
Abstract
Background
During initial trauma assessment, chest x-ray (CXR), pelvis x-ray (PXR), and Focused Assessments with Sonography for Trauma (FAST) are standard imaging adjuncts in blunt trauma. Hypotensive patients with negative CXR/PXR/FAST results “triple negative” present diagnostic challenges. The aim of this study was to characterize injury patterns, management strategies, and outcomes in this high-risk cohort.
Methods
This is a retrospective cohort study (2015-2024) at an urban Level 1 trauma center. Blunt trauma patients aged ≥16 years presenting with systolic blood pressure<90 mmHg and negative CXR/PXR/FAST results were included. Negative CXR/PXR results were defined by consensus review from two trauma surgeons and a trauma radiologist, who determined whether the imaging results could explain hemodynamic instability. Descriptive analyses evaluated etiologies of hypotension, diagnostic pathways, interventions, and outcomes.
Results
A total of 73 patients met inclusion criteria (median age: 42 years, 69.9% male). Blood products were administered in 65.7%, with massive transfusion protocol activated in 13.7%; 17.8% required vasopressors in the Emergency Department. Following initial evaluation, 93.2% underwent computed tomography, while two proceeded directly to the operating room, and one died following resuscitative thoracotomy. Common injury patterns were hemorrhage from extremity injuries, high spinal cord injuries, abdominal solid organ injuries, and severe traumatic brain injuries. Overall, 21.9% required emergent operative and 11.0% required emergent endovascular intervention. Mortality was 5.5%, with all deaths due to severe neurologic injury.
Conclusion
Despite negative initial adjunct imaging, hypotensive blunt trauma patients frequently harbor injuries requiring emergent operative or endovascular intervention, with hemorrhagic and neurologic injuries among the most common causes.
• Hypotensive blunt trauma patients with negative chest x-ray, pelvic x-ray, and FAST imaging frequently harbor clinically significant hemorrhagic or neurologic injuries requiring urgent operative or endovascular intervention. • Negative initial adjunct imaging does not exclude life-threatening injuries and must prompt continued diagnostic vigilance and escalation of care. • Recognition of this high-risk phenotype and timely escalation of diagnostic and therapeutic interventions are essential to improve patient outcomes.Key Takeaways
Introduction
During the initial trauma assessment following blunt trauma, early identification of patients with hemodynamic instability and its etiology is essential, as delays in identifying hemorrhage or alternative shock states contribute to preventable morbidity and mortality. As part of the initial trauma assessment, chest x-ray (CXR), pelvis x-ray (PXR), and Focused Assessments with Sonography for Trauma (FAST) are commonly performed as diagnostic adjuncts to identify the cause of hemodynamic instability following blunt trauma. These rapid, repeatable imaging modalities remain central to Advanced Trauma Life Support (ATLS) algorithms because they provide immediate diagnostic information without interrupting resuscitation.1-3
Despite their widespread use, these modalities have important diagnostic limitations. CXR demonstrates only moderate sensitivity—approximately 70% to 75% for clinically significant thoracic injuries.4-6 PXR provides limited diagnostic yield with poor sensitivity for mechanically unstable pelvic fractures and may miss up to one-third of unstable pelvic fractures while rarely identifying bleeding outside classic open book or vertically unstable fractures.7-9 FAST is highly operator dependent, with sensitivity ranging from 20% to 90%. It frequently fails to identify retroperitoneal hemorrhage, contained solid organ injuries, or spine/pelvic bleeding, all of which can still produce profound hypotension.3,10-12 While computed tomography (CT) provides the most comprehensive assessment of injuries, an increased risk of adverse events has been reported in hypotensive patients undergoing CT. 13 These limitations create diagnostic challenges when evaluating hemodynamically unstable trauma patients.
A particularly challenging clinical scenario arises when a blunt trauma patient remains hypotensive despite negative CXR, PXR, and FAST—referred to as a “triple negative” presentation. These patients represent a high-risk subgroup in whom standard diagnostic modalities in the trauma bay fail to identify a source of instability. In addition to the risk of false-negative results on CXR/PXR/FAST, occult retroperitoneal bleeding, spinal cord injury leading to neurogenic shock, severe traumatic brain injury, extremity injury, and mixed shock states may all present with persistent hypotension despite reassuring initial adjunct imaging. Yet, because triple negative presentations are rare, injury patterns, diagnostic strategies, and clinical outcomes remain poorly described, contributing to significant practice variability. The objective of this study is to describe the injury patterns, diagnostic/therapeutic pathways, and outcomes of hypotensive blunt trauma patients with triple negative imaging managed at a Level 1 trauma center in the modern era.
Methods
Study Design
After approval by the Institutional Review Board, this retrospective cohort study was conducted at an urban Level 1 trauma center between January 2015 and July 2024. Patients were eligible for the study if they were 16 years of age or older, sustained blunt trauma, and arrived at the Emergency Department (ED) with a systolic blood pressure below 90 mmHg. The study excluded patients who did not undergo initial adjunct imaging (CXR, PXR, and FAST) as part of standard trauma evaluation. Only patients with a negative CXR, negative PXR, and FAST that was negative or equivocal were included. CXR and PXR were considered negative when a consensus review by two trauma surgeons (LB and KP) and an emergency radiologist (AG) determined that no radiographic finding could reasonably account for the patient’s hypotension.
Patients were stratified by hemodynamic response to initial resuscitation and classified as non-responders (persistent SBP <90 mmHg), transient responders (initial improvement in blood pressure followed by recurrent hypotension), or responders (initial hypotension but after resuscitation sustained SBP > mmHg throughout their ED course).
Data Variables
All data was obtained from the institutional trauma registry and electronic medical records. Collected data included patient demographics (age, sex, race/ethnicity, body mass index [BMI]), prehospital information, mechanism of injury, ED vital signs and laboratory values, transfusion requirements, vasopressor use, injury severity score (ISS), and Abbreviated Injury Scale (AIS) by body region, hospital and intensive care unit (ICU) length of stay, hospital complications, and in-hospital mortality. Imaging data included initial adjunct studies and all subsequent studies such as computed tomography (CT), magnetic resonance imaging (MRI), and echocardiograms. Clinical trajectories were recorded including the patient’s immediate destination following initial assessment/resuscitation in the trauma bay (CT, MRI, operating room [OR], interventional radiology [IR], ICU, or other locations) and subsequent hospital course. Operative and endovascular procedures were reviewed for indications and intraoperative findings. The primary aim was to describe injury patterns and clinical outcomes of hypotensive blunt trauma patients with a triple negative presentation. Secondary outcomes included diagnostic pathways, rates and types of emergent operative or endovascular procedures, post-ED disposition, transfusion requirements, vasopressor use, distribution of shock etiologies, and mortality with cause of death.
Statistical Analysis
Analyses focused on descriptive statistics appropriate for an exploratory observational study. Continuous variables are reported as means or medians with interquartile ranges as appropriate. Categorical variables are presented as frequencies and percentages. Subgroup analysis was performed between patients requiring emergent operative and/or endovascular intervention. Data were collected and managed using Microsoft Excel for Mac (version 16.73; Microsoft Corporation, Redmond, WA). The study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE).
Results
Patient Characteristics
Patient Demographics and Injury Characteristics
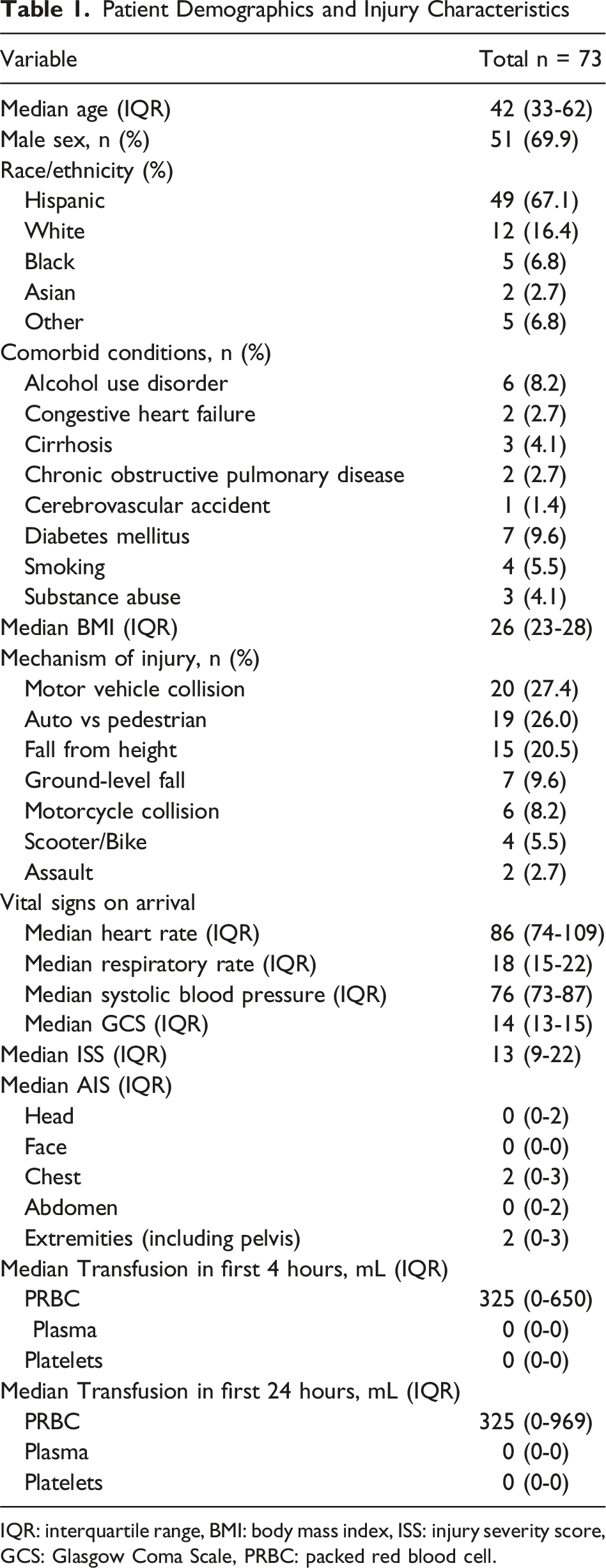
IQR: interquartile range, BMI: body mass index, ISS: injury severity score, GCS: Glasgow Coma Scale, PRBC: packed red blood cell.
Initial Management, Resuscitative Interventions, and Diagnostic Pathways
During the initial resuscitation, two-thirds of patients (65.7%) received blood transfusion, and massive transfusion protocol was activated in 13.7%. Vasopressors were started in 17.8% of patients while in the ED. Following the initial evaluation with negative CXR, PXR, and FAST, 93.2% of patients (68/73) were transported to the CT scanner. Two patients were taken directly to the operating room without CT imaging, one was admitted to the ICU, and one to the medical-surgical floor; two patients died in the ED, including one following resuscitative thoracotomy. Following CT, patient disposition diversified (Figure 1). Among the 68 patients who underwent CT imaging, 29 were subsequently admitted to the ICU, 13 proceeded to the operating room for surgical intervention, 5 went for IR procedures, and 4 underwent MRI for evaluation of suspected spinal cord injury. The remaining patients were admitted to surgical observation, step-down, or medical-surgical units. Summary of initial management pathways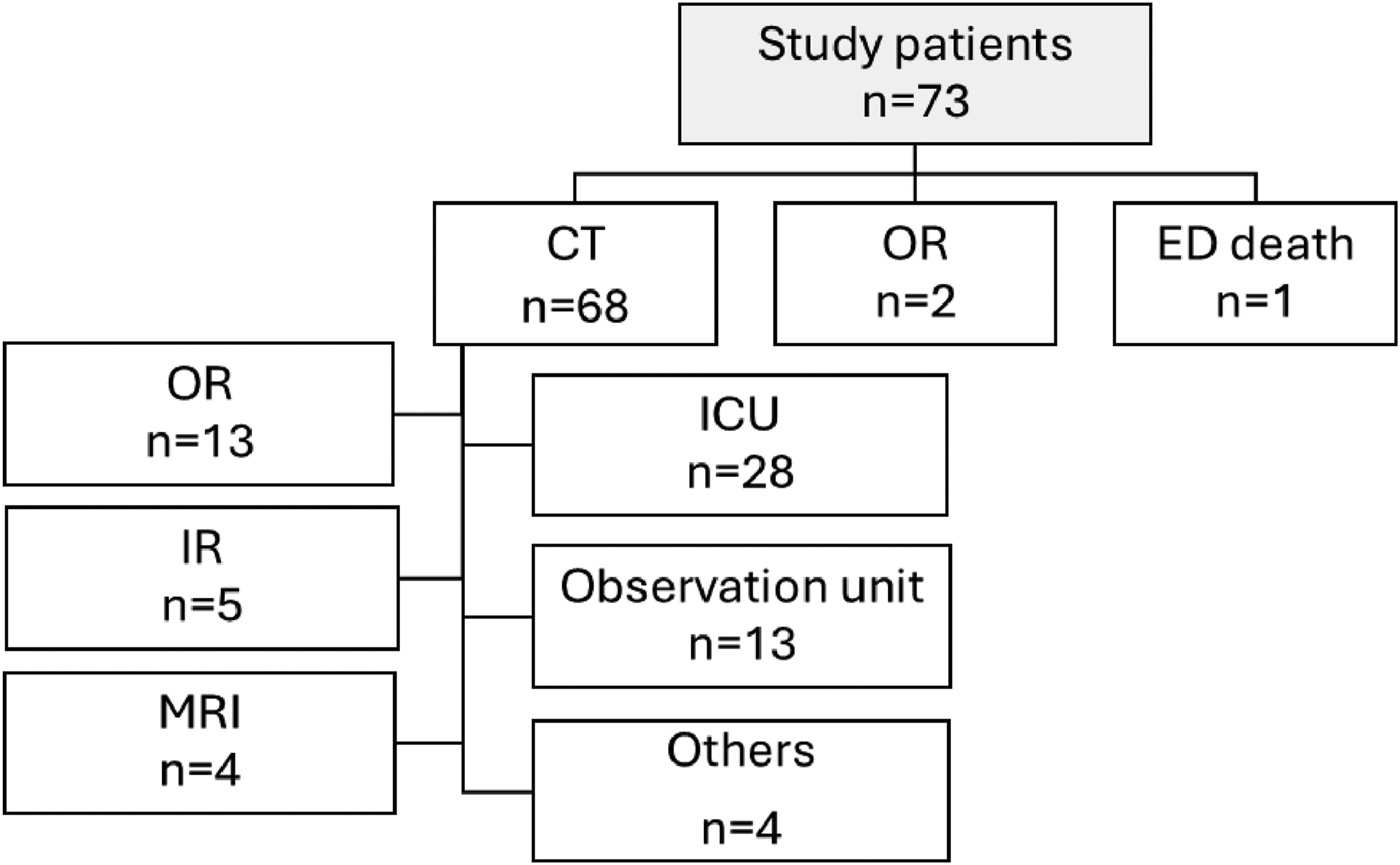
Hemodynamic Response and Subsequent Interventions
Patients were stratified by hemodynamic response to the initial resuscitation. Four patients were classified as non-responders, 27 were classified as transient responders, and 42 patients were classified as responders (Figure 2). Among non-responders (n = 4), two patients required emergent operative intervention for hemorrhage control and vascular injury, one was admitted to the ICU, and one died in the ED. Clinical course of non-responders (a) and transient responders (b) OR: operating room, ICU: intensive care unit, IR: interventional radiology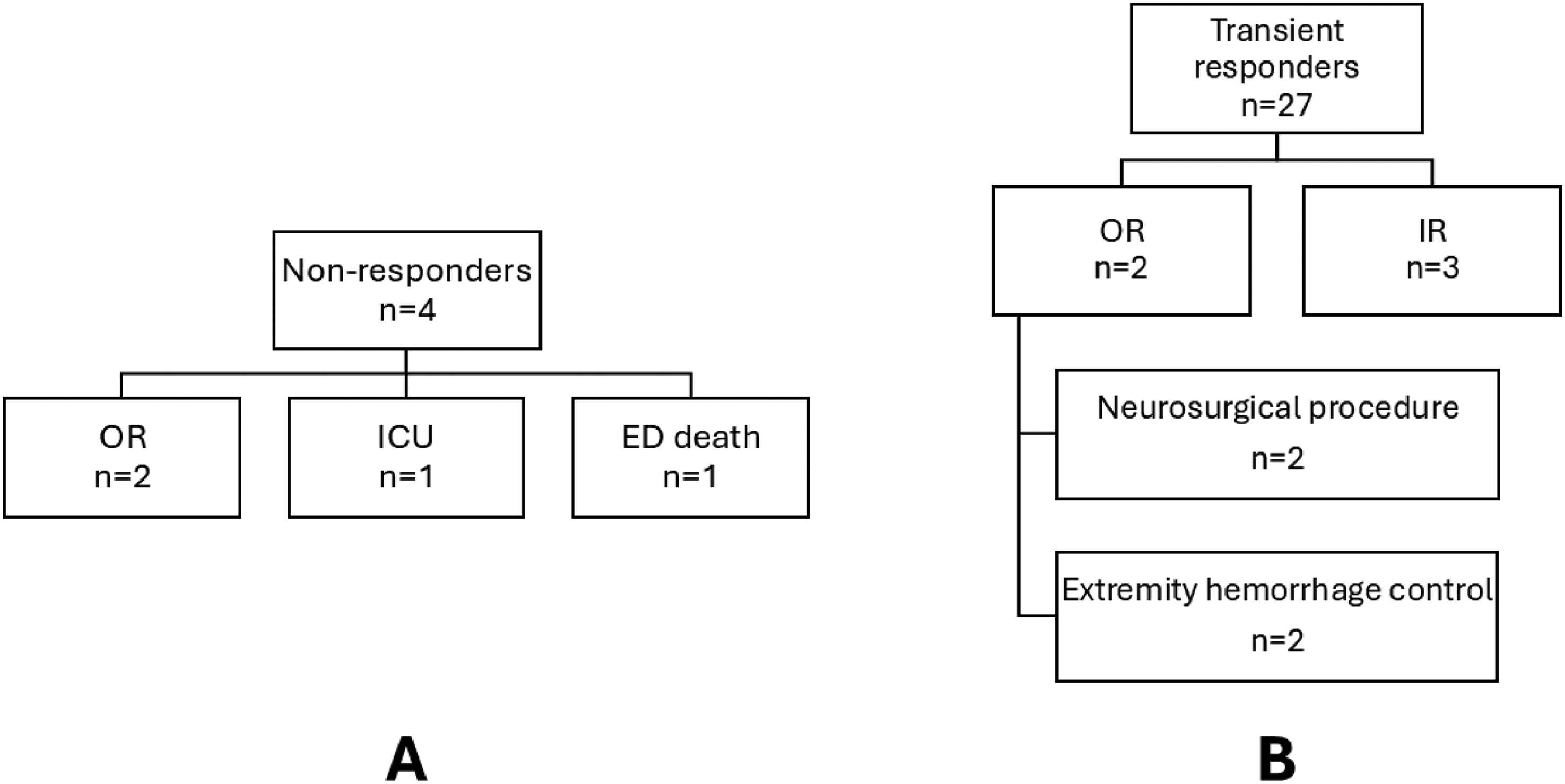
Among transient responders (n = 27), a substantial proportion (33.3%) required urgent intervention. Three patients underwent IR procedures for embolization of solid organ injuries or pelvic fractures, four required operative intervention with neurosurgery, including decompressive craniectomy and spinal stabilization, and two underwent operative management for extremity hemorrhage control.
Of the 73 patients, 65.7% received blood products and 17.8% were started on vasopressors. After initial resuscitation, 68 patients (93.2%) proceeded directly to CT, including 3 non-responders, 26 transient responders, and 39 responders. Among these 68 patients, 11 (16.2%) received vasopressors (2 non-responders, 3 transient responders, and 6 responders), and 46 (67.6%) received blood products (2 non-responders, 21 transient responders, and 23 responders). Accordingly, most non-responders (75%) and transient responders (77.8%) received blood products, and 57.1% of responders also received blood products, consistent with early, balanced trauma resuscitation. Massive transfusion protocol was activated in nine patients who proceeded directly to CT.
Injury Patterns
In our cohort, the most common injury patterns were hemorrhage from extremity, neck or vascular injuries (n = 11, 15%), severe traumatic brain injuries (n = 11, 15%), solid organ injuries in the abdomen (n = 8, 11%), and high spinal cord injuries (n = 5, 7%). Additional injury patterns included major extremity fractures, rib and sternal fractures with or without associated pulmonary contusions, scalp lacerations and spinal fractures.
Emergent Operative and Endovascular Interventions
List of Cases With Emergency Operative Interventions
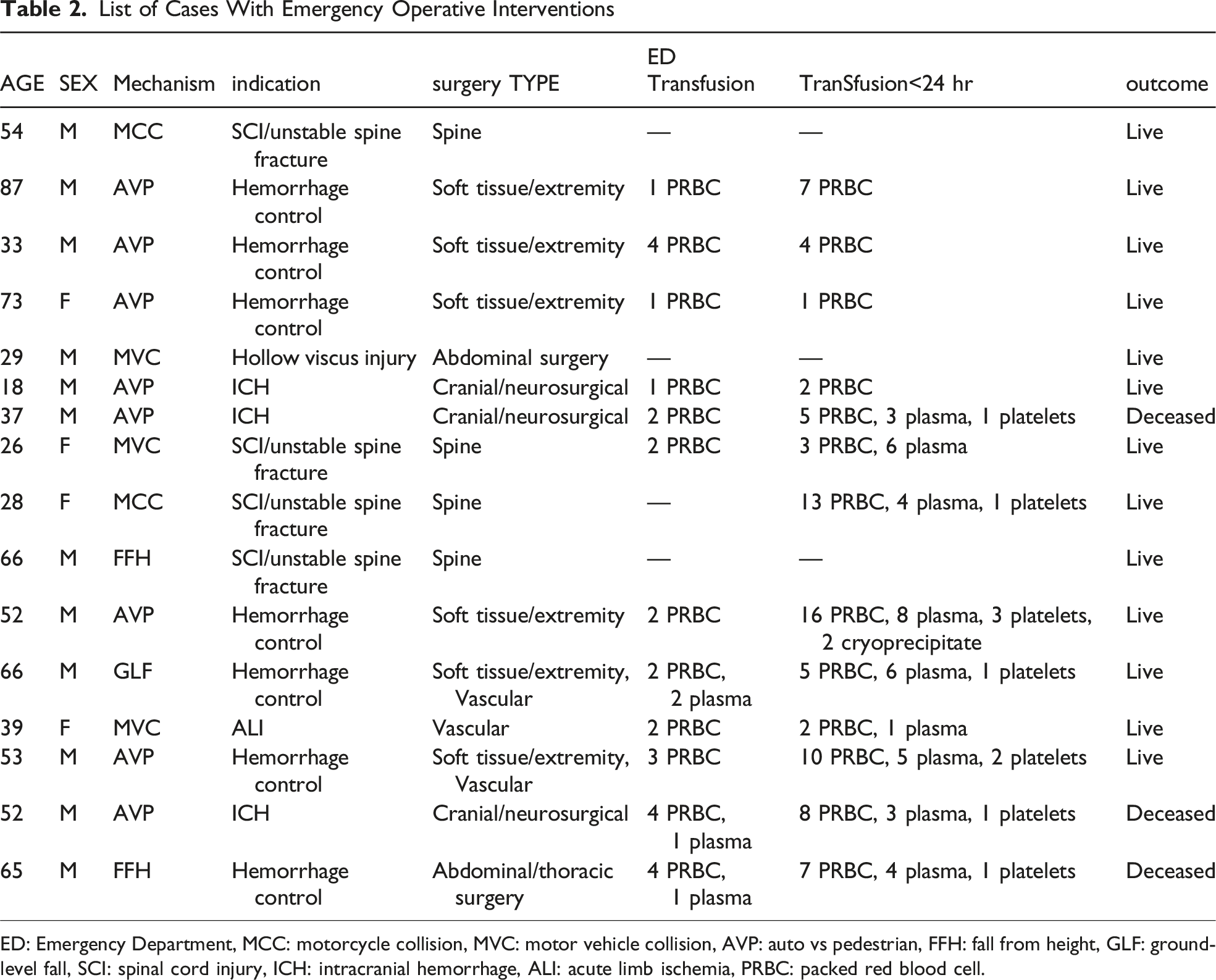
ED: Emergency Department, MCC: motorcycle collision, MVC: motor vehicle collision, AVP: auto vs pedestrian, FFH: fall from height, GLF: ground-level fall, SCI: spinal cord injury, ICH: intracranial hemorrhage, ALI: acute limb ischemia, PRBC: packed red blood cell.
List of Cases With Emergency Endovascular Interventions
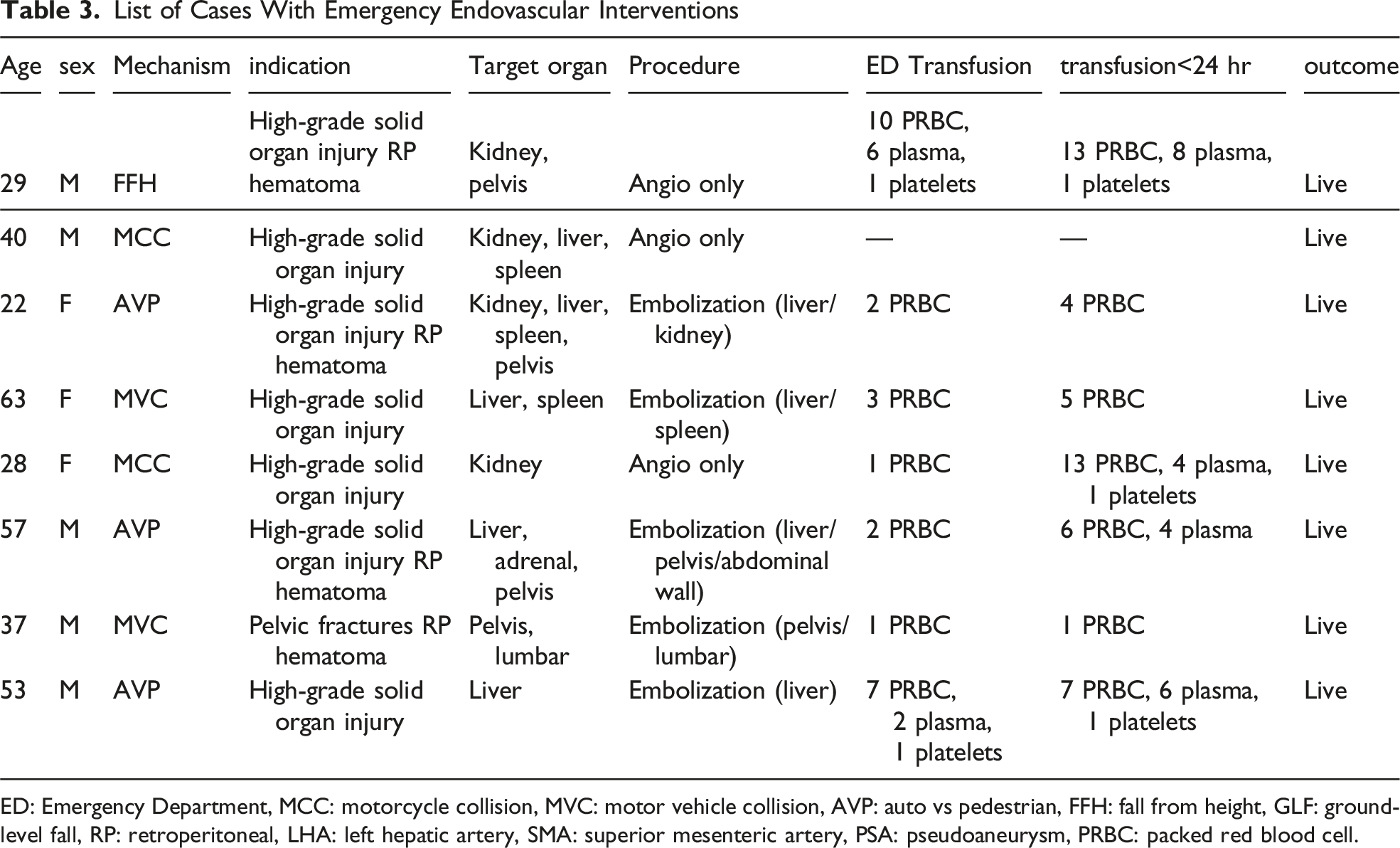
ED: Emergency Department, MCC: motorcycle collision, MVC: motor vehicle collision, AVP: auto vs pedestrian, FFH: fall from height, GLF: ground-level fall, RP: retroperitoneal, LHA: left hepatic artery, SMA: superior mesenteric artery, PSA: pseudoaneurysm, PRBC: packed red blood cell.
Clinical Outcomes
Overall, hypotensive blunt trauma patients with triple negative initial imaging demonstrated high rates of operative and endovascular intervention. Hemorrhagic and neurologic injuries were the predominant drivers of emergent surgical or endovascular intervention. The overall mortality rate was 5.5% (4/73), with all deaths due to severe neurologic injury. No fatalities were attributed to missed hemorrhage on CXR, PXR, or FAST. Following definitive diagnosis and management, most patients achieved hemodynamic stabilization.
Discussion
In this study including hypotensive blunt trauma patients with “triple negative,” namely, negative results on CXR, PXR, and FAST in the trauma bay, the patients frequently harbored critical injuries, with nearly one-third requiring emergency operative or endovascular interventions. Most patients in our cohort underwent CT after the initial assessment and resuscitation, which represents current practice patterns for identifying the source of hemodynamic instability and guiding definitive management. Advances in trauma resuscitation, particularly early and balanced blood transfusion, have led to improved hemodynamic stabilization, allowing more patients to undergo CT imaging. Our data suggest that the etiologies of triple negative hypotension most commonly fall into four categories: (1) hemorrhage from extremity, neck, or vascular injuries, (2) high spinal cord injuries, (3) solid organ injuries in the abdomen, and (4) severe traumatic brain injury. These phenotypes highlight that the cause of hypotension often lies outside the anatomical regions most effectively assessed by early adjunct imaging. Among patients requiring emergency interventions, ongoing hemorrhage from solid organ and extremity injuries, and intracranial and spinal cord pathology, were the most common injury patterns. These findings highlight the diagnostic limitations of early adjunct imaging and underscore the importance of maintaining a high index of suspicion for hemorrhagic and/or other types of shock states even when initial imaging is unrevealing.
CXR, PXR, and FAST are routinely used as the initial evaluation of hypotensive blunt trauma patients due to their speed, portability, and specificity for major thoracic, pelvic, and intraperitoneal injuries. Despite their clinical utility, all three modalities have important limitations, and the cause of hypotension may remain unidentified, creating diagnostic and clinical challenges. Consequently, negative findings across all three studies do not meaningfully reduce the likelihood of clinically significant hemorrhagic or neurologic pathology as the underlying cause of persistent hypotension. Currently, there is limited published data characterizing patients who remain hypotensive after all three adjuncts are negative. With no consensus regarding optimal next steps, this leads to wide practice variability across trauma centers.9,14-16 Clinicians may struggle with balancing the risks of transporting an unstable patient to CT, the potential morbidity associated with nontherapeutic laparotomy, and the consequences of missed hemorrhage or delayed recognition of non-hemorrhagic shock. This clinical ambiguity underscores a critical knowledge gap at a moment when decisional clarity is essential. The cumulative effect of these limitations is reflected in our cohort, where occult extremity hemorrhage, solid organ injury, and neurologic injury were common despite negative adjunct imaging.
Compared with CXR, PXR, and FAST, CT provides substantially higher sensitivity and specificity for detecting visceral, vascular, and neurologic injuries that may be occult on bedside imaging.17-22 This distinction is particularly relevant in cases of suspected neurogenic shock, as hemodynamic instability from spinal cord injury may develop within hours of injury rather than at initial presentation, 23 and neurosurgical intervention generally requires definitive preoperative imaging. 24 Traditional trauma teaching has emphasized reserving CT for hemodynamically stable patients or transient responders due to concerns regarding delayed hemorrhage control and prior studies reporting clinical deterioration and even cardiac arrest during imaging. 13 However, there is no universal consensus guiding CT use in hypotensive trauma patients with triple negative imaging.16,17,21,25,26 More recent studies have reported mixed results, with several demonstrating that CT can be safely performed in carefully selected unstable patients without delaying definitive hemorrhage control or increasing mortality.27-30 In our cohort, aggressive early resuscitation with blood products and judicious vasopressor support allowed 93.2% of patients to undergo CT following initial trauma evaluation, with roughly two-thirds receiving blood transfusions and 13.7% having MTP activation. No adverse events during CT scanning were observed in our study.
Although vasopressors have historically been avoided in early trauma resuscitation due to associations with worse outcomes in hemorrhagic shock,31,32 their selective use may be appropriate in carefully chosen patients. Nearly one-fifth of patients in our cohort required vasopressor support in the ED, and a small subset remained on vasopressors during CT imaging. Many of these patients were ultimately found to have severe TBI or spinal cord injuries, in whom hypotension is undesirable and maintenance of adequate mean arterial pressure is critical for cerebral and spinal cord perfusion. When clinical assessment strongly suggests neurogenic shock, advances in CT speed and accessibility support carefully monitored transport to the scanner with vasopressor support in selected patients. Emerging evidence supports the judicious use of vasopressors as a short-term adjunct within a damage control resuscitation framework, 33 and our findings are consistent with this evolving approach.
There are several limitations to this study. First, its retrospective design introduces the potential for reporting bias, as data was derived entirely from electronic medical records. Selection bias is also possible, as inclusion was limited to patients who survived long enough to undergo diagnostic evaluation in the ED, which may underestimate injury severity and skew the distribution of shock etiologies by excluding the most critically injured patients. 34 Second, while CXR and PXR images were reviewed retrospectively, FAST results were obtained from clinical documentation alone, without access to archived ultrasound images. Additionally, management decisions were not protocolized and varied by provider which introduces potential treatment bias. Third, the sample size was modest, with 73 identified over a 10-year period, limiting statistical power for subgroup analyses. Moreover, this single center study was conducted at a high-volume Level I trauma center, which may limit generalizability to centers with different resources, imaging availability, or patient populations. Finally, shock etiology in trauma is often multifactorial, and some patients likely had multiple concurrent contributors to hypotension that were difficult to disentangle retrospectively.
Conclusion
In hypotensive blunt trauma patients, negative CXR, PXR, and FAST imaging does not exclude life-threatening injuries. These high-risk “triple negative” patients frequently harbor clinically significant hemorrhagic or neurologic injuries that require urgent surgical or endovascular intervention. Recognition of this high-risk phenotype and timely escalation of diagnostic and therapeutic interventions are essential to improve patient outcomes.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.