (ICA; 2.5%, n = 2).
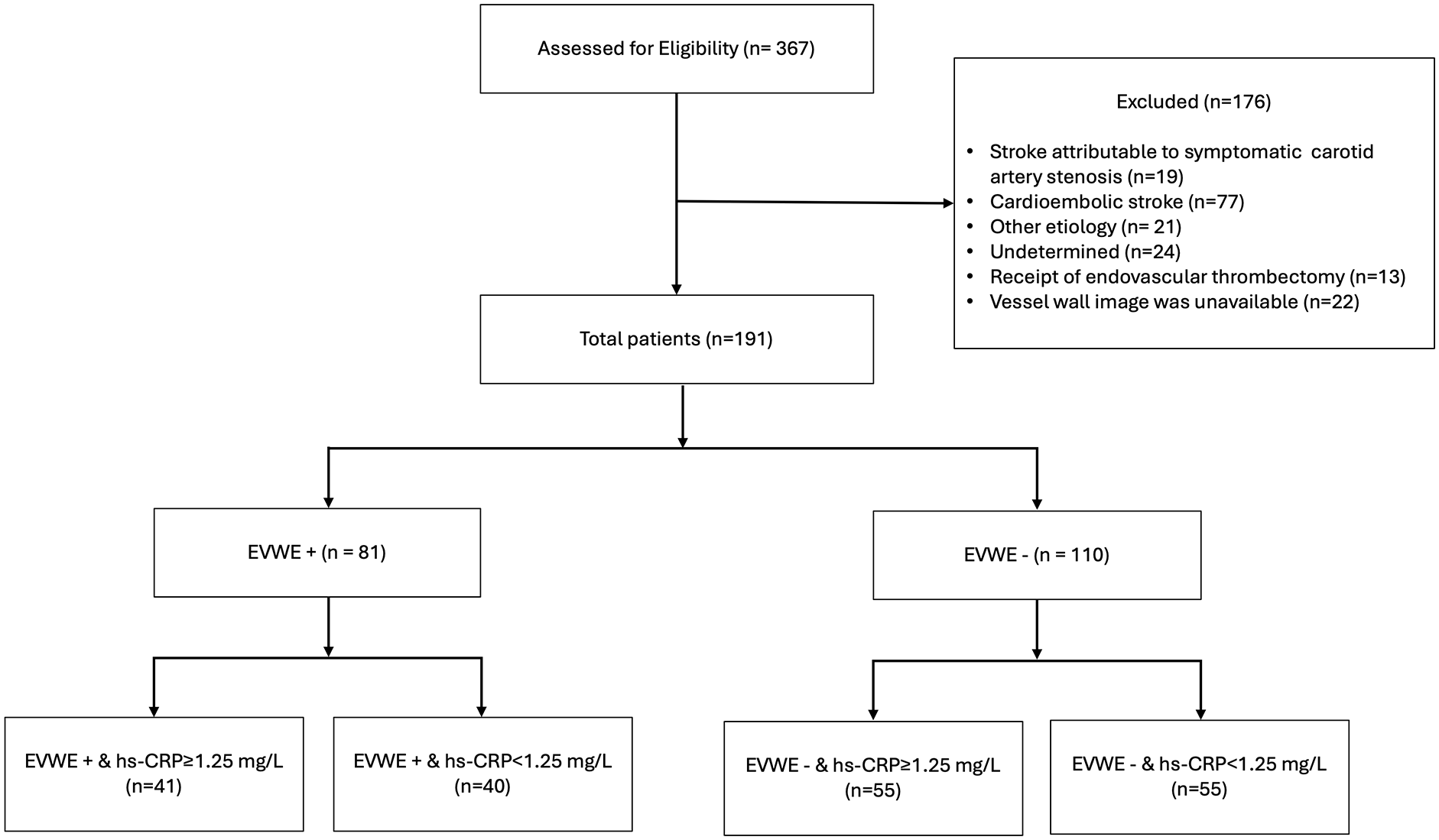
Flow diagram of patient selection and enrollment. Abbreviations: EVWE, eccentric vessel wall enhancement; hs-CRP, high-sensitivity C-reactive protein.
Baseline demographic and clinical characteristics of patients with acute ischemic stroke, comparing those with and without eccentric vessel wall enhancement.

Abbreviations: NIHSS: National Institutes of Health Stroke Scale; hs-CRP: high-sensitivity C-reactive protein; IQR: Interquartile range; DAPT: dual antiplatelet therapy; TOAST: Trial of ORG 10172 in Acute Stroke Treatment; LAA: large artery atherosclerosis; SVO: small vessel occlusion.
Values are presented as mean ± standard deviation or number (%). Chi-square test or Fisher’s exact test was used for categorical variables, and independent-samples t-test was used for continuous variables.
Atrial fibrillation: past history or diagnosed during admission.
Lipid profiles were reassessed between 6 months and 1 year after the index stroke.
p < 0.05 **p < 0.01.
The prevalence of EVWE+ varied across different arterial territories with LAA. Basilar artery LAA showed the highest proportion at 83.3% (n = 15 of 18), followed by ACA at 80% (n = 4 of 5), MCA at 54.1% (n = 20 of 37), and PCA at 50% (n = 6 of 12). The lowest rates of EVWE+ were observed in the vertebral artery at 25% (n = 3 of 12) and distal ICA at 37.5% (n = 3 of 8).
All patients in both the EVWE+ and EVWE- groups received statin therapy (100% compliance in each group). Among the total cohort, lipid profiles were reassessed in 159 patients between 6 months and 1 year after the index stroke. Under statin treatment, mean LDL levels were 60.9 ± 25.0 mg/dl in the EVWE+ group and 62.5 ± 25.7 mg/dl in the EVWE- group (p = 0.693). DAPT treatment was administered to 75 (92.6%) patients in the EVWE+ group and 105 (95.5%) patients in the EVWE- group, with no difference between the groups (p = 0.532). The median duration of DAPT was 69 days (IQR 26–140) in the EVWE+ group and 60 days (IQR 30–128.25) in the EVWE− group.
During follow-up, 16 patients experienced recurrent ischemic stroke. The recurrence rate was lower in patients with EVWE+ at 3.7% (n = 3) compared to 11.8% (n = 13) in those with EVWE−. Among patients with LAA who had recurrent stroke, recurrence in the same symptomatic vessel as the index stroke occurred in 33.3% (n = 3) of EVWE- patients (n = 9) compared to 66.7% (n = 2) of EVWE+ patients (n = 3).
A supplementary analysis was conducted to directly compare the baseline characteristics of patients with EVWE+ and hs-CRP < 1.25 mg/l (n = 40) to those with EVWE− and hs-CRP ⩾ 1.25 mg/l (n = 55; Supplemental Table). No differences were found in age, sex, hypertension, diabetes, dyslipidemia, history of stroke, coronary artery disease, chronic kidney disease, active cigarette smoking, atrial fibrillation, follow-up duration, DAPT treatment, or DAPT duration between the two groups (all p > 0.05). The TOAST classification also did not differ between the groups (p = 0.094).
Association between EVWE, hs-CRP, and ischemic stroke
Kaplan-Meier survival analysis showed a trend toward a lower risk of subsequent ischemic stroke in the EVWE+ group compared to the EVWE- group, although this did not reach statistical significance (HR 0.32, 95% CI 0.12–0.87; p = 0.061; Figure 3). When stratified by hs-CRP levels, patients with hs-CRP ⩾ 1.25 mg/l had a higher risk of subsequent ischemic stroke compared to those with hs-CRP < 1.25 mg/l, but this association was also not statistically significant (HR 2.31, 95% CI 0.87–6.16; p = 0.108).
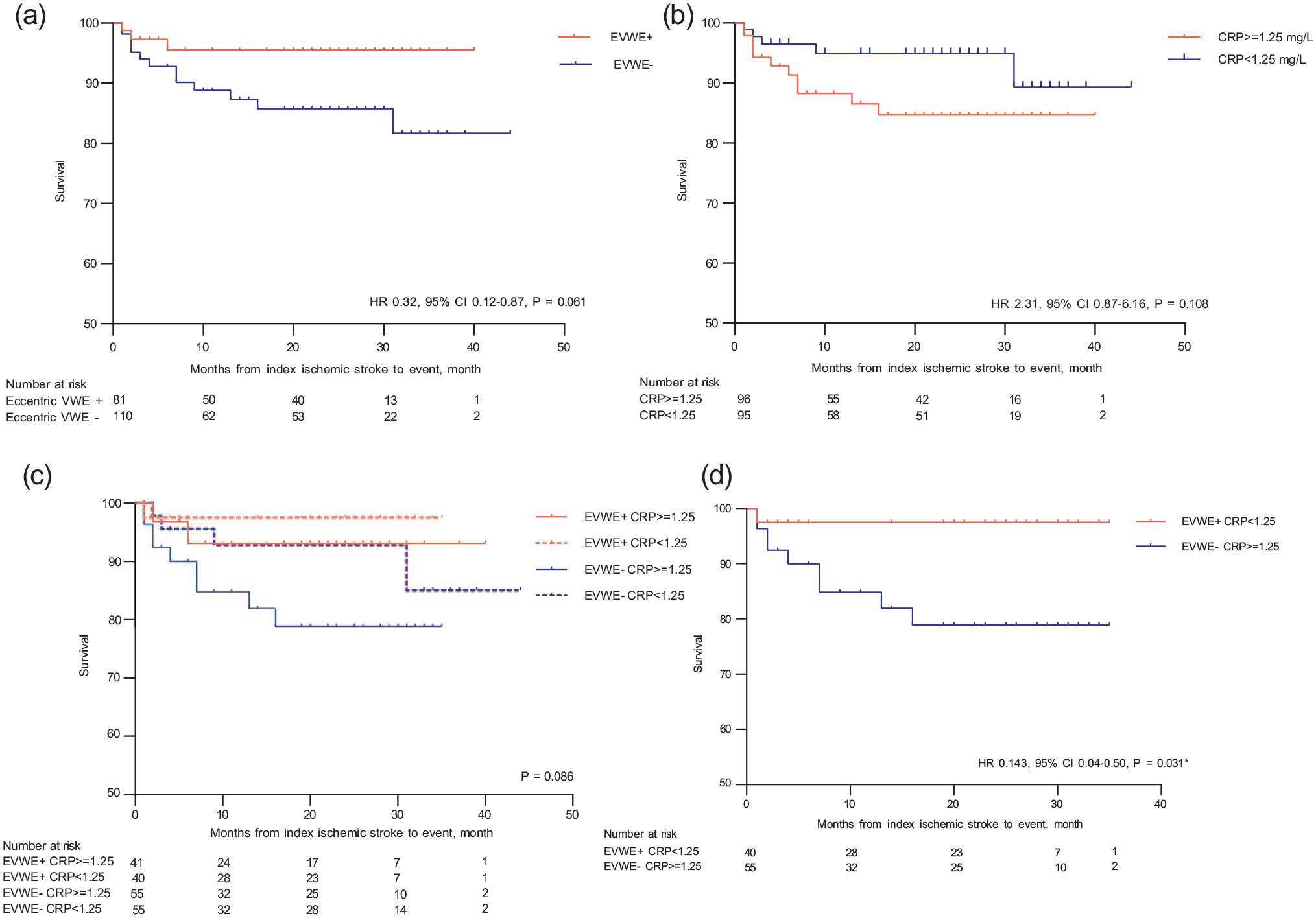
Kaplan-Meier survival estimates of subsequent ischemic stroke: (a) comparison between patients with and without eccentric vessel wall enhancement (EVWE), (b) comparison between patients with high (⩾1.25 mg/l) versus low (<1.25 mg/l) C-reactive protein (CRP) levels, (c) four-group comparison based on combinations of EVWE status and CRP levels, and (d) direct comparison between patients with EVWE+ and CRP < 1.25 mg/l versus EVWE− and CRP ⩾ 1.25 mg/l.
The combination of EVWE and hs-CRP status was further analyzed. Patients with EVWE+ and hs-CRP < 1.25 mg/l had a lower risk of subsequent ischemic stroke compared to those with EVWE− and hs-CRP ⩾ 1.25 mg/l (HR 0.143, 95% CI 0.04–0.50; p = 0.031).
Cox regression analysis was performed to assess the association between EVWE, hs-CRP levels, and ischemic stroke (Table 2). In the unadjusted model, EVWE+ showed a trend toward a lower risk of ischemic stroke compared to EVWE− (HR 0.32, 95% CI 0.09–1.13; p = 0.076). Hs-CRP levels ⩾ 1.25 and ⩾2 mg/l were not associated with ischemic stroke risk (p = 0.120 and p = 0.410, respectively). The combination of EVWE+ and hs-CRP < 1.25 mg/l was associated with a lower risk of ischemic stroke compared to EVWE− and hs-CRP ⩾ 1.25 mg/l, although this did not reach statistical significance in the unadjusted model (HR 0.14, 95% CI 0.02–1.13; p = 0.065).
Association between eccentric vessel wall enhancement, C-reactive protein levels, and subsequent ischemic stroke: unadjusted and adjusted Cox regression analysis.

Abbreviations: EVWE: eccentric vessel wall enhancement; hs-CRP, high-sensitivity C-reactive protein.
Model 1:adjusted by age and diabetes mellitus.
Model 2: Model 1 + adjusted by hypertension, dyslipidemia, prior stroke, coronary artery disease, active cigarette smoking, and chronic kidney disease.
After adjusting for age and diabetes (Model 1) and further adjusting for hypertension, dyslipidemia, stroke, coronary artery disease, active cigarette smoking, and chronic kidney disease (Model 2), the associations remained similar, with HRs for EVWE+, hs-CRP ⩾ 1.25, and hs-CRP ⩾ 2 mg/l of 0.32 (95% CI 0.09–1.15; p = 0.080), 2.05 (95% CI 0.68–6.21; p = 0.206), and 1.26 (95% CI 0.45–3.51; p = 0.664), respectively. The combination of EVWE+ and hs-CRP < 1.25 mg/l remained associated with a lower risk of ischemic stroke compared to EVWE- and hs-CRP ⩾ 1.25 mg/l in both adjusted models, although not statistically significant (Model 1: HR 0.14, 95% CI 0.02–1.12; p = 0.063; Model 2: HR 0.13, 95% CI 0.02–1.15; p = 0.067).
Discussion
In this study, we investigated the association between two inflammatory biomarkers, EVWE on MRI and serum hs-CRP levels, and the risk of subsequent ischemic stroke in patients with acute ischemic stroke due to intracranial LAA or SVO who received guideline-adherent medical treatment. Our results suggest that the presence of EVWE, paradoxically, showed a trend toward a lower risk of recurrent ischemic stroke, although this did not reach statistical significance. In our study population, hs-CRP levels were neither associated with EVWE nor with an increased risk of subsequent ischemic stroke. However, the combination of EVWE positivity and low hs-CRP levels was associated with a favorable outcome compared to the combination of EVWE negativity and high hs-CRP levels.
Previous studies have reported that EVWE on high-resolution vessel wall MRI is associated with the symptomatic status of ICAD plaques in patients with recent stroke.4,6,7 The underlying pathophysiologic mechanism of EVWE is thought to involve the accumulation of gadolinium-based contrast agents in the neovascularization and increased endothelial permeability of the atherosclerotic plaque, which are features of plaque vulnerability and inflammation.13,14 These findings suggest that EVWE may be a marker of plaque instability and increased risk of future cerebrovascular events. In addition to its prognostic value, EVWE has been shown to have diagnostic utility in differentiating ICAD from other intracranial vasculopathies, such as moyamoya disease, vasculitis, and reversible cerebral vasoconstriction syndrome.6,15 Thus, the presence of EVWE may guide the selection of patients who could benefit from more aggressive antithrombotic therapy or novel anti-inflammatory treatments. In our study, EVWE positivity was associated with a trend toward lower risk of recurrent stroke. This observation suggests that EVWE status might help identify patients who respond differently to optimal medical therapy. Our results highlight the importance of considering the interaction between imaging biomarkers and treatment strategies when assessing the prognostic value of EVWE in patients with acute ischemic stroke.
Among patients with large artery atherosclerosis (LAA) who experienced recurrent stroke, recurrence in the territory of the initial symptomatic vessel was more frequent in those with positive vessel wall enhancement (EVWE+) than in those without enhancement (EVWE−). While the small number of recurrent events precludes definitive mechanistic conclusions, these findings reaffirm that EVWE+ may not only identify culprit intracranial atherosclerotic lesions but also predict their potential for future events.
Regarding hs-CRP, previous studies have demonstrated that elevated hs-CRP levels are associated with an increased risk of cardiovascular events, even among patients receiving statin therapy. 8 Hs-CRP is an acute-phase reactant produced by the liver in response to inflammatory cytokines, such as interleukin-6 and tumor necrosis factor-alpha, which are released in the context of atherosclerosis and other inflammatory conditions. 16 Elevated hs-CRP levels reflect the presence of systemic inflammation and have been shown to predict the risk of future cardiovascular events, including ischemic stroke, independently of traditional risk factors.17,18 Moreover, hs-CRP has been implicated in the pathogenesis of atherosclerosis through various mechanisms, such as endothelial dysfunction, monocyte recruitment, and platelet activation.19,20 These findings suggest that hs-CRP is not merely a biomarker of inflammation but may also actively contribute to the development and progression of atherosclerotic disease. However, in our study, hs-CRP levels were not associated with an increased risk of subsequent ischemic stroke. This finding is in contrast with the results of previous studies and may be attributed to several factors. First, our study population consisted of patients who received optimal medical management, including high-dose statin therapy, which has been shown to reduce hs-CRP levels and may have attenuated the association between hs-CRP and recurrent stroke risk. 21 Second, the relatively small sample size and low number of recurrent stroke events in our study may have limited our ability to detect an association between hs-CRP and clinical outcomes.
Although we found no association between hs-CRP and recurrent stroke risk, the combination of EVWE and hs-CRP status appeared to provide prognostic information. Patients with EVWE positivity and low hs-CRP levels had a favorable outcome, while those with EVWE negativity and high hs-CRP levels had an unfavorable outcome. This finding suggests that the integration of imaging and serum biomarkers of inflammation may offer a more comprehensive assessment of risk in patients with acute ischemic stroke.
Interestingly, contrary to our expectation, EVWE was not associated with hs-CRP levels in our study population. This finding suggests that EVWE and hs-CRP may reflect different aspects of the inflammatory process in the pathogenesis of ischemic stroke. One possible explanation for the lack of association between EVWE and hs-CRP is that EVWE may represent a localized inflammatory response within the intracranial vessel wall, while hs-CRP reflects systemic inflammation. 22 The presence of EVWE may indicate the vulnerability of an atherosclerotic plaque, which can be influenced by local factors such as shear stress, endothelial dysfunction, and the accumulation of inflammatory cells. 23 In contrast, hs-CRP levels are determined by the overall inflammatory burden in the body, which can be affected by various conditions, including obesity, smoking, and chronic infections. 24 Therefore, the dissociation between EVWE and hs-CRP suggests that local and systemic inflammation may have distinct roles in the development and progression of ischemic stroke.
The clinical implication of this finding is that the combined assessment of EVWE and hs-CRP may provide a more comprehensive evaluation of the inflammatory status in patients with acute ischemic stroke. The presence of EVWE, even in the absence of elevated hs-CRP, may identify patients with vulnerable intracranial plaques who could benefit from targeted interventions, such as intensive antithrombotic therapy or plaque-stabilizing agents. 25 Conversely, elevated hs-CRP levels, regardless of EVWE status, may indicate the need for systemic anti-inflammatory treatments to reduce the risk of recurrent stroke and other cardiovascular events. 26 Further research is needed to elucidate the complex interplay between local and systemic inflammation in the pathogenesis of ischemic stroke and to develop personalized treatment strategies based on the individual inflammatory profile.
Our study has several limitations. First, the sample size was relatively small, and the number of recurrent ischemic stroke events was low, which may have limited our ability to detect associations between the inflammatory biomarkers and clinical outcomes. A key limitation of our study was the insufficient statistical power to definitively assess the relationship between hs-CRP levels and stroke recurrence. While elevated hs-CRP (⩾1.25 mg/l) showed a trend toward increased stroke risk (HR 2.31), the wide confidence intervals (95% CI 0.87–6.16) and borderline significance (p = 0.108) suggest the study was underpowered to detect this association reliably. This limitation persisted in adjusted analyses, with hazard ratios remaining similar but confidence intervals consistently crossing unity. The relatively modest sample size (n = 191), low event rate, and median follow-up of 21 months likely contributed to this limited statistical power. Future studies with larger cohorts and longer follow-up periods would be needed to definitively establish the prognostic value of hs-CRP in this patient population. Second, we did not assess the dynamic changes in EVWE and hs-CRP levels over time, which may provide additional prognostic information. Third, all participants in our study received the most optimal medical treatment, which may have influenced the observed associations between the inflammatory biomarkers and clinical outcomes. As a result, we could not determine the pure effect of EVWE or hs-CRP on the risk of recurrent ischemic stroke in the absence of medical treatment.
In conclusion, our study suggests that EVWE positivity might potentially identify a subset of patients with acute ischemic stroke who could respond differently to intensive medical therapy. While previous studies have shown associations between hs-CRP levels and stroke outcomes, hs-CRP levels were not associated with an increased risk of recurrent ischemic stroke in our population. However, the observation that the combination of EVWE and hs-CRP status might provide prognostic information warrants further exploration, particularly the potential association between EVWE positivity combined with low hs-CRP levels and more favorable outcomes. These preliminary findings suggest a possible role for combining imaging and serum biomarkers of inflammation in risk stratification. Further large-scale, prospective studies are warranted to validate these results and explore the role of personalized treatment strategies based on the individual inflammatory profile.
Supplemental Material
sj-docx-1-eso-10.1177_23969873251317341 – Supplemental material for Vessel wall enhancement and high-sensitivity CRP as prognostic markers in intracranial atherosclerotic stroke: A prospective cohort study
Supplemental material, sj-docx-1-eso-10.1177_23969873251317341 for Vessel wall enhancement and high-sensitivity CRP as prognostic markers in intracranial atherosclerotic stroke: A prospective cohort study by Seunghee Na, Taewon Kim, Jaseong Koo, Yun Jeong Hong and Seong-Hoon Kim in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional committee and the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
Written informed consent was obtained from all patients or their representatives.
Guarantor
TK
Contributorship
T.K. contributed to conceptualization, methodology and data curation. J.K., Y.J.H., and S.H.K contributed to investigation. S.N., T.K. contributed to writing – original draft preparation and review & editing.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available to protect participant privacy but are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.