
Abstract
Inter-surgeon variability in robotic surgery learning curves, as well as the impact of trainee involvement and the presence or absence of a formal robotic training curriculum, remain poorly defined. Cumulative sum (CUSUM) analysis is a validated method for evaluating learning curves in robotic surgery. Our study aimed to utilize CUSUM analysis to explore whether surgical trainees affect surgical operating times. We retrospectively analyzed robotic-assisted cholecystectomies performed by 7 surgeons at a single academic institution between 2012 and 2022. A robotic surgery curriculum was implemented in 2016. Cases were ordered chronologically for each surgeon, and CUSUM learning curves were generated using operative time as the outcome. The first peak in the CUSUM curve indicated the completion of the learning phase. Trainee involvement was analyzed by postgraduate year. 707 operations were performed. Five surgeons demonstrated a distinct learning phase, with a learning phase ranging from 20 to 59 cases, whereas two surgeons exhibited baseline proficiency without an identifiable learning phase. Despite consistently high trainee participation (94.5% of cases) and similar distributions of trainee seniority, learning curve variability persisted. Implementation of an institutional robotic training curriculum was not associated with abrupt changes in learning curve trajectories among surgeons. Learning curves in robotic-assisted cholecystectomies are highly variable and surgeon-specific. Implementation of the robotic training program did not influence the overall trajectory of the surgeon’s personal learning phase.
Key Takeaways
• Surgeon learning curves for robotic-assisted cholecystectomy are highly variable and surgeon-specific, even within a standardized academic training environment. • High levels of trainee involvement do not uniformly prolong operative learning curves, indicating that surgical education can be integrated without compromising attending surgeons’ efficiency. • Implementation of a formal robotic training curriculum did not meaningfully alter surgeon-specific learning curve trajectories, supporting the use of CUSUM analysis for performance monitoring rather than credentialing purposes.
Introduction
Robot-assisted laparoscopic surgery has rapidly expanded across multiple domains of general surgery over the past decade, driven by improved ergonomics, enhanced visualization, and increased dexterity compared with conventional laparoscopy.1,2 As adoption of robotic platforms has accelerated, parallel efforts in surgical education have sought to define objective methods for assessing technical competency, surgeon progression, and procedural mastery within this evolving operative environment. Traditional metrics such as case volume alone have proven insufficient to capture the complexity of skill acquisition, particularly for advanced minimally invasive techniques that involve distinct psychomotor and cognitive demands. 3
In this context, cumulative sum (CUSUM) analysis has emerged as a robust statistical method to evaluate performance trends over time. 4 It is used to quantify learning curves and assess procedural proficiency using objective metrics such as operative time, complication rates, or conversion to open surgery.5-7 Prior literature commonly describes a three-phase learning curve: an initial learning phase, a plateau phase reflecting performance stabilization, and a subsequent improvement phase indicating procedural mastery and efficiency. 8
Operating time remains one of the most frequently used outcome measures for learning curve analysis due to its availability, reproducibility, and sensitivity to technical efficiency.9,10 However, operative duration is influenced by numerous factors including patient complexity, institutional workflows, and trainee involvement.11-13 In academic centers, surgical trainees’ participation is an essential component of education but may introduce variability in operative performance metrics. While several studies have examined learning curves for robotic procedures, limited data exist regarding how trainee participation influences attending surgeon learning curves during the adoption and maturation of robotic techniques.
The primary aim of this study was to investigate the effect of surgical trainee involvement on attending surgeon learning curves for elective robotic-assisted cholecystectomy using CUSUM analysis of operative time. We hypothesized that trainee participation does not adversely affect attending surgeon operative time learning curves, even following the implementation of a structured robotic training curriculum. By evaluating longitudinal performance across multiple surgeons over a decade, this study seeks to clarify the interaction between surgical education and operative efficiency in the robotic era.
Methods
Study Design and Setting
We conducted a retrospective cohort study of all elective robotic-assisted laparoscopic cholecystectomies performed at a single academic institution between July 2012 and June 2022. Procedures were performed by seven attending general surgeons during the study period. All seven surgeons began collecting data starting at the beginning of their careers at the same institution, shortly after completion of fellowship. Six of the surgeons completed a minimally invasive surgery fellowship and one completed a critical care fellowship. Start of employment varied from 2012-2017. Surgeons 1 and surgeons 3-6 underwent formal robot training during fellowship, while surgeons 2 and 7 did not.
The institution implemented a formal robotic training curriculum for surgical trainees in 2016, which served as a temporal reference point for trainee exposure to robotic surgery. This study was approved by the Loma Linda University institutional review board (5180124), with waiver of informed consent.
Patient Selection
Adult patients who underwent elective outpatient robotic-assisted cholecystectomy were included. Cases involving intraoperative cholangiography or indocyanine green fluorescence imaging (Firefly technique) were also included. Exclusion criteria included cholecystectomies performed in conjunction with major additional procedures; emergency or urgent cases; single-site or five-port cholecystectomies; and cases involving pregnancy or incarcerated patients. Minor concomitant procedures were also excluded. Surgical trainees (postgraduate year 1-6) participated in operations at the discretion of the attending surgeon.
Operative Technique and Outcomes
Robotic-assisted cholecystectomies were performed using a standardized four-port technique. Procedures were performed using the da Vinci Si surgical system (Intuitive Surgical Inc., Sunnyvale, CA) until the institutional transition to the da Vinci Xi system in 2017. Surgeon console time was not uniformly available and was therefore excluded from the analysis.
Patient demographic variables collected included age, sex, race and body mass index (BMI). The primary outcome of interest was operative time, defined as the duration from skin incision to skin closure, recorded in minutes. Trainee involvement was documented based on operative reports. If 2 trainees were involved in a case, the most senior trainee was considered the involved trainee, and their PGY year was recorded. Readmissions on file within 30 days after surgery were recorded. Reoperations and interventional procedures including ERCP or percutaneous drainage procedures within 30 days of operation were also recorded.
Statistical Analysis
Continuous variables were summarized using means with standard deviations or medians with interquartile ranges, as appropriate. CUSUM analysis was performed to evaluate surgeon-specific learning curves using operative time as the primary performance metric. For each surgeon, cases were ordered chronologically, and CUSUM scores were calculated as the cumulative deviation of individual operative times from the benchmark mean. The learning phase was defined as the initial upward trajectory of the CUSUM curve, with completion of the learning phase identified at the first peak. Differences in operative time across surgeons were evaluated using the Kruskal-Wallis test. Statistical significance was defined as a two-sided P-value <0.05. All statistical analyses were performed using Stata 14.0 (StataCorp, College Station, TX) and Microsoft Excel v. 2024 (Microsoft Corporation, Redmond, WA).
Results
Patient and Case Characteristics
Demographics of the Study Population (n = 707)
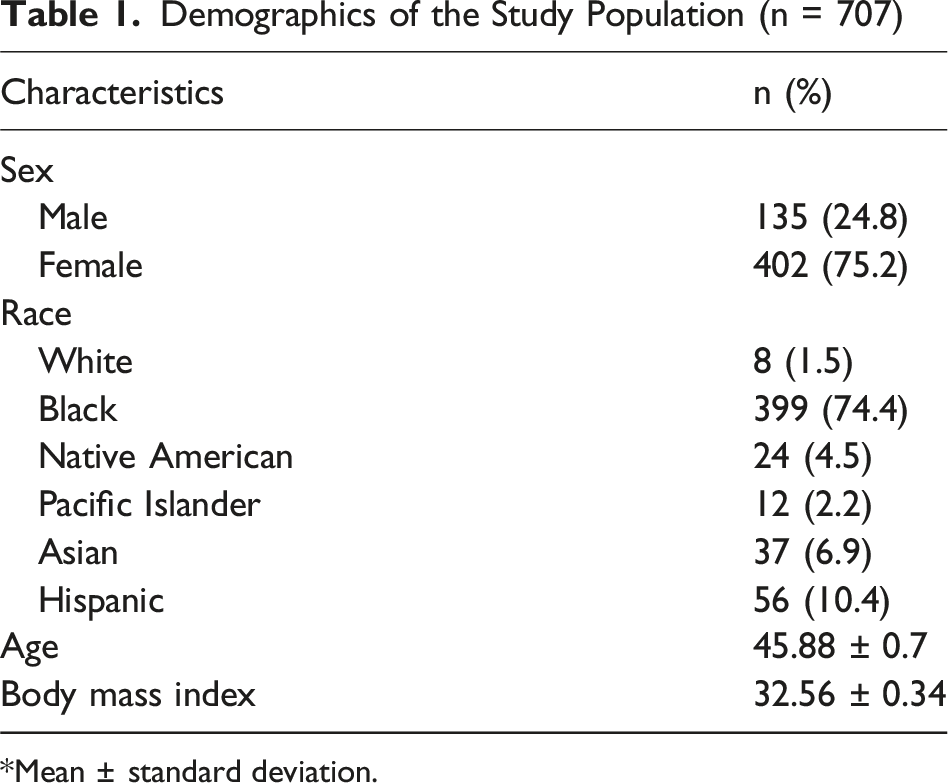
*Mean ± standard deviation.
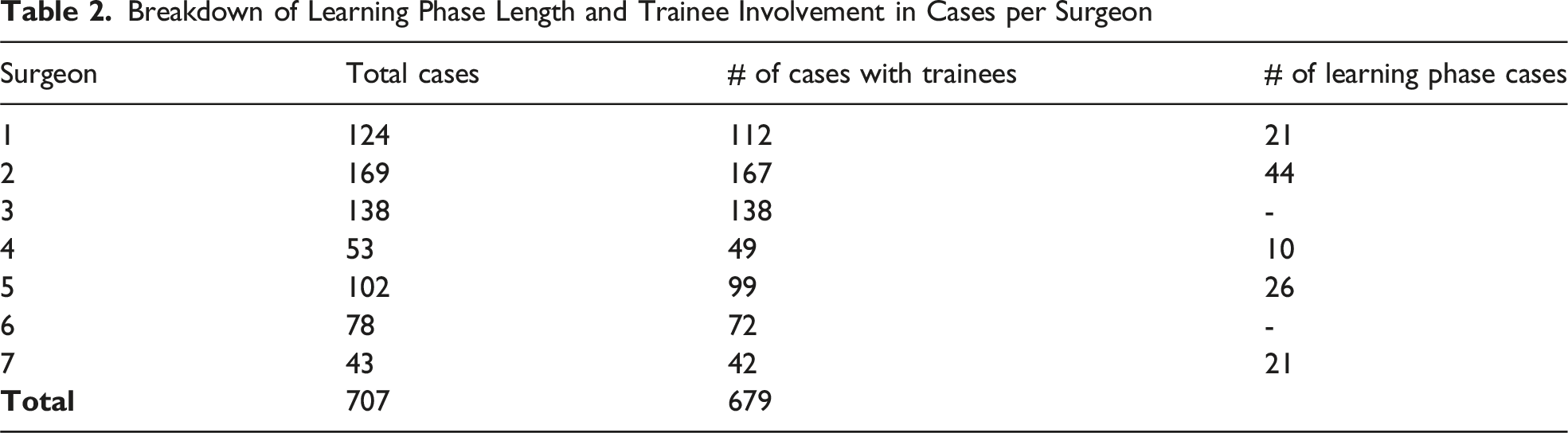
Breakdown of Learning Phase Length and Trainee Involvement in Cases per Surgeon
Learning Curve Analysis
Figure 1 illustrates surgeon-specific CUSUM learning curves. Vertical reference lines denote the time of implementation of the institutional robotic training curriculum in 2016 for Surgeons 1-3 and Surgeon 5. Surgeon-specific cumulative sum (CUSUM) learning curves for robotic procedures. Vertical reference lines denote the time of institutional implementation of the robotic training curriculum for applicable surgeons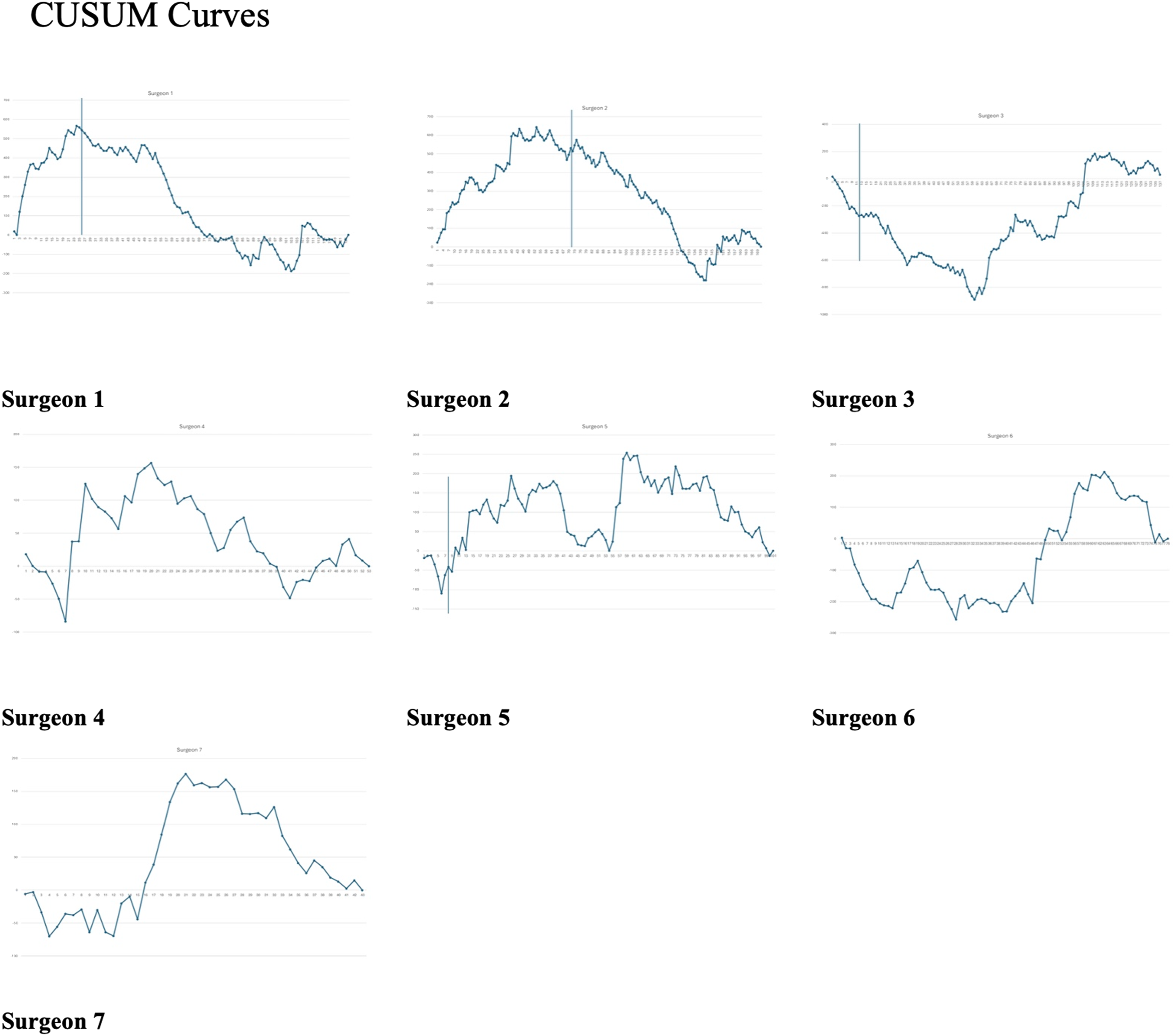
Surgeons 1, 2, 4, 5, and 7 demonstrated a distinct initial learning phase with a upward slope, while Surgeons 3 and 6 did not exhibit a clear learning phase at the onset of independent practice. Learning phase caseloads for Surgeons 1, 2, 4, 5, and 7 were 20, 53, 24, 59, and 21, respectively. These surgeons subsequently demonstrated a second learning phase following implementation of the robotic training curriculum. In contrast the CUSUM curves for initially remained stable or negative before increasing after approximately case 60 for Surgeon 3 and case 28 for Surgeon 6, peaking after 56 and 35 cases, respectively.
Operative Time Distributions
Operative time distributions varied significantly across surgeons. Surgeon-specific median procedure times ranged from 71.5 to 113 minutes. Maximum procedure times among surgeons ranged from 205 to 335 minutes. There were significant differences in operative time distributions across surgeons (P < 0.001).
Trainee Involvement by Postgraduate Year
Figure 2 depicts the distribution of resident involvement by postgraduate year (PGY) across all surgeons. The x-axis represents PGY involvement and level, with 0 indicating cases without trainee involvement and 6 indicating fellow-only involvement, while the y-axis represents the number of cases involving each PGY level. Distribution of resident involvement by postgraduate year (PGY) across surgeons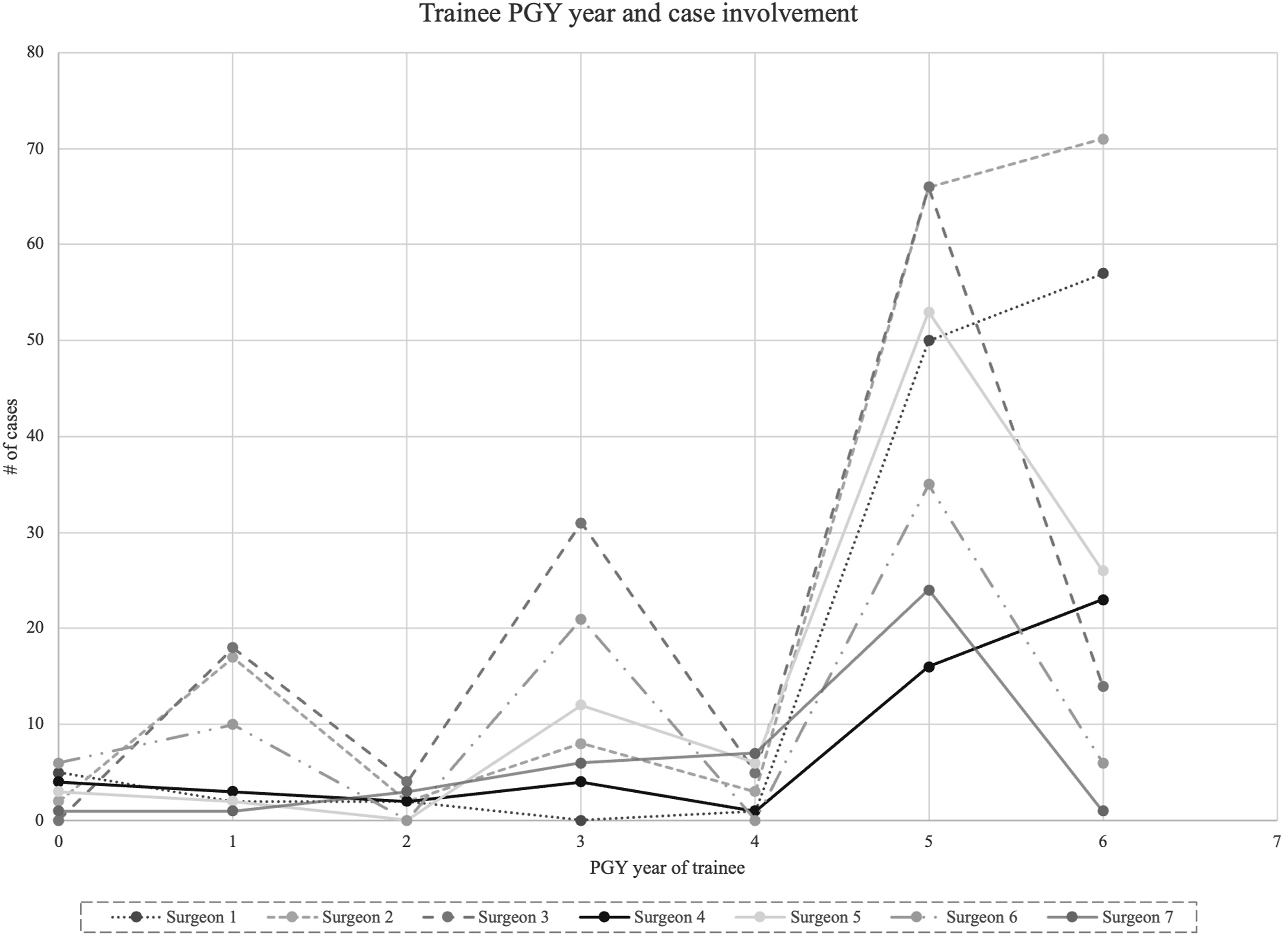
30-Day Readmission Rates and 30-Day Postoperative Procedure or Reoperation Rates

Discussion
Our findings demonstrate marked heterogeneity in surgeons’ learning trajectories, with substantial variability in the presence, duration, and shape of learning phases. While several surgeons exhibited a classic learning curve, with an initial phase of inefficiency followed by stabilization and improvement, others showed baseline proficiency without a discernible learning phase. These findings underscore that learning curves are not uniform across surgeons and suggest that procedural experience, prior training, and contextual factors play an important role in shaping performance over time.
A systematic review by Soomro et al aligns with our findings. They reported that learning curve definitions vary widely across procedures, with proficiency requirements spanning broad ranges and often dependent on specific procedural context and prior experience. 14 In robotic cholecystectomy, Karim et al reported that the number of cases required to demonstrate a learning plateau range from 16 to 134, depending on how learning is defined and measured. 15
An important factor contributing to learning curve variability appears to be baseline surgeon experience. Surgeons 1in our cohort had undergone formal robotic training during fellowship prior to independent practice, which may partially explain the shorter or absent early learning phases observed in these individuals. Prior experience with minimally invasive or robotic platforms has been associated with attenuated learning curves in other procedural domains, suggesting that initial exposure and skill transfer can influence early operative performance. 16 Additionally, surgeons 4-6 entered independent practice later in the study period and thus had fewer cases overall, which may limit visibility into later phases of learning.
Distinct learning patterns, including non-linear or biphasic curves, may reflect not only technical skill acquisition but also evolving case complexity, trainee involvement, and adaptation to institutional workflows. Secondary inflection points observed after the nominal learning phase may correspond to transitions in case mix or increasing trainee autonomy, a pattern noted in other robotic learning studies across surgical specialties. Somashekhar et al report that the learning curve in robotic surgery depends not only on the surgeon but also on case mix and the team’s cumulative experience. 17
Despite consistently high trainee participation across all surgeons and a similar distribution of senior trainee involvement, learning curve variability persisted. This suggests that differences in operative efficiency are not solely attributable to trainee involvement, corroborating prior reports that trainee participation does not uniformly prolong learning curves and can be integrated into performance without compromising efficiency. Schroeck et al demonstrated that trainees do not negatively impact the institutional learning curve, using operative time and other objective metrics. 18
The implementation of an institutional robotic training curriculum did not result in abrupt or consistent changes in learning curve trajectories among surgeons with pre- and post-implementation data, suggesting that formal curricula may exert more gradual or context-specific influence on performance rather than immediate, measurable shifts in operative times 19 This interpretation aligns with broader work indicating that structured training programs can enhance skill acquisition without necessarily altering aggregate procedural metrics in the short term. 20
The focus of this study was on operative time as a metric of surgeon learning, rather than patient outcomes. Given that the surgeries selected were non-inflamed gallbladders operated upon electively, the risk of postoperative complications is predictably lower. Reoperation rate was 0%, and overall rates of 30-day readmission and percutaneous drainage were low compared to 30-day readmission rates of 7.7-8.5% and percutaneous drainage rates of 1.31-2.91% in published data using established databases. 21 30-day ERCP rate was 0.99%, as compared to 0.34% rate for laparoscopic cholecystectomy using national databases. 22 While there is minimal literature regarding robotic cholecystectomy 30-day ERCP rates, national data does indicate that robotic-assisted cholecystectomy is also associated with a higher rate of postoperative biliary interventions than the laparoscopic approach. 23 It should be noted that tracking of complication rates and other quality metrics was limited due to electronic health record access limitations, including the inability to access non-institutional records.
This study has several other limitations. Its retrospective design limits causal inference, and unmeasured confounders such as case complexity and patient comorbidities may have influenced operative times and learning curve trajectories. Although trainee involvement was quantified by postgraduate year, the degree of trainee autonomy within individual cases could not be assessed and may have varied over time. Without a third-party vendor, individualized trainee performance data could not be tracked. This is due to institutional legal requirements limiting industry facilitation of direct education. Furthermore, information regarding experience of the operative staff could not be obtained. However, the institution did have extensive prior experience with robotic technology, with quarterly in-service training for operative staff present since 2004 to promote workflow standardization. Finally, this study reflects the experience of a single institution and a limited number of surgeons, which may limit generalizability to other practice settings.
Surgeon-specific CUSUM learning curves demonstrated substantial variability, highlighting the individualized nature of learning in robotic surgery. Despite similar patterns of trainee involvement across surgeons, learning curve differences persisted, suggesting that variability in operative efficiency is mainly independent of trainee involvement. Implementation of an institutional robotic training curriculum did not appear to meaningfully alter learning curve trajectories during the learning phase, as indicated by pre- and post-implementation data. These findings suggest that CUSUM learning curves are heterogeneous and context dependent, limiting their utility as a sole criterion for credentialing. Rather, CUSUM analysis may be better applied as a tool for longitudinal performance assessment, quality improvement, and surgeon self-monitoring.
Footnotes
Author Note
All authors read and approved the final manuscript.
Ethical Considerations
This project was approved by the Loma Linda University Institutional Review Board (5180124).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Z.T. received a travel award from Prytime Medical Devices Inc. (Boerne, TX) unrelated to the present study. All authors declare no conflicts of interest.
Data Availability Statement
Data is available from the corresponding author upon reasonable request.