
Abstract
Morel-Lavallee lesions (MLLs) are traumatic closed degloving injuries with operative intervention (OI), especially excisional debridement, remaining the mainstay of treatment. However, high-quality evidence describing operative techniques and outcomes remains limited. This study aimed to characterize current OI practices and associated outcomes, especially among patients undergoing excisional debridement, hypothesizing an increased risk of wound complications with this approach for MLLs.
Methods
This prospective (2021-2024), multicenter, observational study was conducted across 15 trauma centers and included patients diagnosed with MLL who underwent OI. The association between operative technique (eg, excisional debridement) and the primary outcome of wound complications was evaluated. Wound complications were defined as cellulitis, deep wound infection, skin necrosis, necrotizing soft tissue infection (NSTI), and/or organized hematoma.
Results
Of 88 MLL patients undergoing OI, 36 (40.9%) had excisional debridement, with 4 (11.1%) limited excision to skin, 20 (55.6%) extended to subcutaneous tissue, and 12 (33.3%) down to muscle. Excisional debridement had higher rates of skin necrosis (22.2% vs. 1.9%, P = .002). Although overall rates of wound complications were statistically similar between cohorts (33.3% vs. 17.3%, P = .098), univariate analysis demonstrated excisional debridement had increased risk of wound complications (OR 2.52, CI 1.07-5.97, P = .035).
Conclusion
This prospective multicenter study over three years demonstrated that a fifth of MLLs undergoing excisional debridement developed postoperative skin necrosis. Excisional debridement also had a more than two-fold increased risk of wound complications compared to other OIs. These findings underscore the importance of investigating alternative operative techniques, such as incision and drainage or minimally invasive debridement methods.
Keywords
Introduction
Morel-Lavallee lesions (MLLs) are uncommon closed degloving injuries that occur from blunt trauma. This injury pattern was initially observed and described by a French surgeon named Maurice Morel-Lavallee in 1853. 1 MLLs result from shearing forces that detach subcutaneous tissue from the underlying fascia, leading to disruption of local microvascular and lymphatic networks and persistent fluid collections if left untreated. 2 Although considered infrequent, MLLs may accompany high-energy trauma in a meaningful minority of patients, which contributes to their clinical relevance for trauma providers. 3 In polytrauma patients, diagnosis may be delayed or initially overlooked since early management of these patients appropriately prioritizes other immediately life-threatening injuries.
Treatment strategies for MLLs remain heterogenous; however, operative management remains the primary approach, especially in lesions with threatened skin and soft tissue viability, anatomic regions not amenable to compression, and large or recurrent MLLs.1–5 Surgical intervention is oftentimes performed concurrently with other necessary operations, such as exploratory laparotomy for concomitant hollow viscus injury or internal fixation of underlying fractures.6,7 Some injuries have soft tissue devitalization requiring extensive excisional debridement; however, this poses additional risks for wound healing and wound-related complications compared to incision and drainage of MLLs. 1 Reported complications include cellulitis, deep wound infection, skin necrosis, necrotizing soft tissue infection (NSTI), and organized hematomas.1–3
Despite frequent surgical intervention for MLLs, postoperative outcomes remain poorly characterized as the majority of studies are small case series and undoubtedly reflect publication bias. 3 Given the variability in clinical presentation, the range of surgical techniques used, and the potential for impaired perfusion, a clearer understanding of postoperative outcomes is important for guiding decision making. Specifically, there is a paucity of high-quality data comparing the postoperative risk profile of excisional debridement to other surgical interventions for MLLs, such as incision and drainage or minimally invasive approaches.1–5
To address this knowledge gap, this prospective multicenter study aimed to describe existing operative management paradigms and associated outcomes, especially in those undergoing excisional debridement of MLLs, hypothesizing increased risk of wound complications in patients undergoing excisional debridement of MLLs.
Methods
This was a prospective, multicenter observational study (2021 to 2024) conducted at 15 Level-I trauma centers across the United States.8,9 Institutional review board approval was obtained at each site, with a waiver of consent granted due to the observational methodology of this study. Eligible participants included adult patients (≥18 years old) with MLLs diagnosed clinically and/or supported when available by CT, ultrasound, or MRI, and who underwent operative intervention. CT findings suggestive of acute MLLs include heterogenous fluid collections between the subcutaneous tissue and underlying fascia, oftentimes without well-defined margins. Exclusion criteria included patients with open wounds, pregnancy, or incarceration. This study design and reporting followed the EQUATOR Network Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 10
Primary and Secondary Outcomes
The primary outcome was incidence of wound complications, defined as cellulitis, deep wound infection, skin necrosis, NSTI, and/or organized hematoma. Cellulitis was defined as localized erythematous skin inflammation accompanied by warmth, tenderness, and/or edema related to bacterial infection. Deep wound infection was defined as the presence of abscess or purulence within the wound soft tissues. Skin necrosis was defined as irreversible death of the skin, oftentimes characterized by a dusky or black discoloration. NSTI was defined as a rapidly progressive soft tissue infection with clinical evidence of tissue necrosis. Organized hematoma was defined as a well encapsulated collection of chronic blood products. All complications were diagnosed clinically and/or with adjunct laboratory and imaging studies by the treating trauma team. Only complications that developed during hospitalization were included and conditions that were present on arrival, such as skin necrosis, were excluded. Patients who underwent excisional debridement to any level (skin, subcutaneous tissue, or muscle) were compared to those who underwent other operative interventions, including incision and drainage and minimally invasive (laparoscopic or endoscopic) debridement techniques. The secondary outcome was hospital length of stay (LOS).
Additional Data Collected
Demographic variables collected included sex, age, comorbidities, Charlson Comorbidity Index, body mass index (BMI), and pre-injury antiplatelet or anticoagulation medication use. Clinical data included vitals on arrival, Glasgow Coma Scale (GCS), mechanism of injury, injury severity score (ISS), and abbreviated injury scale (AIS) regional scores.
MLL-specific data including anatomic location of MLL (thigh, flank/lumbar, hip, pelvis, knee, shin or calf, abdomen, shoulder, elbow) and physical exam findings including ecchymosis or discoloration, circumferential involvement, and skin viability. Operative details included maximal depth of excisional debridement (skin vs subcutaneous vs muscle), use of a pulse irrigator, closure of dead space, use of negative pressure wound therapy (NPWT), and wound closure method. Additional outcomes data collected included intensive care unit (ICU) LOS, ventilator days, and discharge disposition.
Statistical Analysis
Patients who underwent excisional debridement were compared to those who underwent other surgical interventions. Categorical variables were summarized as frequencies and percentages, while continuous and ordinal data were displayed as medians with interquartile range. Chi-square was used for categorial variables and Mann-Whitney-U for continuous and ordinal variables. A multivariable analysis was not performed because the sample size and number of events were insufficient to support a reliable adjusted model. Univariable logistic regression was performed to evaluate the risk of wound complications in patients with MLLs undergoing excisional debridement. This risk was reported as an odds ratio (OR) with 95% confidence intervals (CI). Statistical significance was defined as P < .05 (two-tailed). All analyses were performed using IBM SPSS Statistics (Version 29, IBM Corp., Armonk, NY).
Results
Demographics and Comorbidities of MLL Patients Undergoing Excisional Debridement Versus Other Operative Interventions
Demographics and Comorbidities of Morel-Lavallee Lesion Patients Undergoing Excisional Debridement Versus Other Surgical Intervention
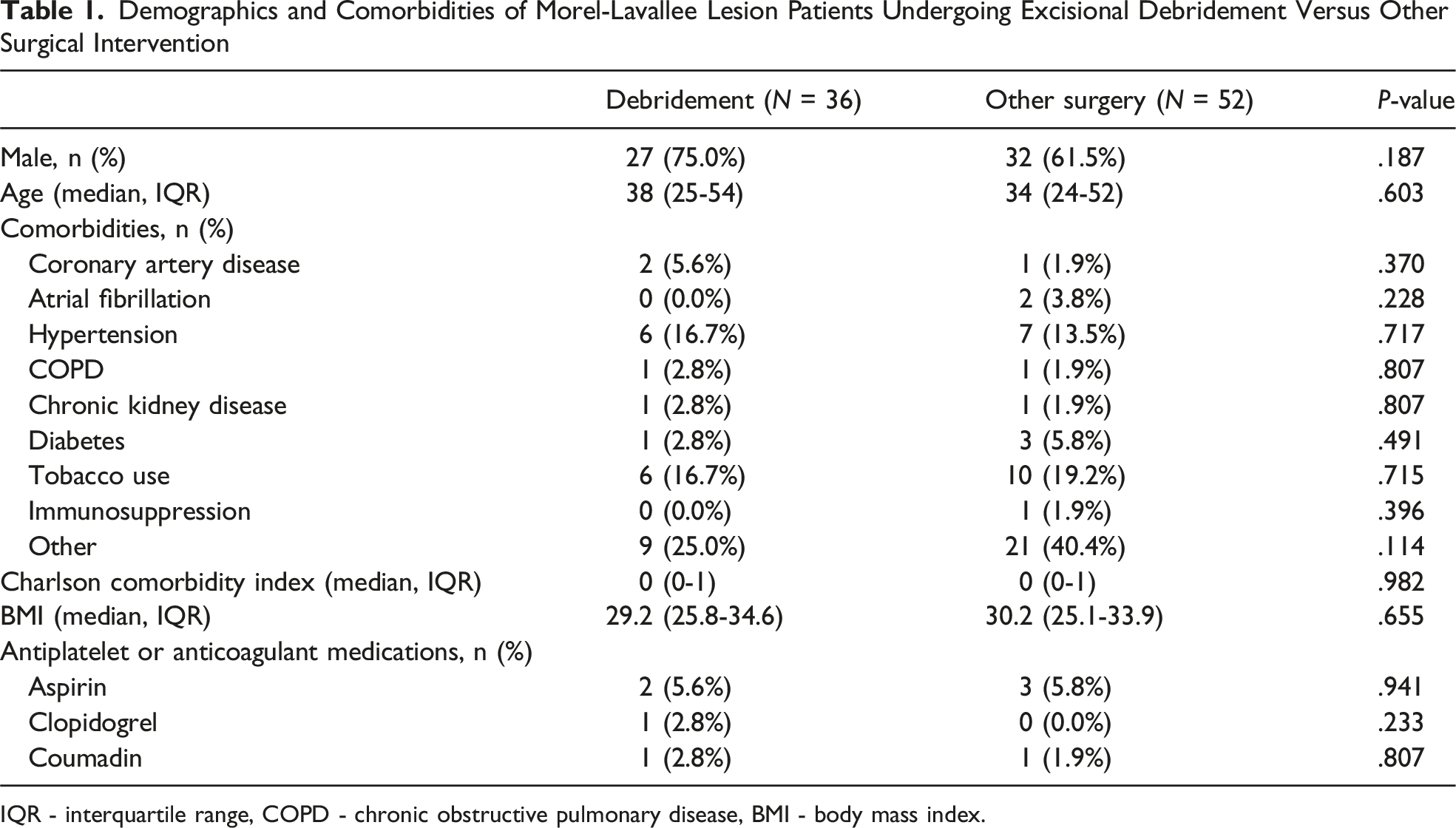
IQR - interquartile range, COPD - chronic obstructive pulmonary disease, BMI - body mass index.
Vital Signs, Injury Profiles, and MLL Locations for MLL Patients Undergoing Excisional Debridement Versus Other Operative Intervention
Vital Signs and Injury Profiles for Morel-Lavallee Lesion Patients Undergoing Excisional Debridement Versus Other Surgical Intervention
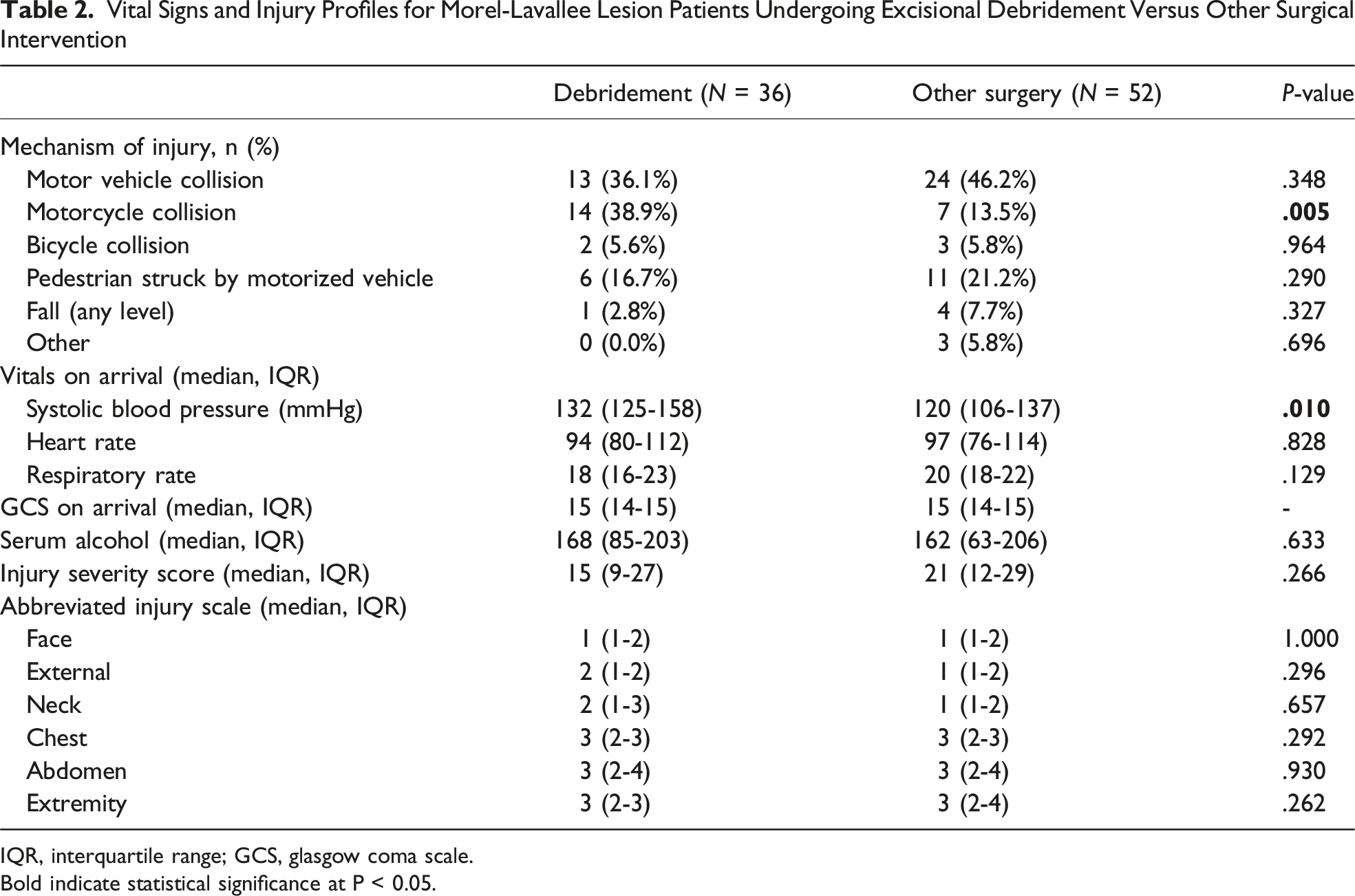
IQR, interquartile range; GCS, glasgow coma scale.
Bold indicate statistical significance at P < 0.05.
Wound Characteristics of Morel-Lavallee Lesion Patients Undergoing Excisional Debridement Versus Other Surgical Intervention
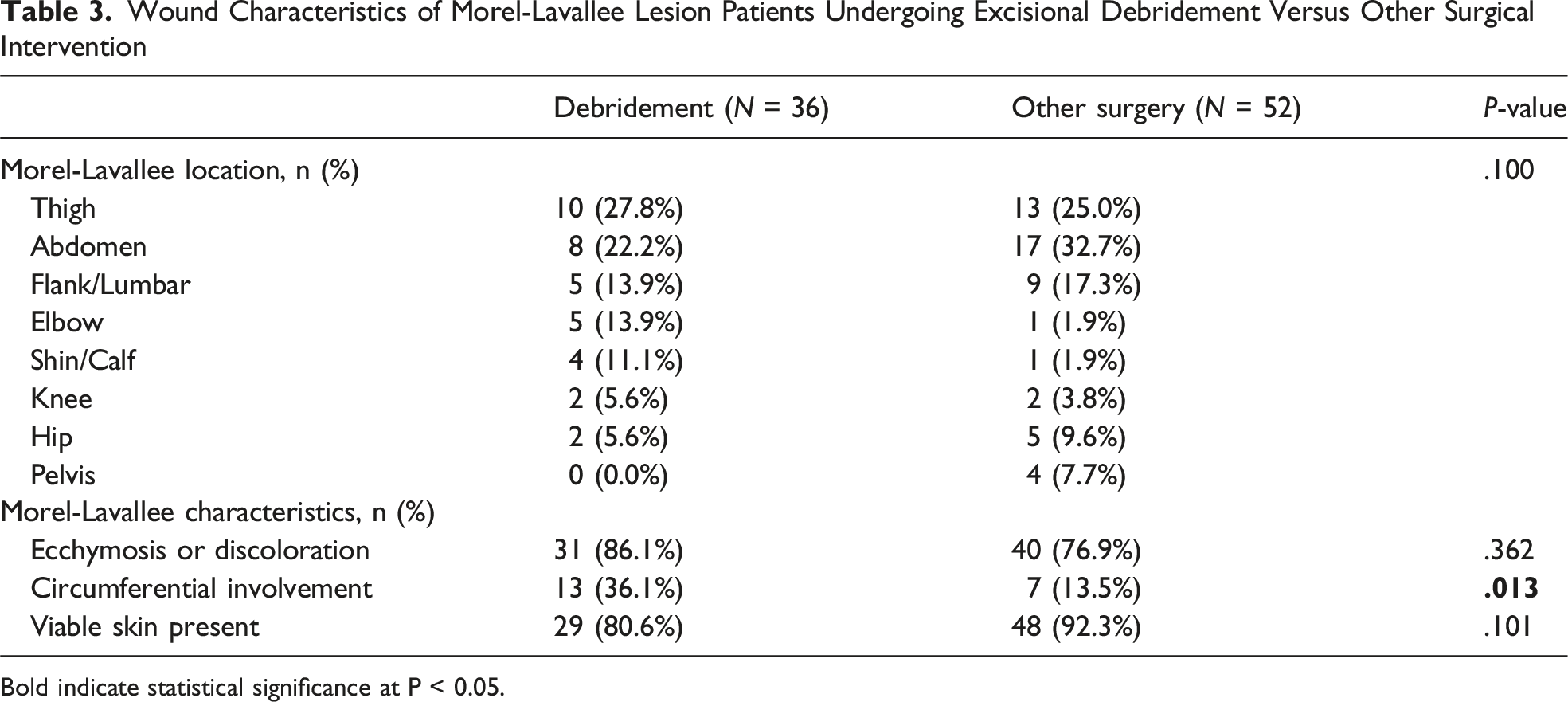
Bold indicate statistical significance at P < 0.05.
Operative Details for MLL Patients Undergoing Excisional Debridement Versus Other Operative Intervention
Operative Details for Morel-Lavallee Lesion Patients Undergoing Excisional Debridement Versus Other Surgical Intervention
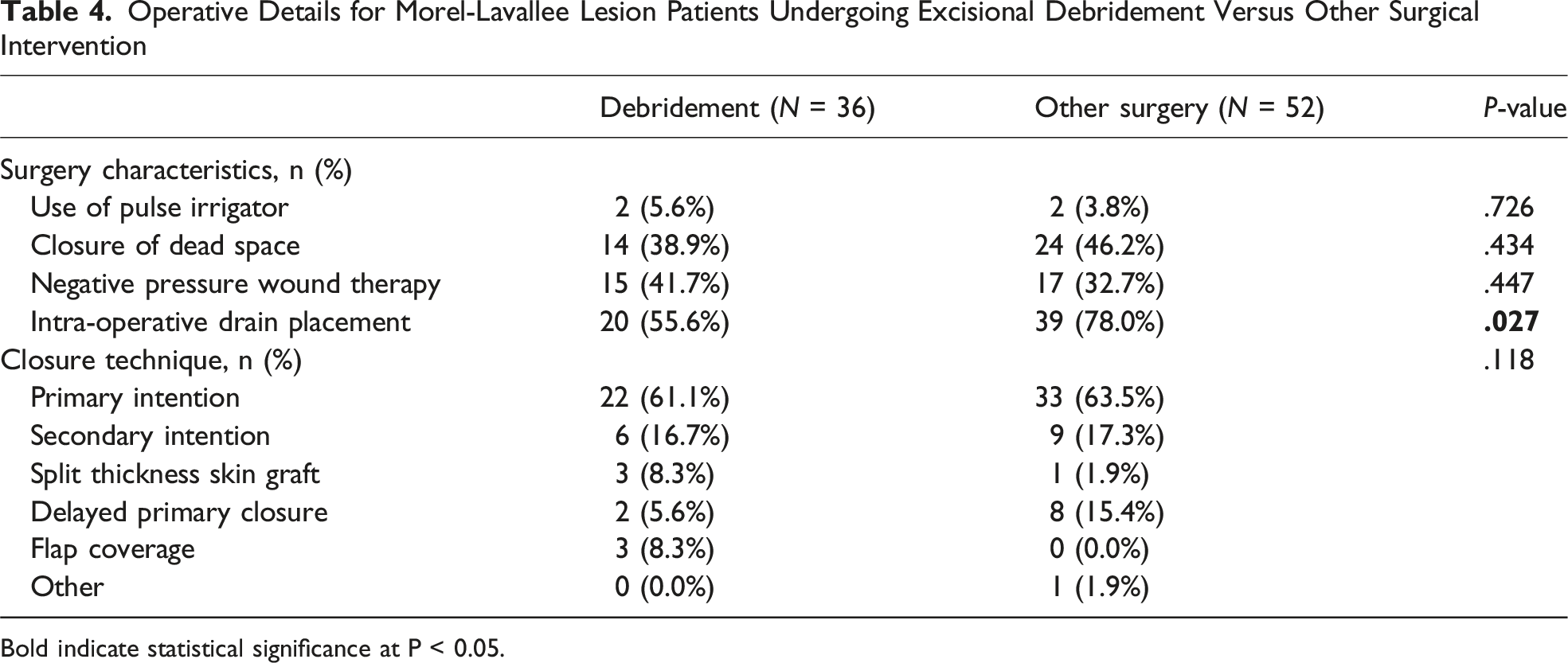
Bold indicate statistical significance at P < 0.05.
Outcomes and Complications for MLL Patients Undergoing Excisional Debridement Versus Other Operative Intervention
Outcomes of Morel-Lavallee Lesion Patients Undergoing Excisional Debridement Versus Other Surgical Intervention
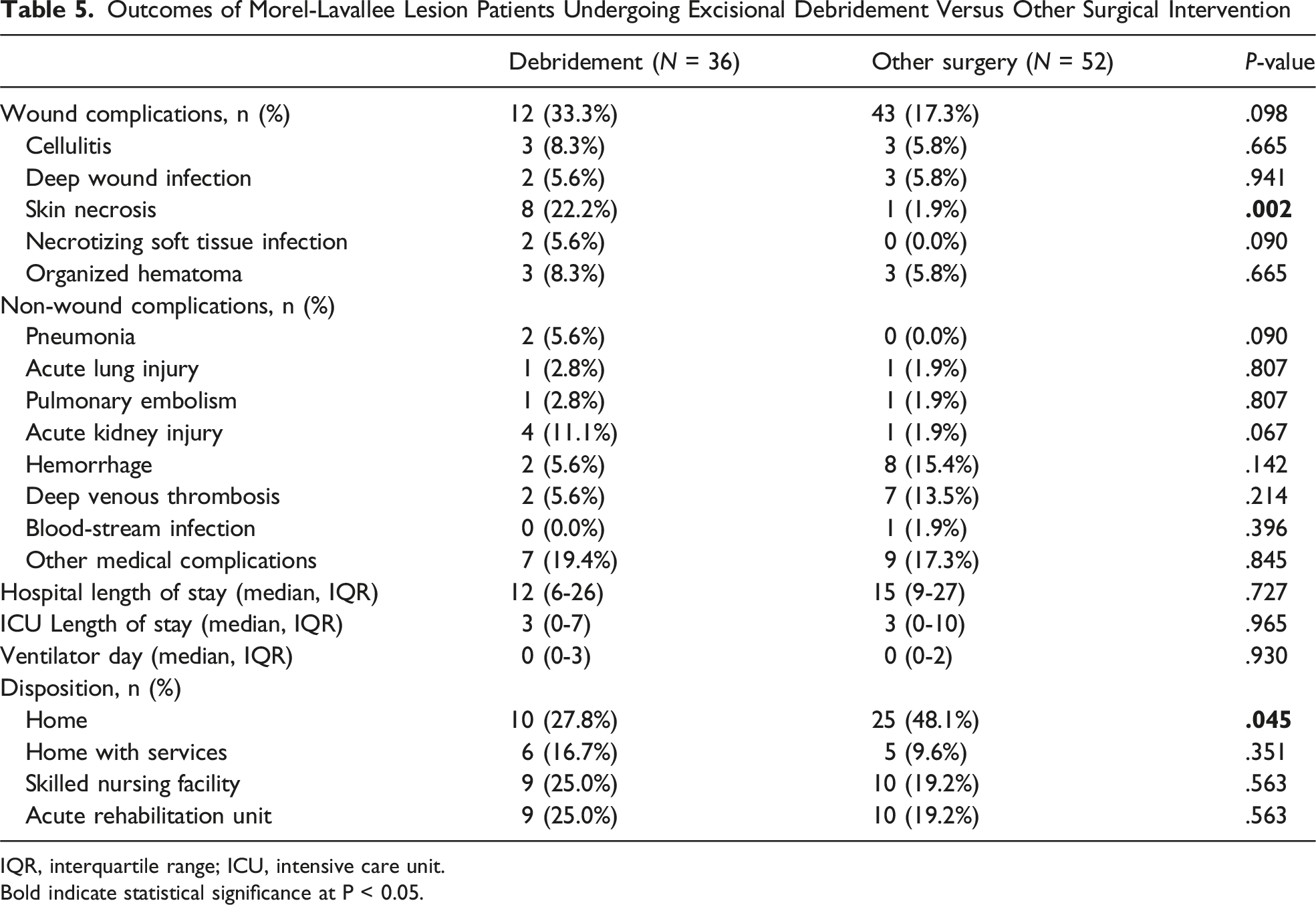
IQR, interquartile range; ICU, intensive care unit.
Bold indicate statistical significance at P < 0.05.
Univariable Logistic Regression of Morel-Lavallee Lesion Patients Undergoing Excisional Debridement
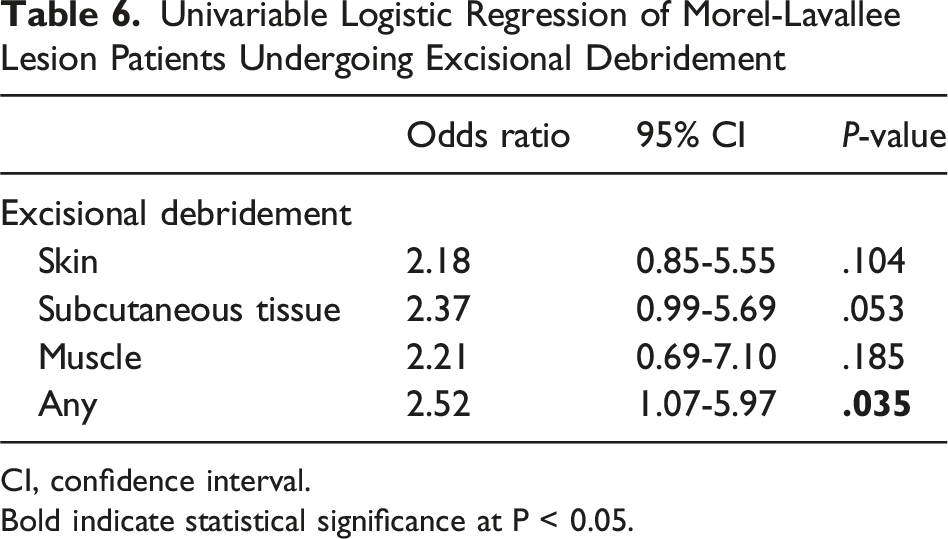
CI, confidence interval.
Bold indicate statistical significance at P < 0.05.
Discussion
Operative intervention remains the primary treatment for MLLs, with excisional debridement being a frequently employed approach. However, high-quality outcomes data are limited, and most prior studies lack generalizability due to selection and publication bias.1–5 In this prospective multicenter cohort, 40% of patients undergoing operative management for MLL underwent excisional debridement, and 20% of these patients developed postoperative skin necrosis. Furthermore, excisional debridement carries more than double the risk of wound complications compared to other operative interventions. These findings outline the postoperative risks associated with excisional debridement and provide opportunities to refine operative decision making in this patient population.
Operative management of MLLs requires meticulous attention to preserving the remaining subcutaneous vascular plexus. The shearing forces that separate subcutaneous tissue from underlying fascia can disrupt perfusing vessels to overlying skin, predisposing patients to necrosis. 2 When necrosis is clinically apparent, excisional debridement is necessary to remove nonviable tissue. However, many patients present with subtle or evolving clinical findings in which skin perfusion is not yet clearly compromised. Progressive cavity expansion can increase pressure on the subdermal capillary network, resulting in delayed skin necrosis. 11 Additionally, the higher proportion of circumferential MLLs in the excisional debridement cohort likely reflects greater initial tissue compromise even before operative intervention, which may partially account for the larger burden of skin loss seen postoperatively. Furthermore, excisional debridement itself may further disrupt residual vascular networks and contribute to postoperative wound complications. 12 Our largest study to date supports this hypothesis as excisional debridement was associated with more than a ten-fold increase in skin necrosis and increased risk of wound complications compared to with other operative strategies. While the authors acknowledge that excisional debridement must be performed for necrosis, the findings of this large multicenter study highlight the potential impact of choosing excisional debridement in cases with uncertain tissue viability and reinforce the value of conservative approaches when clinically feasible.
Intuitively, excisional debridement should create potential for dead space, especially at deeper levels of subcutaneous and muscle tissue. Interestingly, excisional debridement in this study was associated with lower rates of subcutaneous drain placement compared with other operative strategies. This may reflect the alternative approach of simple incision and drainage or minimally invasive techniques with drain placement when excisional debridement was not used. Excisional debridement completely removes the lesion cavity and oftentimes followed by multilayered suture closure. 13 In contrast, incision and drainage or minimally invasive approaches leave portions of the lesion intact and rely on drains postoperatively for continual egress of hemolymphatic fluid and facilitate soft tissue apposition.14,15 Although drains can be beneficial in these settings, they have notable limitations that include clogging, malfunction, incomplete evacuation of irregular cavities, and the potential to serve as a conduit for bacterial entry. 15 Given the variability in drain use observed across centers in this study, standardized protocols may help reduce wound morbidity and should be explored in future investigations.
Advances in minimally invasive and robotic surgery through developments in endoscopic visualization and laparoscopic/robotic instruments have transformed many fields within surgery by reducing wound morbidity, postoperative pain, recovery time, and hospital length of stay. 16 However, application of these strategies to MLLs have been limited, with only a handful of case reports and small case series describing such techniques.17–21 Our current study found that hospital LOS was similar between patients undergoing excisional debridement and less invasive approaches, yet the latter group had higher rates of discharge home. This may reflect improved functional outcomes or could be related to selection bias of the severity of MLL or other concomitant injuries not captured in ISS and AIS which were similar between cohorts. While excisional debridement remains a common and necessary operative approach for MLLs, future research should focus on minimally invasive strategies including endoscopic or robotic surgery that may help decrease the high rate of complications seen in this cohort.
This study has several limitations due to its observational methodology. First, this study is prone to selection bias and residual confounding variables, although the two cohorts were reasonably similar in terms of demographics, comorbidities and injury profiles. Second, this study lacked specific data on MLL volume/size and morphology, extent of debridement in cm3, and indications for operations (eg, laparotomy for concomitant hollow viscus injury),6,7,22 which may have influenced MLL management choice and outcomes. Third, although this was a prospective multicenter study conducted over 3 years, the cohort of 88 patients undergoing operative intervention limited statistical power, particularly for depth of debridement and prevented us from performing a more robust multivariable analysis. Finally, the finding of increased wound complications appears to be predominantly driven by postoperative skin necrosis, which may simply reflect a continued natural history of MLL injuries that require excisional debridement and not a secondary complication per se to the operative intervention itself. Notably, prior studies demonstrate that MLLs managed non-operatively also result in skin necrosis, suggesting that this finding may reflect the underlying pathophysiology of the injury itself.1,3,11 Regardless, this information helps providers be aware of this risk and may alter surgical plans including potentially a more aggressive debridement if indicated at the index operation. Despite these limitations, this study represents the largest prospective MLL cohort undergoing excisional debridement to date and provides important insight on postoperative outcomes, with direct relevance for both patient counseling and clinical decision making.
Conclusion
This prospective multicenter study over 3 years demonstrated that more than one-fifth of MLLs undergoing excisional debridement developed postoperative skin necrosis. In addition, excisional debridement had a more than two-fold increased risk of wound complications compared to other operative interventions. These findings highlight the need to examine alternative operative techniques, such as minimally invasive debridement methods. Taken together, these results emphasize the importance of selecting approaches that preserve soft tissue perfusion whenever feasible, with the goal of reducing wound morbidity and improving postoperative recovery for patients with MLLs.
Footnotes
Author Contributions
Conception and Study design: All authors. Literature Review: PDN, AG, JN. Data acquisition: TC, JD, DS, MS, WB, RC, AT, RP, RC, ET, TD, DK, AS, AJ, AC, MS. Data Analysis and Interpretation: All authors. Drafting of the manuscript: PDN, JN. Critical revision: All authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on request.
Manuscript Presentation
Southern California American College of Surgeons 2026 Annual Meeting.