
Abstract
Background
Unplanned returns to the operating room (uROR) are associated with worse outcomes including increased complications and length of stay (LOS) in adults. However, the incidence and predictors of uROR for pediatric trauma patients (PTPs) are unknown. This study aimed to identify predictors of uROR for PTPs.
Methods
The 2017-2019 Trauma Quality Improvement Program database was queried for PTPs 1-16 years-old to compare patients with uROR to those without uROR. Multivariable logistic regression analysis was performed.
Results
From 44 711 PTPs identified, 299 (.7%) underwent uROR. Pediatric trauma patients requiring uROR were older (14 vs 8 years old, P < .001), had a higher rate and associated risk of mortality (8.7% vs 1.4%, P < .001) (OR 6.67, CI 4.43-10.05, P < .001) as well as increased complications including surgical infection (16.4% vs .2%, P < .001) and compartment syndrome (4.7% vs .1%, P < .001). Patients undergoing uROR had increased LOS (18 vs 2 days, P < .001) and intensive care unit LOS (9 vs 3 days, P < .001). Independent associated risk factors for uROR included rectal injury (OR 4.54, CI 2.28-9.04, P < .001), brain injury (OR 3.68, CI 2.71-5.00, P < .001), and gunshot wounds (OR 2.55, CI 1.83-3.56, P < .001).
Discussion
The incidence of uROR was <1% for PTPs. However, patients requiring uROR had increased LOS and associated risk of death compared to those without uROR. Predictors of uROR included gunshot wounds and injuries to the rectum and brain. Patients with these risk factors should be counseled with efforts made to improve care for these high-risk populations.
Introduction
Traumatic injury is the leading cause of morbidity and mortality in children and accounts for over 180,000 hospital admissions each year. 1 Many pediatric trauma patients (PTPs) will require an operative intervention. In some of these cases, post-operative complications necessitate an unplanned return to the operating room (uROR). In adults, post-surgical complications that require uROR most often arise from infections, vascular complications, ischemic organ damage, or poor wound healing. 2 Furthermore, adult trauma patients with uROR have an increased risk of morbidity, mortality, and prolonged length of stay (LOS), compared to those without uROR. 3
Although factors predicting uROR in adult trauma patients have been previously described, 3 the incidence of uROR in PTPs and the risk factors associated with uROR in this population are unknown. Therefore, this study aimed to identify risk factors associated with uROR in PTPs using a national database, hypothesizing that PTPs with uROR have increased LOS and complications.
Methods
This study was approved by the institutional review board, and a waiver of consent granted due to use of the Trauma Quality Improvement Program (TQIP) database, a deidentified national database.4,5 Trauma Quality Improvement Program was queried for PTPs between 1 and 16 years-old from 2017 to 2019 who were admitted directly to the operating room from the emergency department (ED). All operative procedures fitting this criterion were included. Patients not admitted directly to the operating room from the ED were excluded. Patients requiring an uROR were compared to patients without uROR. An uROR was defined by TQIP as one or more unplanned surgeries following the patient’s initial surgery for a similar or related previous procedure that occurred during index hospitalization. Differentiation between unplanned and planned operations in the database was based on data sourced from hospital records. No distinctions were made between patients requiring a single uROR vs multiple uROR.
Demographic variables collected include age, sex, and comorbidities including diabetes, smoking, and substance use. The injury profile was also evaluated and included the mechanism of injury, injury severity score (ISS), and individual injury types such as traumatic brain injury (TBI) and injury to the rectum. Outcomes measured include unplanned intensive care unit (ICU) admission at any time during the initial hospitalization, hospital LOS, ICU LOS, and complications including cerebrovascular accident (CVA), ventilator-associated pneumonia (VAP), cardiac arrest, surgical site infections (SSI), venous thromboembolism (VTE), acute kidney injury (AKI), compartment syndrome, catheter-associated urinary tract infection (UTI), central-line-associated bloodstream infection, and sepsis.
Continuous variables were reported as medians with interquartile ranges and compared using a Mann-Whitney U test. Categorical data were reported as percentages, while continuous data were presented as medians with interquartile range. All P-values were two-sided, with a statistical significance level of <.05. In addition, a multiple logistic regression analysis was performed to identify independent predictors of uROR. Using a univariable logistic regression model, variables with P < .20 were selected for further analysis using a multivariable logistic regression model. This was reported with an odds ratio (OR) with 95% confidence intervals (CIs), and P < .05 was considered statistically significant. All analyses were performed with IBM SPSS Statistics for Windows (Version 28, IBM Corp., Armonk, NY).
Results
Demographics and Injury Profile of Pediatric Trauma Patients With and Without uROR.
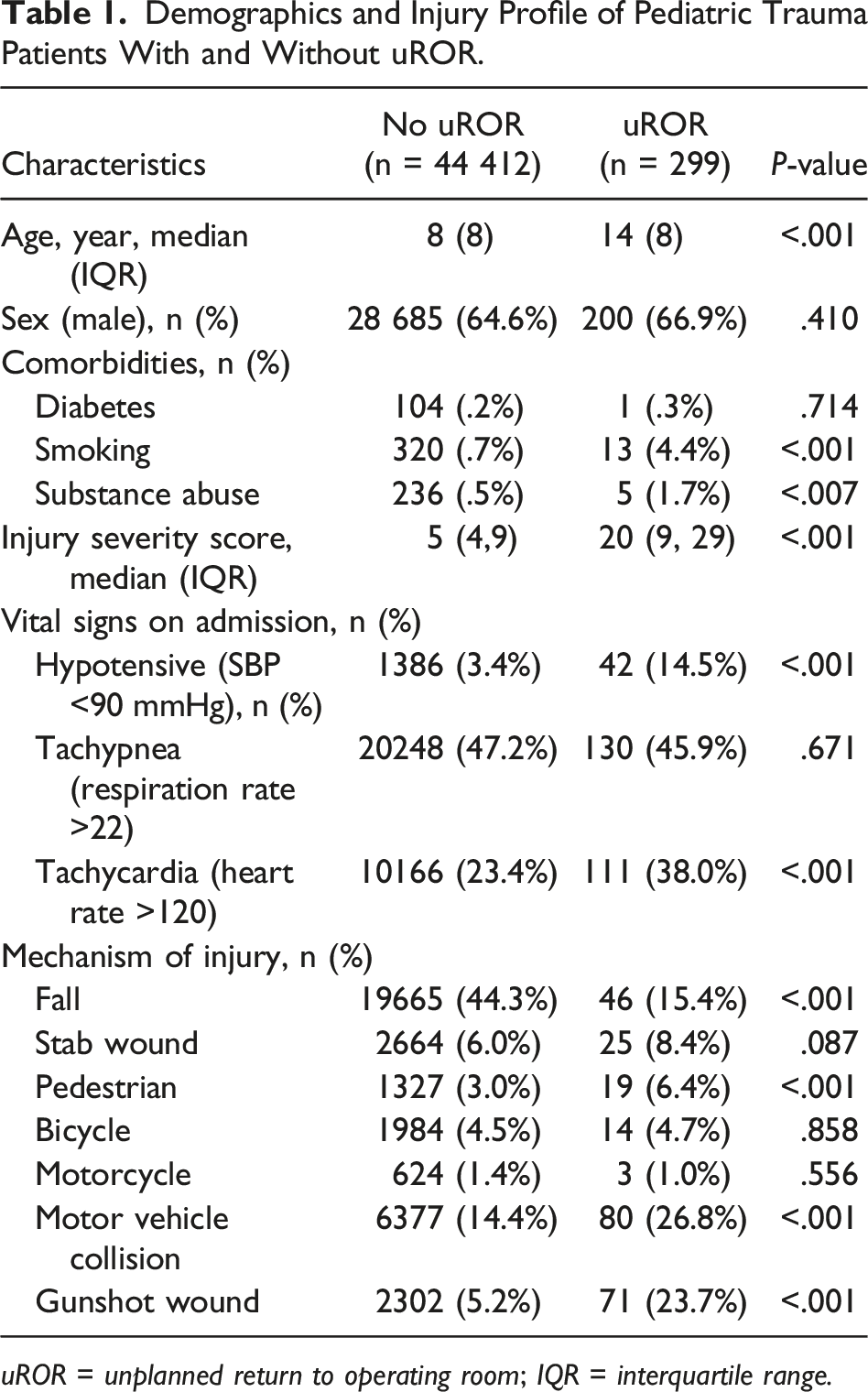
uROR = unplanned return to operating room; IQR = interquartile range.
Injuries in Pediatric Trauma Patients With and Without uROR.
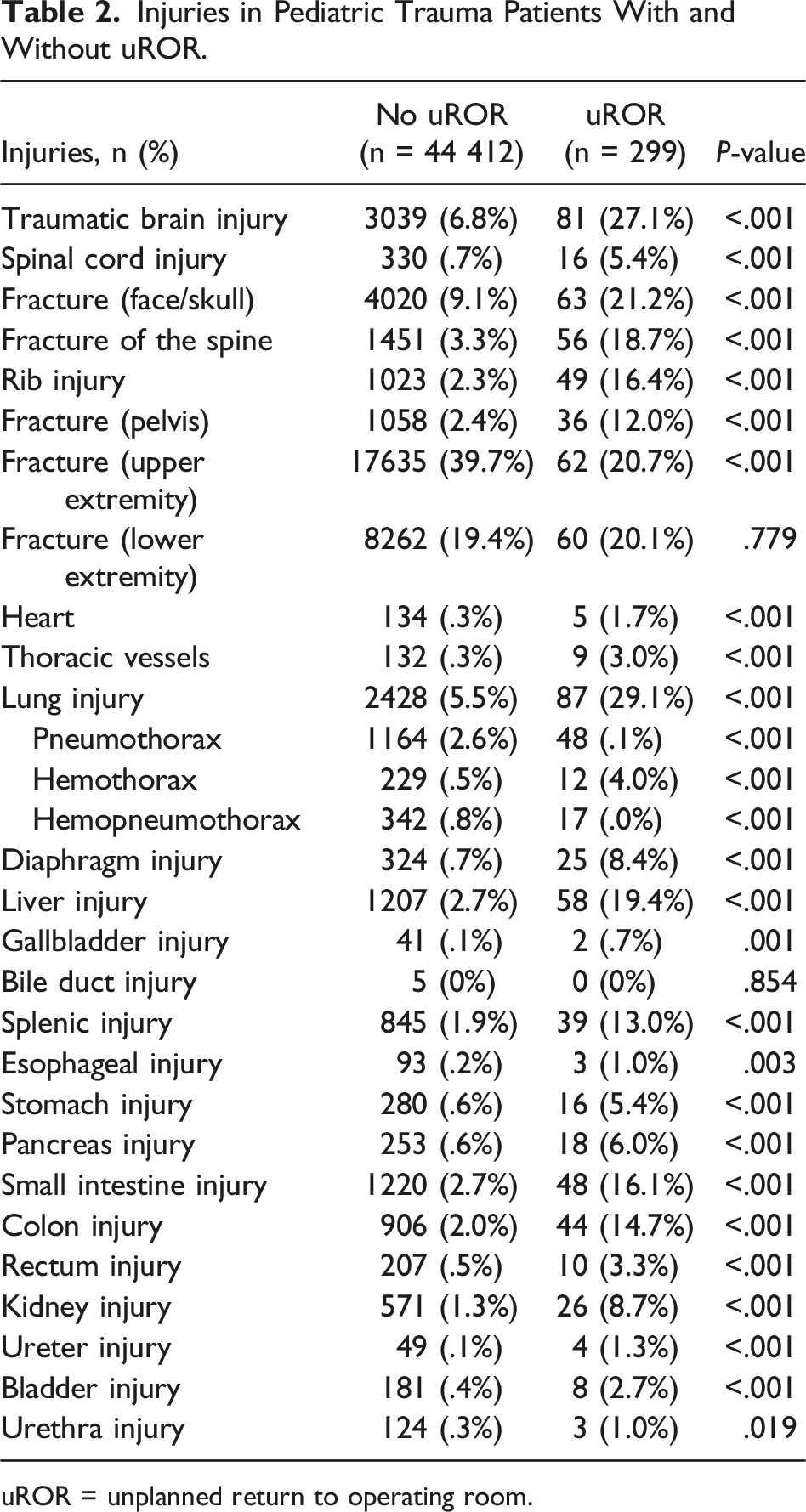
uROR = unplanned return to operating room.
Outcomes in Patients Undergoing uROR.
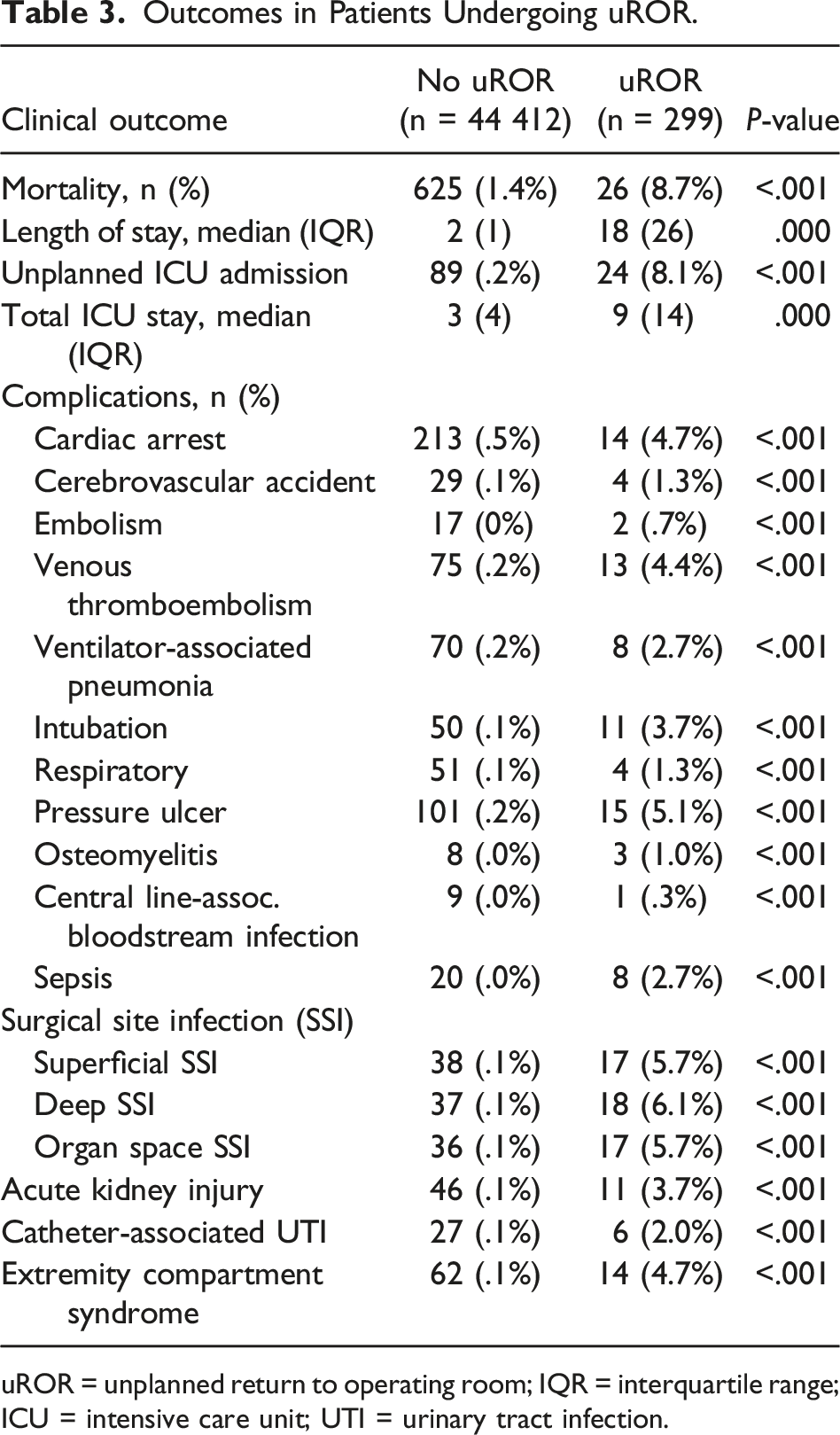
uROR = unplanned return to operating room; IQR = interquartile range; ICU = intensive care unit; UTI = urinary tract infection.
Logistic Regression Analysis of Risk Factors for uROR.
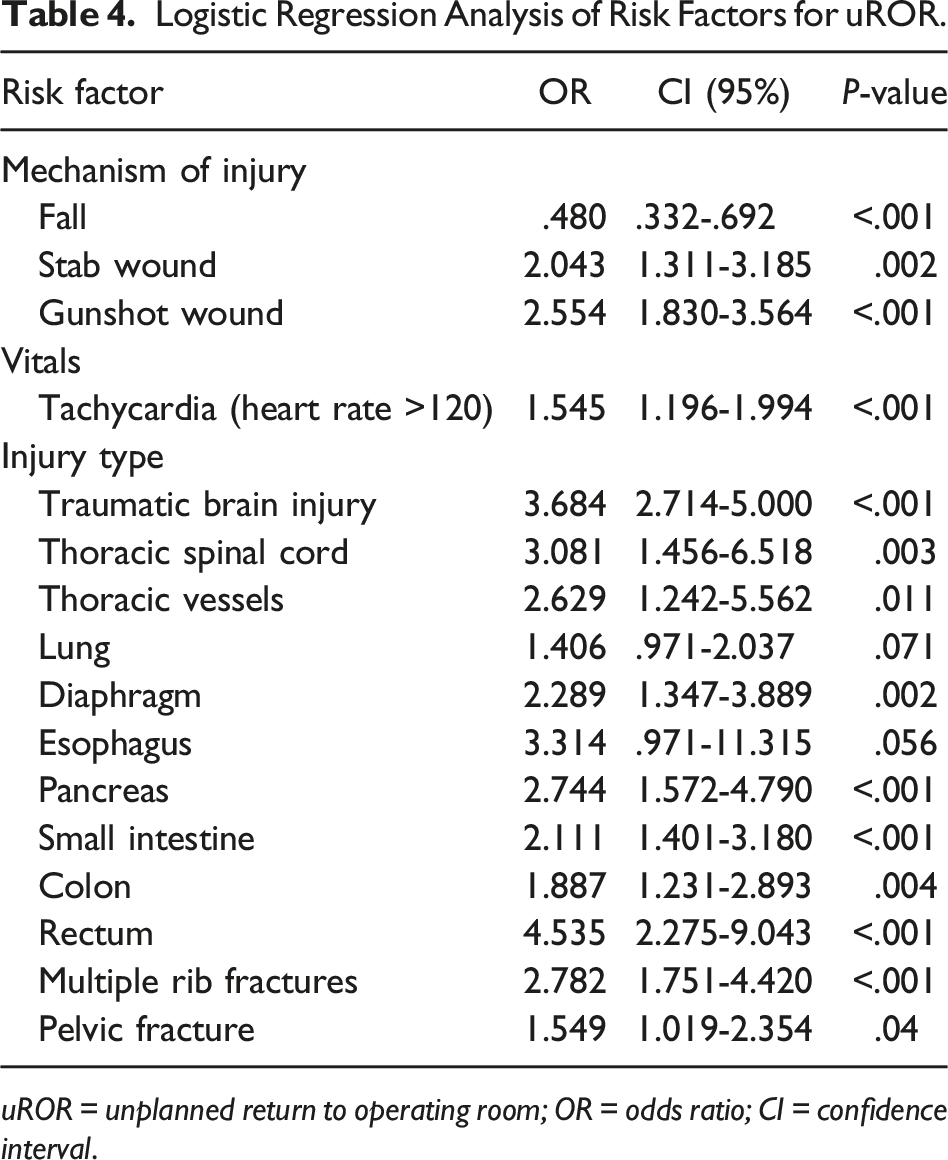
uROR = unplanned return to operating room; OR = odds ratio; CI = confidence interval.
Discussion
Unplanned reoperations are costly and predispose adult trauma patients to increased LOS and mortality.3,6 Similarly, this national analysis found increased complications, mortality, and LOS in PTPs undergoing uROR. In addition, associated risk factors for uROR included gunshot or stab wounds and specific injuries such as rectal injuries and TBI.
Injury can decrease physiologic reserve, alter homeostasis, and increase the risk of uROR. In this analysis of 3 years of national data, we found that nearly all injuries were more common in the uROR cohort. However, interestingly injury to the rectum was the strongest independent predictor for uROR. Challenges associated with rectal injuries that may predispose patients to uROR include the rarity of this injury, intra-abdominal contamination, and risk of post-surgical anastomotic leak, hemorrhage, and infection.7,8 While advancements have been made in terms of surgical tact, such as fecal diversion for extraperitoneal rectal injuries and primary anastomosis with judicious use of antibiotics, the anastomotic leak rate for elective rectal surgery (2.5% to 33.3%) is higher than other parts of the gastrointestinal tract.9–12 This, coupled with the relative infrequency of this injury, an incidence of .2% reported at a single center, likely contributes to the increased risk of uROR. 13 Additionally, rectal injuries in older PTPs are associated with more severe injuries and complications than younger PTPs. 14 Future efforts to increase education, standardize management strategies, and implement quality improvement efforts focused on pediatric rectal injuries should be employed to mitigate the risk of uROR.
Traumatic brain injury is a common injury for PTPs, but nonoperative management is used in most cases, as surgery is reserved for TBI with intracranial hemorrhage that causes significant mass effect. 15 Traumatic brain injury was the second greatest independent predictor of uROR in PTPs, even when controlling for extracranial injuries, which occur in 46-63% of severe TBI patients.16,17 This may at least partially be due to the fact that young children with TBI may be unable to communicate symptoms, thereby delaying treatment and leading to an increased risk of requiring uROR. Also, in general, TBI patients are known to have increased risk of complications that may or may not be directly related to a neurosurgical procedure, such as VAP and VTE.18,19 While these complications are rarer in children, it appears efforts to curtail uROR may be best targeted for children with brain injury.
Penetrating trauma is associated with direct trauma that is usually evident to the trauma surgeon. Of the mechanisms of injury analyzed, gunshot and stab wounds were both identified as independent associated risk factors for uROR in PTPs. Firearm injuries in the pediatric population continue to be a significant cause of morbidity and mortality. 20 In 2020, firearm injuries overtook MVC as the leading cause of death in people under 18 years of age. 1 This study suggests that, in addition to the loss of life suffered from penetrating trauma in children, there is also an increased risk of uROR that the practicing trauma surgeon should be aware of. Future research is needed to identify why this increased risk occurs and then attempt to mitigate the risk.
Limitations of this analysis include those inherent to a retrospective database design including missing data and coding errors. Given that the management of severely injured PTPs may involve damage control laparotomy prior to definitive surgical treatment, miscoding errors may lead to overestimates of uROR. 2 However, TQIP data collection is performed by trained data abstracters who are aware of this practice. This database lacks pertinent variables such as indications for uROR, if patients required more than 1 uROR, and the temporal relation of the uROR and index operation. Finally, there are notable differences between the cohorts in terms of ISS and morbidity, some of these were accounted for in the multivariable analysis; however, there may be unaccounted confounders not included.
In conclusion, PTPs suffering an uROR were more likely to have associated complications, LOS, and mortality. This study also identified multiple associated risk factors for pediatric uROR, including rectal injuries, TBI, and penetrating mechanisms of injury (ie, gunshot wounds and stab wounds). These risk factors deserve further study with the hope of mitigating the increased risk of uROR and poor outcomes seen in these children.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.