
Abstract
Background
Laparoscopic Subtotal Cholecystectomy (SC) is a technique for performing safe cholecystectomy when excessive inflammation prevents exposure of the Critical View of Safety. Studies have evaluated outcomes and complications of laparoscopic cholecystectomy (LC), with mixed results in terms of surgeon experience. It is unclear if the rate of SC is associated with experience. We hypothesized that the rate of SC would decrease as surgical experience increased.
Methods
We performed a retrospective review of LC performed at an academic medical center. Demographics were analyzed using descriptive statistics. We performed a multivariable logistic regression to examine the relationship between years in practice and performance of SC. We performed a sensitivity analysis comparing those in their first year on faculty with all others.
Results
Between November 1, 2017, and November 1, 2021, there were 1222 LC performed. 771 patients (63%) were female. 89 patients (7.3%) underwent SC. There were no bile duct injuries requiring reconstruction. Controlling for age, sex, and ASA class, there was no difference in the rate of SC by years of experience (OR .98, 95% CI .94–1.01). In a sensitivity analysis comparing first-year faculty to those beyond their first year, there was also no difference (OR .76, 95% CI 0.42-1.39).
Discussion
We find no difference in the rate of performance of SC between junior and senior faculty. This reflects consistency, in keeping with best practice guidelines. This could be confounded by junior faculty requesting assistance during difficult operations. Further investigation into factors affecting decision-making may clarify this.
Key Takeaways
Laparoscopic Subtotal Cholecystectomy is an uncommon, but important technique for performing a safe operation in a hostile operative field. There is no difference in the rate of performance of subtotal cholecystectomy among surgeons of varying years of experience.
Background
Laparoscopic subtotal cholecystectomy (SC) is a well-accepted surgical approach in the difficult cholecystectomy when the Critical View of Safety cannot be safely obtained due to excessive inflammation, fibrotic scaring or altered anatomy. 1 Utilization of this technique has increased over time in the United States, in keeping with safe cholecystectomy guidelines, 2 while rates of conversion to open cholecystectomy have decreased between 2003 and 2014. 3 With these trends, some have expressed concern that SC may be performed too commonly, in light of potential consequences of this approach.4,5
In this same time frame, there has been growing concern that trainees in general surgery are not adequately prepared for independent practice upon completion of residency. 6 This has been reflected in surveys of residency faculty, fellowship directors, and surgeons in practice.7,8 Furthermore, when surveyed, a substantial number of chief residents and recent graduates feel unprepared or unconfident for independent practice.9-11 These findings suggest the possibility that early career surgeons are uncomfortable with, or ill-prepared for, more difficult cholecystectomies and therefore may opt to perform subtotal cholecystectomy excessively.
While studies have investigated the utilization of subtotal cholecystectomy, there is no description of subtotal cholecystectomy performance stratified by years in surgical practice. The purpose of this study is to investigate the rates of laparoscopic subtotal cholecystectomy performed by surgeons with different levels of experience. Our hypothesis was that early career surgeons would perform a higher percentage of subtotal cholecystectomies compared with their more senior counterparts.
Methods
The study was given exempt status by the institutional review board (IRB).
This was a single-center retrospective review of all laparoscopic cholecystectomies performed by the Acute Care Surgery service, on patients 18 years of age or older, between November 1, 2017, and November 30, 2021. The study population was identified by CPT code 47562, 47563, and 47564 utilizing a centralized electronic medical record (EMR) tool. Our study group was identified via keyword search using a centralized medical record research tool among all laparoscopic cholecystectomies for the following terms: “subtotal cholecystectomy,” “subtotal cholecystectomy,” “fenestrating cholecystectomy,” “fenestrated cholecystectomy,” “partial cholecystectomy,” and then confirmed via manual chart review. Attending surgeon names were identified using an EMR report tool. Laparoscopic Cholecystectomies performed by services other than Acute Care Surgery were excluded. All baseline characteristics were obtained using our centralized EMR tool and included age at the time of surgery, sex, race, ethnicity, BMI, American Society of Anesthesiology (ASA) class, and length of stay.
Years in practice was calculated from attending surgeon name and procedure data. Our independent variable was years in practice, and dependent variable was subtotal cholecystectomy (SC) vs traditional cholecystectomy (TC). A sensitivity analysis was performed replacing years in practice with instructor vs faculty status. Instructors are defined as those in their first year of independent practice following completion of fellowship.
Statistical Methods
Baseline characteristics were assessed using both chi-squared and Student’s t-test analyses. Multivariable logistic regression was performed with years in practice as the independent variable and subtotal cholecystectomy as the dependent variable. Covariates included in the multivariable model were age, ASA class, BMI, and sex. Years in practice and instructor status on SC were assessed with multiple logistic regression using the above covariates. The same model was used replacing years in practice with instructor status (yes/no) for the sensitivity analysis. All statistical analyses were performed using Stata version 16.1 (Stata Corp, College Station, TX).
Results
Baseline Patient Characteristics.
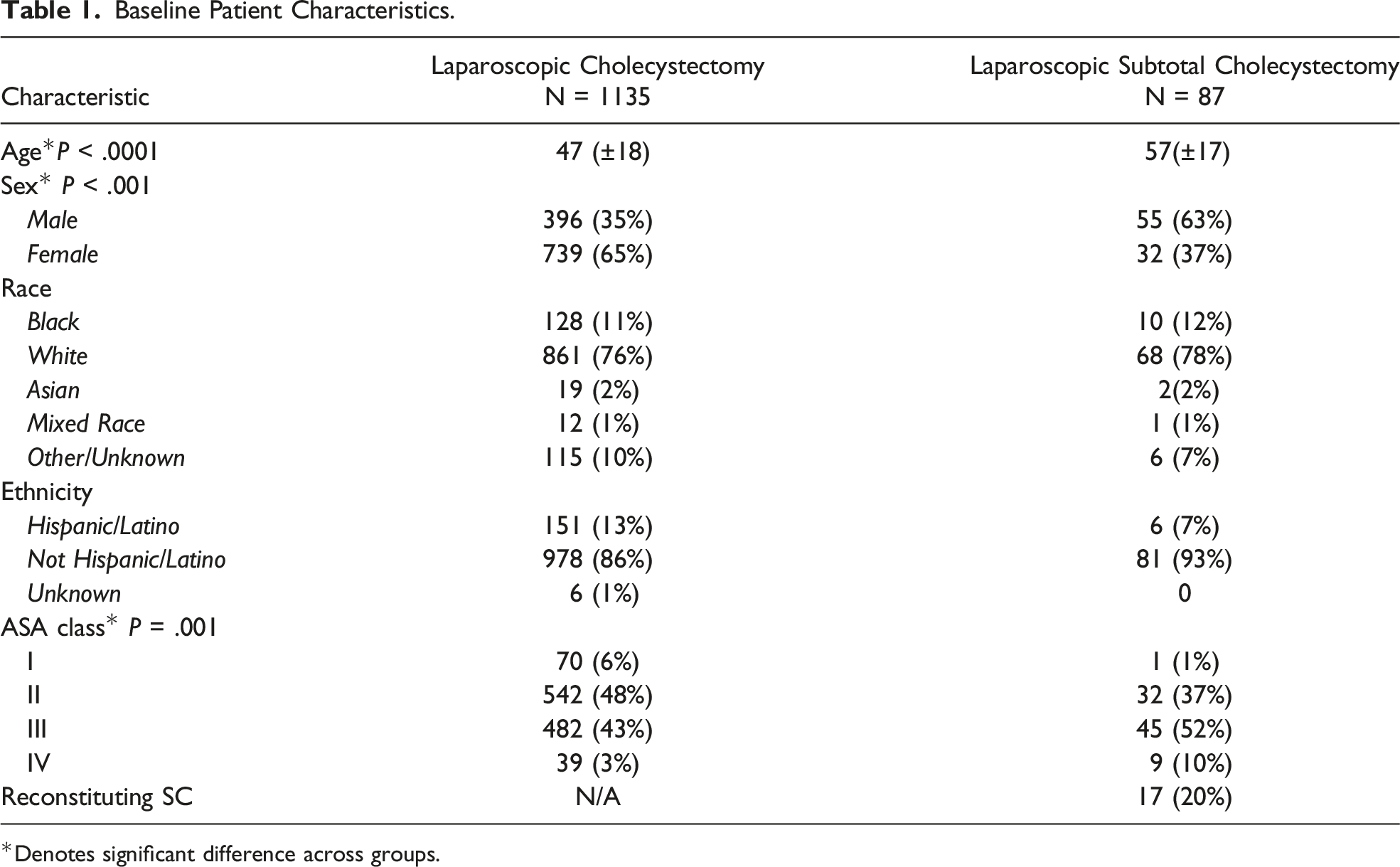
*Denotes significant difference across groups.
Univariate Outcomes Between Standard and Subtotal Cholecystectomy.

*Denotes significant difference across groups.
In a sensitivity analysis comparing instructors (those in their first year of practice) to other faculty, there was no difference (OR .79, 95% CI 0.43-1.44, P = .434). There were no cases of bile duct injury requiring reoperation or reconstruction in the cohort.
Discussion
In this retrospective study of 1222 laparoscopic cholecystectomies, we note no difference in the rate of performance of subtotal cholecystectomy between junior and senior faculty. Laparoscopic subtotal cholecystectomy remains a safe and effective, but relatively uncommon operation when the critical view of safety cannot be safely obtained. This allows for relief of biliary symptoms without risking bile duct injury requiring reconstruction. 1
These findings are in contrast with growing concerns in the surgical literature regarding the readiness for practice of recent residency graduates. With increasing operative complexity and decreased work hours during general surgical residency training, both faculty and graduating residents have expressed concern in survey studies that residents completing general surgery training are not fully prepared for independent practice.6-11 Additionally, multiple retrospective studies suggest an association between early career surgeons and increased complication rates.12,13 In this series, we noted no difference in performance of subtotal cholecystectomy, including on sensitivity analysis of those surgeons in their first year of practice.
Our study has several limitations. First, this is a retrospective study, which relies on operative documentation and the performance of an EMR search tool. It is possible that not all cases of subtotal cholecystectomy are captured. Second, this was performed in a quaternary, academic referral center. It is possible that the severity of patients’ biliary disease, as well as their comorbidities, makes it difficult to generalize these findings to the surgical community at large. Finally, while we did not note a difference in the rate of subtotal cholecystectomy between junior and senior faculty, part of the institutional culture of safety involves partners assisting one another with more difficult operations, which could potentially skew the findings and limit their applicability in dissimilar settings.
In conclusion, in this retrospective review, we did not identify a difference in the rate of performance of subtotal cholecystectomy between junior and more experienced faculty. This reflects consistency across seniority levels, in keeping with multi-society best practice guidelines. These results can be confounded by junior faculty requesting assistance during more difficult operations. Prospective investigation into surgeon and patient factors affecting decision-making may shed light on this.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.