
Abstract
Background
Return to operating room (ROR) is an important quality metric reflecting surgical outcomes. This study aimed to identify risk factors associated with ROR after lower extremity bypass (LEB) for chronic limb-threatening ischemia (CLTI).
Methods
A retrospective analysis was performed using the Society for Vascular Surgery Vascular Quality Initiative (SVS-VQI) database for patients undergoing LEB for CLTI between 2007 and 2020. Patients were divided into two groups: Group I (ROR) and Group II (No ROR). Univariate and multivariate regression analyses were conducted to identify risk factors, with significance set at P < .05.
Results
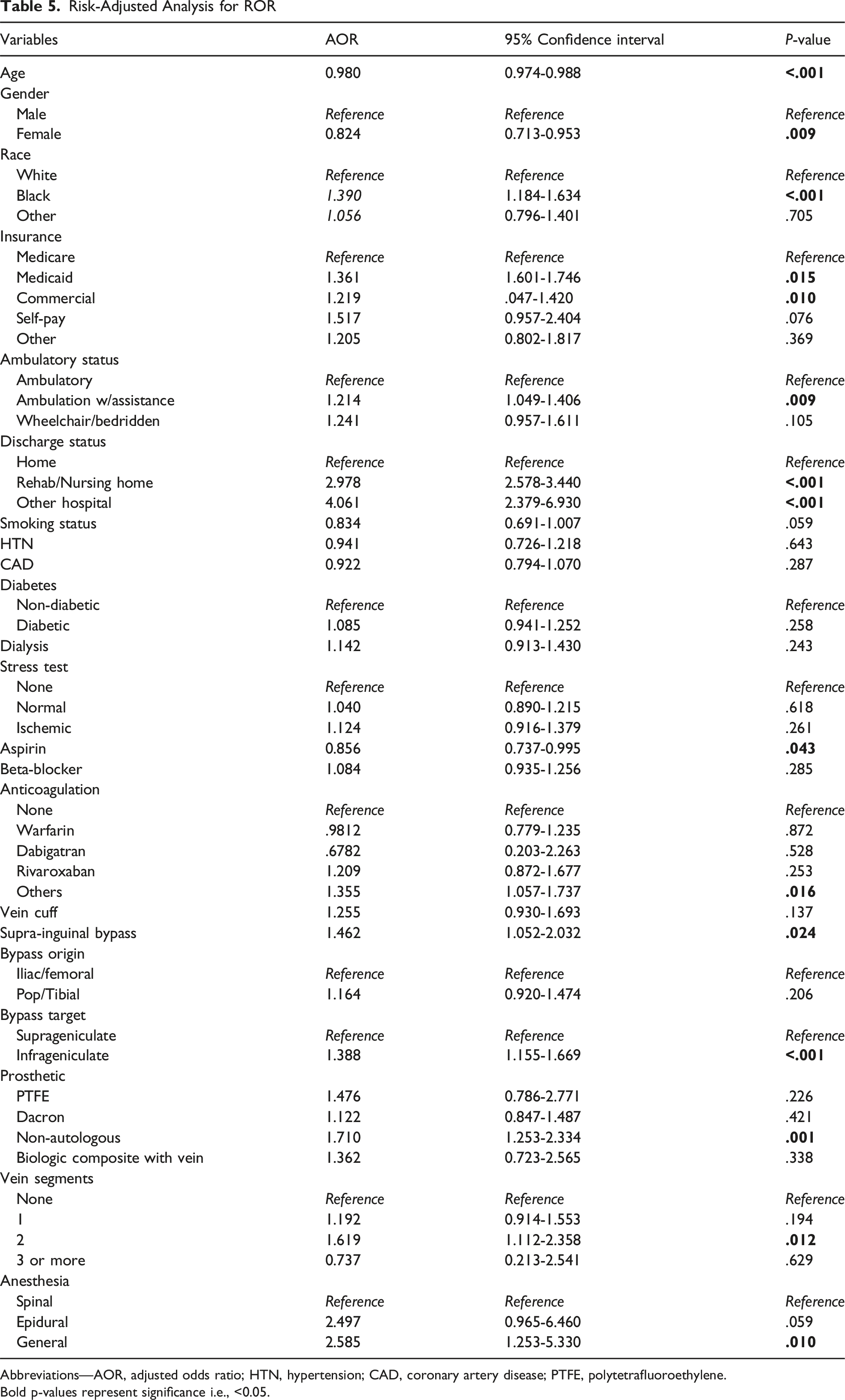
Among 10 800 patients, 1443 (14%) required ROR. Factors significantly associated with increased ROR risk included African American race (OR 1.39, CI [1.18-1.63]), Medicaid insurance (OR 1.36, CI [1.06-1.75]), ambulatory with assistance (OR 1.21, CI [1.05-1.41]), discharge to rehabilitation (OR 2.98, CI [2.58-3.44]), transfer to other hospitals (OR 4.06, CI [2.38-6.93]), concomitant bypass (OR 1.46, CI [1.05-2.03]), infrageniculate graft insertion (OR 1.39, CI [1.15-1.67]), non-autologous biologic conduit (OR 1.71, CI [1.25-2.33]), and general anesthesia (OR 2.58, CI [1.25-5.33]). Female sex (OR 0.82, CI [0.71-0.95]) and aspirin use (OR 0.85, CI [0.73-0.99]) were protective. Bypass thrombosis was the most common reason for ROR. No significant trend in ROR reduction was observed over the study period.
Conclusion
Multiple clinical and operative factors increase ROR risk after LEB for CLTI. Risk stratification and targeted interventions are essential to minimize complications and improve patient outcomes.
Keywords
Introduction
Chronic Limb-Threatening Ischemia (CLTI) represents the most severe form of peripheral artery disease (PAD), and is defined by presence of rest pain, ischemic ulcerations or gangrene. 1 It is estimated that roughly 11% of all patients with PAD suffer from CLTI and are at an extremely high risk for limb loss without revascularization. 2 Both endovascular interventions and lower extremity bypass (LEB) operations can be utilized for revascularization in patients with CLTI. BEST-CLI (Best Endovascular vs Best Surgical Therapy for Patients with Critical Limb Ischemia) trial is a randomized controlled trial which showed that for the patients with CLTI who have adequate saphenous vein for revascularization have improved outcomes when treated with LEB. 3 Despite being utilized for over five decades, there is considerable heterogeneity in the techniques utilized by vascular surgeons for performing LEB. Technical details of the LEB are important for successful operation. These include choosing appropriate inflow and outflow vessels, assessing conduit and its quality, determining graft configuration and length and configuring the plane where the bypass should be tunneled. Due to tenuous nature of the LEB, any error in judgment or technique leads to failure of the bypass. If the LEB fails acutely, it can have devastating consequences including limb loss. Most of these errors need to be surgically corrected promptly to maintain bypass patency and preserve limb. An unplanned return to the operating room (ROR) after the operation is considered a metric which reflects quality of the index operation and has been shown to be associated with worse outcomes. Unplanned return to the operating room after LEB is usually multifactorial and may represent errors in clinical judgment and or technical failures during the index operation. Previously published literature describes that unplanned return to the operating room is also associated with increased risk of unplanned readmission to the hospital. 4
This study aims to analyze the Vascular Quality Initiative (VQI) database to identify the patients who required unplanned return to the operating room after LEB for CLTI and to identify the factors associated with it. While some of the factors may not be modifiable, it is pertinent for practicing vascular surgeons to identify the factors which can be modified to reduce the risk of unplanned return to the operating room. More importantly, we seek to determine the intraoperative findings during the re-do operations and expand on the potential risk factors for developing these complications and focus on strategies which can be utilized to prevent such occurrences in the future.
Methods
Data Source
A retrospective analysis was performed for all patients undergoing LEB for CLTI in the Society for Vascular Surgery Quality Initiative (VQI) database between 2007 and 2020. The VQI database is a registry that contains operative information from >800 participating institutions across North America and undergoes regular audits allowing each institution to have access to all regional data in addition to their own. The Pennsylvania State University College of Medicine Institutional Review Board approved the current study (IRB No. STUDY00024186). Since patient records were kept confidential and no intervention was conducted, the Institutional Review Board waived the requirement for patient consent.
Study Groups
In the present analysis, we focused on the patient characteristics and intraoperative variables and explored risk factors associated with unplanned ROR in patients undergoing LEB surgery for the diagnosis of CLTI. Patients were divided into two groups: Group I composed of patients who underwent an unplanned operation after the LEB surgery, and Group II consisted of patients who did not need an unplanned operation after the index LEB surgery. Return to Operating Room (ROR) was defined as any unplanned reoperation occurring during the earlier postoperative period that can be index hospitalization or within 30 days of the index procedure.
Inclusion Criteria
A total of 66 142 patients underwent LEB for CLTI in the VQI registry between 2007 and 2020. Patients with age <18, indication for bypass other than CLTI, urgent operations, missing return to OR data information, non-home living status, non-occlusive disease, transfers, and non-CLTI were excluded. This resulted in 55 342 patients being excluded and 10 800 patients included in our study, as shown in Figure 1. Sample inclusion and exclusion criteria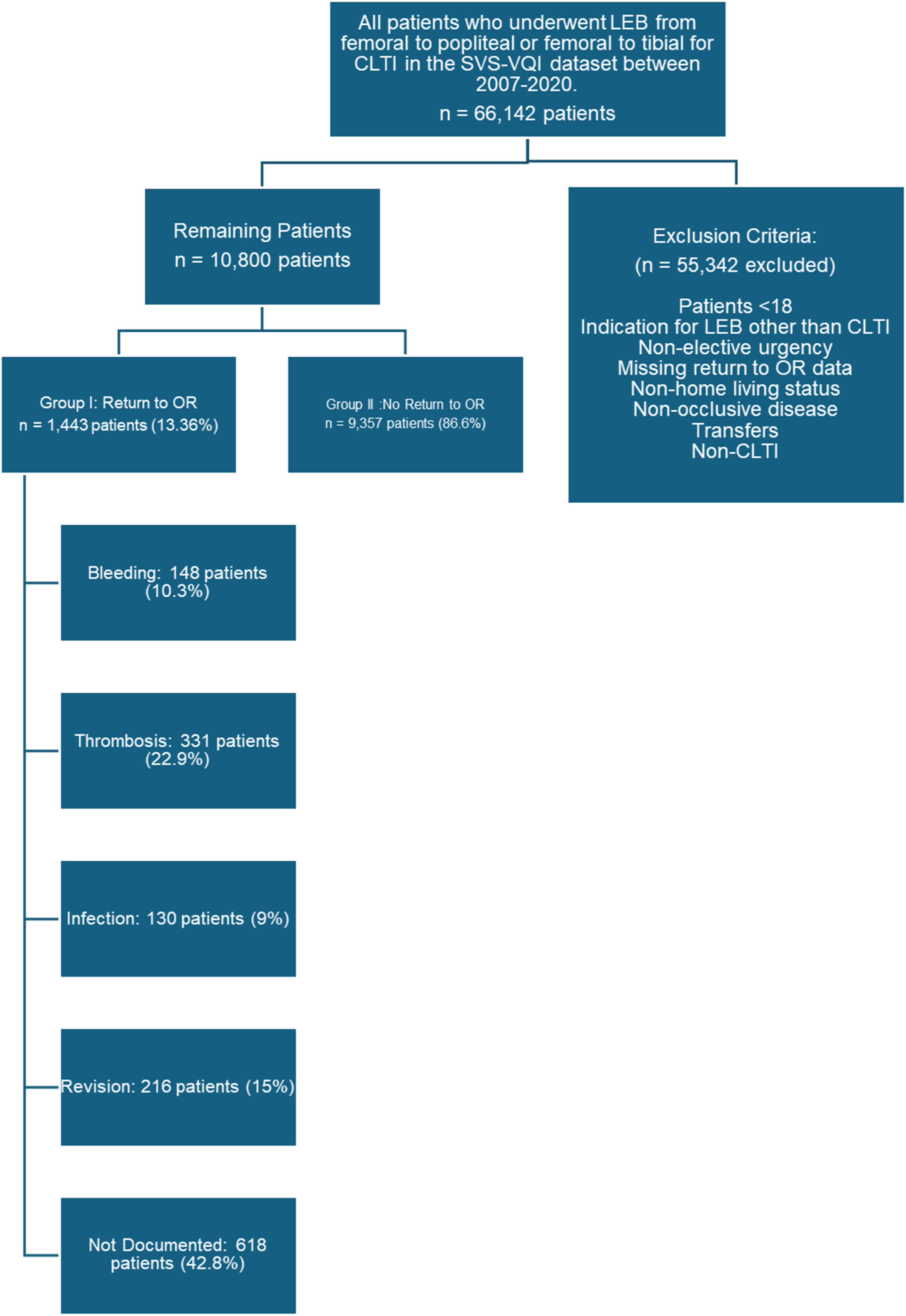
Patient and Procedural Characteristics
The patient features such as demographic and preoperative variables (ie, age, gender, race, insurance, ambulatory status, discharge status, and smoking status), medical history (ie, hypertension, diabetes, coronary artery disease, dialysis, COPD, HbA1c, and preoperative functional status), surgical history (ie, previous arterial bypass, carotid stenting, aneurysmal repair, percutaneous transluminal angioplasty, major amputation, and prior coronary artery bypass grafting), preoperative medication history (ie, aspirin, P2Y12, statins, beta-blocker, ACE-inhibitor, and anticoagulants) and Fontaine classification of PAD (rest pain and tissue loss) were analyzed. We also explored intraoperative characteristics such as vein graft location, vein harvest incision, vein cuff, sequential graft, anesthesia (spinal, epidural, general), groin incision, procedure time, concomitant procedure, graft origin, recipient site, graft vein type, vein segment, and conduit type (synthetic comprising of PTFE and Dacron, non-autologous biologic and composite with vein). The major risk factors leading to ROR were identified in Group I, and the incidence of each cause was compared among the two groups.
Statistical Analysis
All statistical analyses were performed using Stata 18.0 IC version (College Station, TX). Categorical variables were assessed using the Pearson Chi-Square test to evaluate differences between the two study groups. Continuous variables were tested using the t-test, after verifying the normality of their distribution, to compare between the groups. A multivariate analysis was performed using logistic regression analysis to study the risk factors associated with the ROR and were selected if these factors were observed to be statistically significant in univariate analysis. The effect estimates of these risk factors were reported in adjusted odds ratios (AOR) and corresponding 95% confidence intervals. A trends analysis was also performed to test for the change in the occurrence of ROR during the study period, All the analyses were deemed significant if the P-value was found to be <.05.
Results
Among the 10 800 patients who were included in the present study, 1443 (13.4%) returned to the OR following lower extremity bypass surgery (Group I), while 9357 (86.6%) did not return to the OR following lower extremity bypass surgery (Group II). The trends of ROR over the course of years show that the incidence of unplanned ROR has not decreased with the passage of time. These trends are summarized in Figure 2. Annual proportion of patients with and without unplanned return to the operating room (ROR) following lower extremity bypass for chronic limb-threatening ischemia (CLTI) in the vascular quality initiative (VQI) registry (2007-2020). The figure represents year-specific proportions and does not reflect cumulative incidence. No statistically significant temporal trend was observed (P = .081)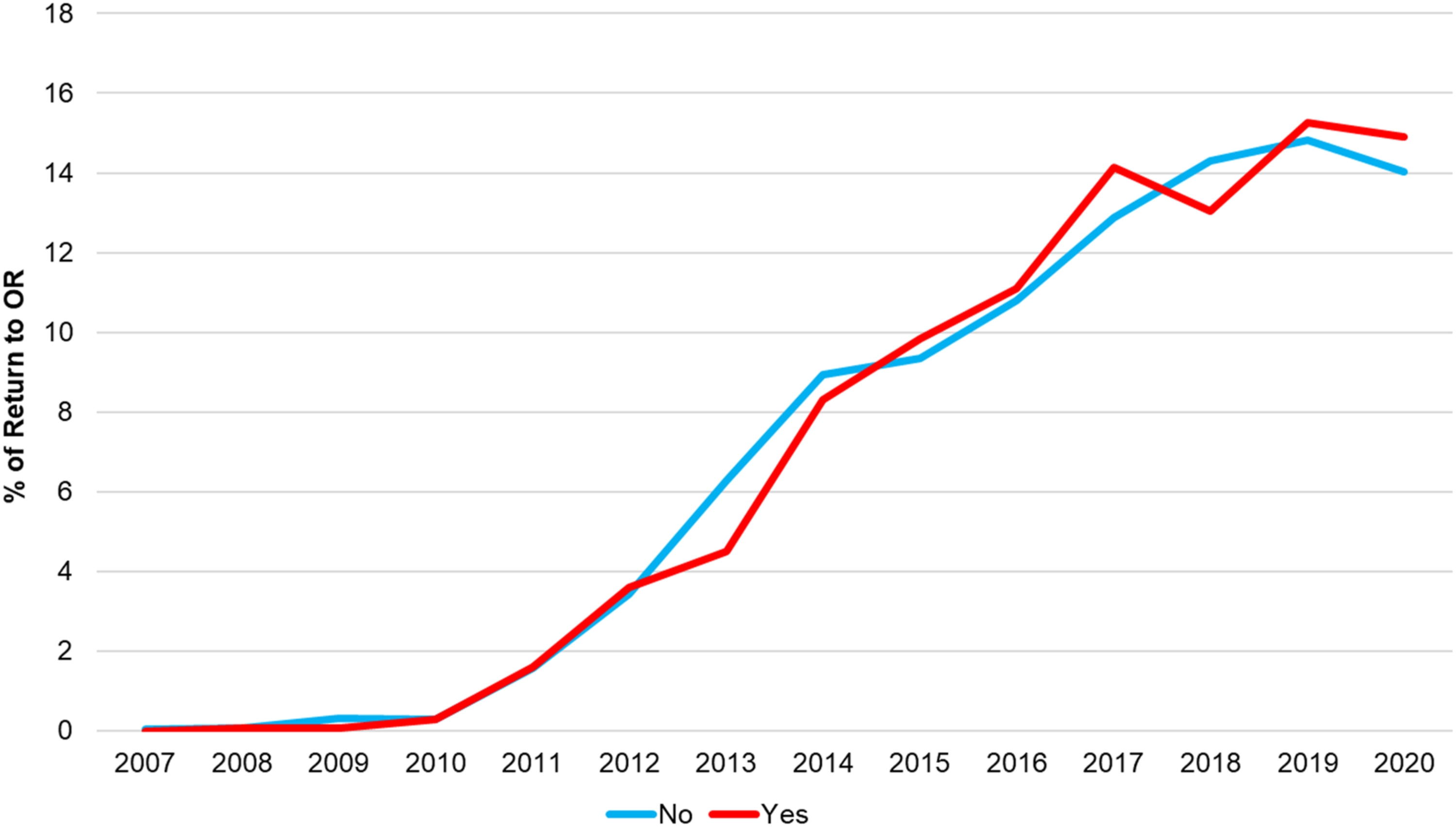
Patient Characteristics
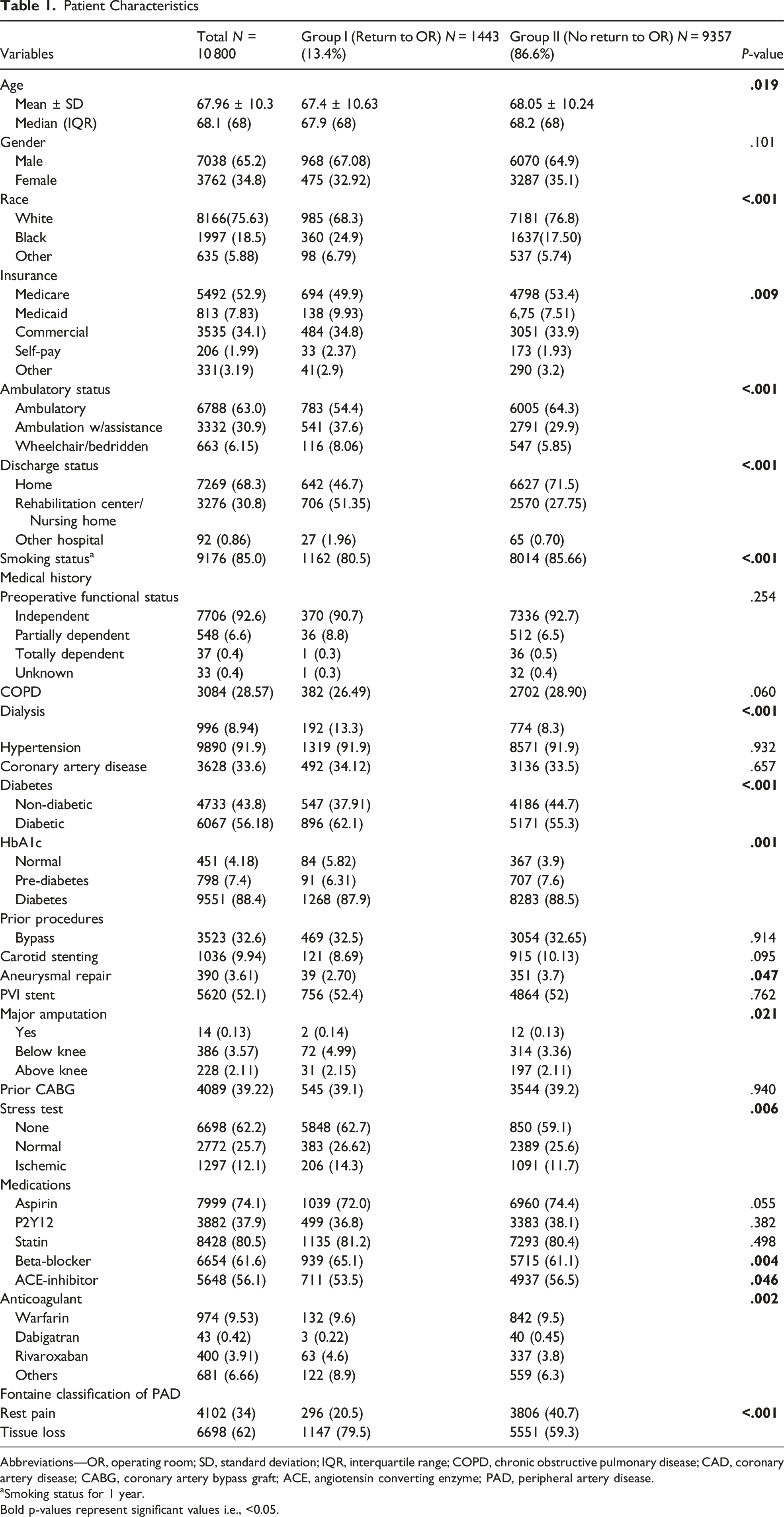
Abbreviations—OR, operating room; SD, standard deviation; IQR, interquartile range; COPD, chronic obstructive pulmonary disease; CAD, coronary artery disease; CABG, coronary artery bypass graft; ACE, angiotensin converting enzyme; PAD, peripheral artery disease.
aSmoking status for 1 year. Bold p-values represent significant values i.e., <0.05.
Intraoperative Characteristics
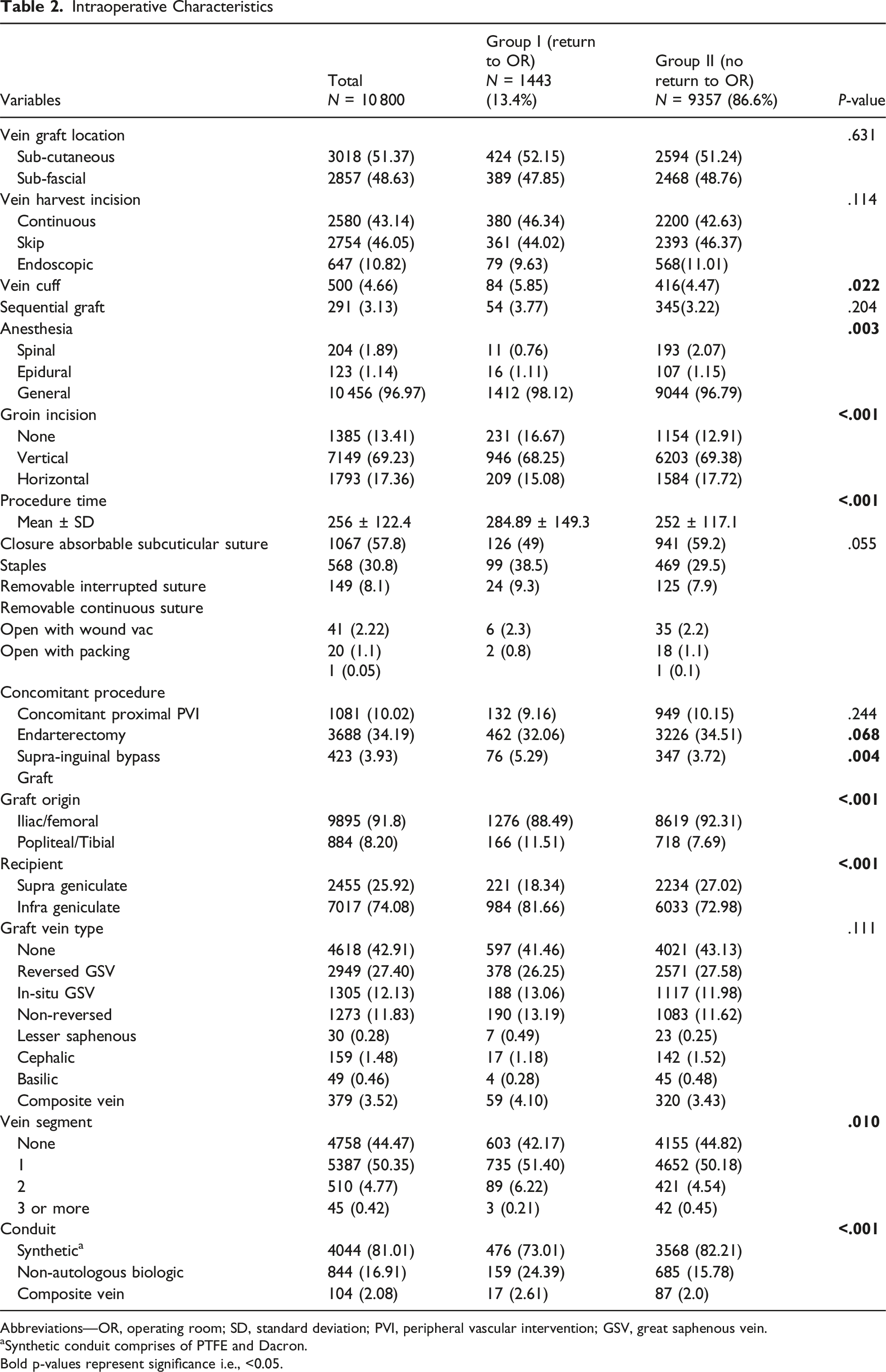
Abbreviations—OR, operating room; SD, standard deviation; PVI, peripheral vascular intervention; GSV, great saphenous vein.
aSynthetic conduit comprises of PTFE and Dacron. Bold p-values represent significance i.e., <0.05.
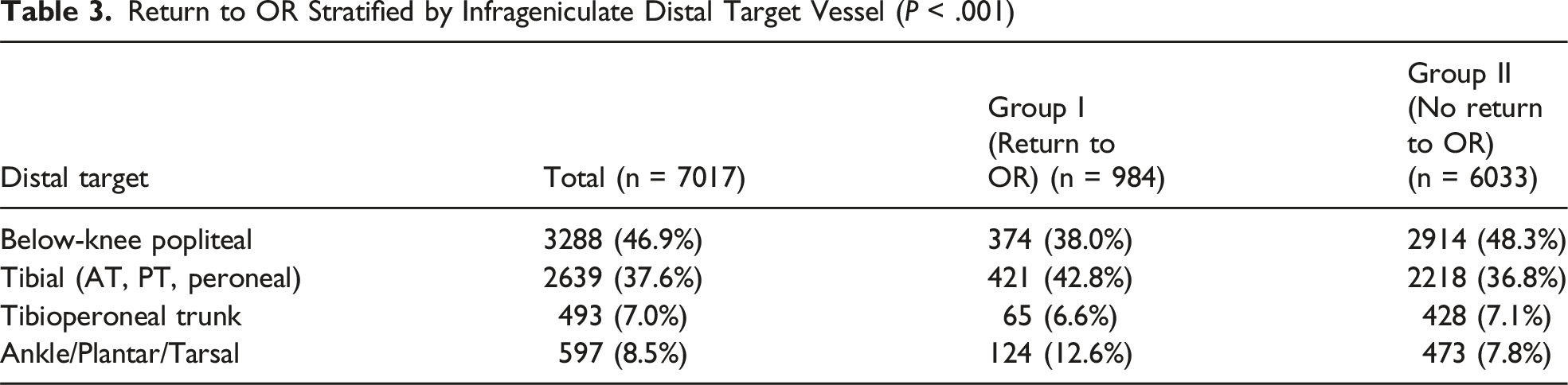
Return to OR Stratified by Infrageniculate Distal Target Vessel (P < .001)
Causes for Return to OR: By stratifying the causes of ROR for the patients within Group I to understand the underlying problems, we were able to identify the following reasons for ROR: Thrombosis (n = 331, 22.9%), Bypass Revision (n = 216, 15%), Bleeding (n = 148, 10.3%), Infection (n = 130, 9%) and the cause was not documented in 618 patients (42.8%). This data is illustrated in Figure 1. The sub-analysis to understand the causes for Return to OR among different intraprocedural variables revealed a distinct pattern.
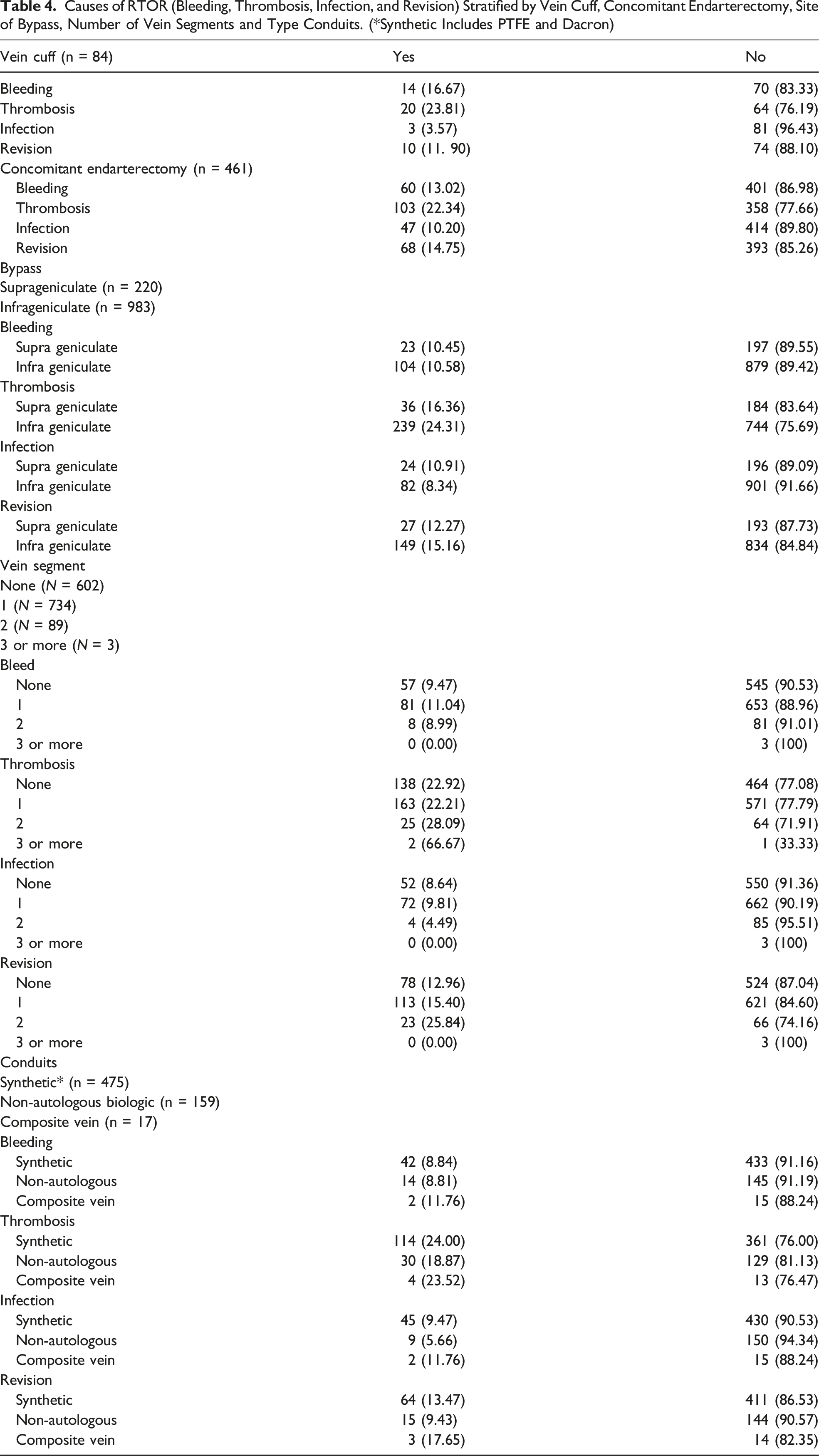
Causes of RTOR (Bleeding, Thrombosis, Infection, and Revision) Stratified by Vein Cuff, Concomitant Endarterectomy, Site of Bypass, Number of Vein Segments and Type Conduits. (*Synthetic Includes PTFE and Dacron)
Multivariate Analysis to Assess Risk Factors Associated With ROR
Risk-Adjusted Analysis for ROR
Abbreviations—AOR, adjusted odds ratio; HTN, hypertension; CAD, coronary artery disease; PTFE, polytetrafluoroethylene. Bold p-values represent significance i.e., <0.05.
Discussion
This retrospective review explores preoperative and intraoperative factors associated with unplanned ROR for patients undergoing peripheral arterial bypasses to treat CLTI. Of the 10.800 patients undergoing LEB operation for the treatment of CLTI, 1443 (13.36%) patients had unplanned ROR. Overall, the trends over the course of years show that the incidence of unplanned ROR has not decreased with the passage of time. Risk-adjusted multivariant analysis identified following factors to be associated with an increased risk of ROR: male gender, black race, Medicaid insurance status, ambulation with assistance, non-home discharge, use of aspirin, infrageniculate bypass, non-autologous biologic conduit, multi-segment vein bypass and use of general anesthesia. We were interested in knowing the intraoperative factors which predispose a patient to the increased risk of unplanned ROR. Following intraoperative factors were found to be associated an increased risk of ROR: use of vein cuff, use of general anesthesia, longer duration of operation, concomitant endarterectomy, concomitant supra-inguinal bypass, graft origin to be popliteal or tibial, graft target to be an infrageniculate artery, more than one vein segment and non-autologous biologic conduit. Within the subgroup of the infrageniculate bypasses, patients with distal target vessel to be tibial or more distal had much higher risk of ROR as compared to patients with below-knee popliteal artery to be the recipient site for the graft. Further sub-analysis of intraoperative factors associated with increased risk of ROR showed that among patients with vein cuff, the most common reason for ROR was thrombosis, among patients with concomitant endarterectomy, the most common reason for ROR was thrombosis, among the patients with infrageniculate bypasses, the most common reason for ROR was thrombosis, those who had one venous segment were more likely to ROR due to bleeding (11%) and infection (9.8%): those who had two vein segments were more likely to ROR due to need for revision of the bypass (25.8%) and those who had three or more vein segments used for the bypass were more likely to ROR due to bypass thrombosis, and for patients who underwent lower extremity bypasses with non-vein conduits, those with synthetic conduit were more likely to ROR due to thrombosis (24%), those with composite with vein conduit were more likely to ROR due to bleeding (11.76%), infection (11.76%) and need for bypass revision (17.65%).
ROR serves as a pivotal quality metric in patient care and has been reported as a major prognostic marker for clinical outcomes. Extensive research studies based on the National Quality Surgical Quality Improvement Program (NSQIP) database have discussed ROR and its variability for different surgical procedures.3,5-8 While previously published research has clearly identified ROR as a quality metric which has been found to be associated with poor surgical outcomes, the precise cause of ROR is a subject, which hasn’t been explored in detail before. Within the vascular surgeries documented in NSQIP registries, carotid endarterectomy is associated with the lowest risk of ROR (3.1%), while some other operations such as embolectomies for treatment of acute ischemia and abdominal vascular reconstructions have been associated with significantly higher risk of ROR (18.2% and 14.4%, respectively). Furthermore, it is also known that patients with ROR after vascular surgery are more likely to have higher risks of postoperative complications, mortality, and failure to rescue.5,6 In another investigation, leveraging a comprehensive national cohort of readmissions after LEB, the incidence of unplanned ROR among patients undergoing LEB’s was 17.6%. 9 While some factors such as gender and race are not modifiable, our findings suggest that several intraoperative factors such as concomitant endarterectomy and use of vein cuff may be modifiable by paying meticulous attention to technical details of the operation. The current analysis shows that thrombosis is the most common reason for ROR, highlighting the importance of technical details of the operation, ensuring adequate anticoagulation throughout the procedure and ensuring optimal anticoagulation in the postoperative time. Every effort should be made to pay attention to modifiable risk factors to minimize the incidence of unplanned ROR.
Previously, our group meticulously elucidated a spectrum of factors intricately linked to ROR after aortic surgery, which gives insights for a judicious implementation for risk stratification.4,10-12 Consistent with the subject, data sources like VQI can be utilized to analyze ROR among patients undergoing LEB. Smith et al reported a meta-analysis of factors associated with early readmissions after lower extremity revascularization, including endovascular procedures, which ranged from female sex, dependent ambulatory status, and various comorbidities; however, none of the reported literature was from VQI. 13 It is noteworthy that our group’s prior meta-analysis identified an 18% cumulative risk of readmission following LEB, with a higher likelihood among patients with coexisting congestive heart failure and hypertension. In a separate study, we also found that prolonged operative time was significantly associated with increased risk of ROR.14,15 A study by Hamouda et al demonstrated that staple skin closure was independently associated with a higher risk of ROR following lower extremity bypass. In present analysis, a similar trend was observed with a higher proportion of ROR events in patients who underwent staple closure compared to those with suture-based techniques. However, it was found to be marginally insignificant and was therefore not included in multivariable analysis. 16 Interestingly, this analysis identified preoperative aspirin use as being associated with a lower risk of ROR. While causality cannot be inferred from observational data, this finding is biologically plausible. Aspirin, through its antiplatelet and anti-inflammatory effects, likely contributes to improved graft patency, reduced perioperative thrombosis, and fewer ischemic complications, all of which may reduce the need for early reintervention. The insights from existing literature, coupled with present analyses, extend beyond the purview of vascular surgeons and steps into shaping strategies in risk mitigation and cost containment in the broader perspective of health care delivery.
A recent comprehensive meta-analysis by Conte et al of long-term outcomes after LEB for CLTI helps us frame this study within the context of vascular surgery outcomes and improvement efforts. The meta-analysis revealed that although there is improvement in technical success rates for LEB, the rates of Major Adverse Limb Event (MALE) and perioperative complications remain significant. 17 This highlights the importance of this study’s findings, which aimed to identify risk factors for ROR, as ROR can increase incidence of postoperative complications, providing further granularity in understanding factors underlying these adverse outcomes. The implications of our study extend beyond the immediate postoperative period, with significant implications for long-term outcomes for patients and increased health care resource utilization. 18 Focusing on modifiable risk factors, such as optimizing perioperative management for patients with dependent ambulatory status or those requiring complex bypass procedures, could allow health care providers to decrease the incidence of ROR and its corresponding economic burden. 19
The association of African American race and Medicaid insurance with increased frequency of ROR highlights the critical role of race and SES in surgical outcomes. Our study adds to the already collected studies regarding racial disparities which have shown that many African American patients suffer from increased incidence of postoperative complications and mortality, probably due to inadequate access to care, potential comorbidities, or decreased quality of health care facilities available to them. 20 Medicaid insurance, often a surrogate marker for lower SES, further enhances these disparities by decreasing access to high-quality postoperative care and rehabilitation services. The interplay of race and SES underscores the importance of formulating quality initiatives and targeted interventions to address these inequities and improve outcomes in these vulnerable populations. Furthermore, the trend analysis from our study shows that despite the data collection over the years and various publications regarding many vascular procedures, the ROR rates have not declined significantly over the years, as shown in Figure 2. This issue’s persistence implies that it is not enough to collect data; active implementation of evidence-based interventions and quality improvement initiatives is needed. The lack of progress in reducing ROR rates indicates a potential gap in translating the research into clinical practice and provides a basis for systemic changes that would enable quality improvement in the care being provided to patients undergoing LEB. Additionally, the trend analysis depicts the brutal reality of the everyday life of vascular surgeons, who are still fighting to eradicate this issue.
This study has its limitations due to its retrospective nature. The VQI dataset has predetermined variables, which limits the scope of information gathered. Although our statistical analysis adjusted the results for several variables, some confounding variables could still exist. This also means we are limited in our investigation because the predetermined variables restrict the establishment of cause-and-effect relationships. The most significant limitation of our study is the selection bias due to VQI being a self-reported and optional database for hospitals and physicians. Additionally, a large patient population (10 800) was captured from the VQI database in this study; this could mean that some variables, although statistically significant, were clinically irrelevant. As with most studies conducted using an extensive database, the interpretation of results should be done cautiously, and clinical judgment should be used when applying the results in real-life scenarios. However, using a comprehensive database like VQI enriches the study’s foundation. Being a sizeable surgical database accessible to most hospitals and surgeons for analyzing outcomes or risk factors for various vascular procedures adds to the study’s strength. The dataset offers detailed insight into pre-, intra-, and postoperative variables and allows for generalizability to a wide range of populations across the United States and beyond, with broad clinical applications. Finally, the methodology from this study using the VQI database is reproducible, as shown in prior studies from the same database, which ensures the study’s reliability and applicability.
Conclusion
This study highlights the interaction of various risk factors resulting in ROR following LEB for CLTI. The findings emphasize the need for comprehensive risk stratification with targeted interventions to help mitigate the modifiable risk factors. Further research on developing and implementing standardized care and quality improvement initiatives will help improve patient outcomes while reducing the economic burden from ROR in vascular surgery.
Footnotes
Author Note
Abstract was presented as a poster presentation at 2024 Vascular Annual Meeting (VAM). Abdul Wasay Paracha and Ahsan Zil-E-Ali share the first authorship and contributed equally to this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.