
Abstract
Background
Laboratory biomarkers have been used as prognostic markers in several solid tumors. This study aims to evaluate 3 preoperatively measured laboratory values: blood neutrophil to lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and monocyte-to-lymphocyte ratio (MLR), as potential prognostic biomarkers in patients with peritoneal carcinomatosis undergoing cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (CRS-HIPEC).
Methods
We performed a retrospective review of 156 patients who underwent CRS-HIPEC between 2013 and 2020. Biomarker ratios were calculated based on the preoperative laboratory values closest to the date of CRS-HIPEC. Multivariable Cox regression models were used to evaluate the biomarkers’ associations with survival (OS), recurrence-free survival (RFS), and postoperative outcomes.
Results
Increased MLR was independently associated with worse OS (P < 0.001) and RFS (P = 0.03) in this patient cohort. Additionally, increased MLR was independently associated with increased rate of hospital re-admission within 30 days after discharge (P = 0.04). None of the analyzed biomarkers were associated with increased rate of Clavien-Dindo class III/IV complication or hospital length of stay.
Conclusions
In this retrospective review, increased preoperative MLR was independently associated with worse overall and recurrence-free survival as well as increased rate of hospital re-admission. Preoperative PLR was associated with increased hospital length of stay. Thus, the utilization of preoperative systemic inflammatory biomarkers may aid in preoperative counseling and risk stratification prior to CRS-HIPEC.
Keywords
Key Takeaways
• This study used routine preoperative laboratory measurements to identify biomarkers associated with postoperative and oncologic outcomes for patients undergoing cytoreductive surgery with hyperthermic intraperitoneal chemotherapy. • In this patient population, increased preoperative monocyte-to-lymphocyte ratio was associated with worse overall survival and recurrence-free survival, while increased platelet-to-lymphocyte ratio was associated with increased hospital length of stay.
Introduction
Peritoneal carcinomatosis (PC) is regarded as end-stage cancer with poor survival due to limited effective treatment options. For select patients with PC due to appendiceal or colorectal origin, cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (CRS-HIPEC) has emerged as a potential surgical treatment option.1-3 Although such therapy, with or without systemic chemotherapy, has improved outcomes for select patients, CRS-HIPEC is associated with significant morbidity, with 25%-35% of patients sustaining a Clavien-Dindo grade III/IV complication.4,5 Additionally, recurrence rates remain high. Several studies have identified the peritoneal cancer index as well as a complete cytoreduction as important independent prognostic factors.6,7 However, few preoperative prognostic factors have been identified. Thus, much effort has recently been placed on patient selection and preoperative prognostication to identify patients who are most likely to benefit from CRS-HIPEC without sustaining postoperative complications.
Chronic inflammation is a predisposing risk factor for many cancers, including GI malignancies, and plays a pro-tumorigenic role in the development and proliferation of cancer. A pro-inflammatory state promotes tumor cell growth, potentially leading to impaired survival and enhanced recurrence patterns.8,9 Several studies have investigated the ability of inflammatory biomarkers as surrogates of a patient’s inflammatory state to predict postoperative and oncologic outcomes in patients with solid tumors, including colorectal, hepatobiliary, and gastric cancers.10-13 Such biomarkers include the neutrophil to lymphocyte ratio (NLR), monocyte-to lymphocyte-ratio (MLR), and the platelet-to-lymphocyte ratio (PLR), which can be derived from a patient’s complete blood cell count with differentiation. A meta-analysis encompassing over 2000 patients with bladder cancer demonstrated that increased neutrophil to lymphocyte ratio (NLR) was associated with disease recurrence and progression in patients who underwent TURBT. 12 More specifically, a recent retrospective study demonstrated that increased levels of preoperative NLR, PLR, and MLR of patients with non-small cell lung cancer undergoing surgery associated with disease-free survival and overall survival, while NLR and PLR were associated with worse overall survival in patients with stage II or III gastric cancer.14,15 However, it is unknown whether such markers can be used as prognostic factors for patients with peritoneal carcinomatosis undergoing CRS-HIPEC. Thus, the aim of this study is to determine the association between a patient’s preoperative NLR, MLR, and PLR and oncologic outcomes.
Methods
Data Sources and Definitions
This institutional retrospective study was approved by Institutional Review Board of Vanderbilt University (IRB # 200 638) and utilizes a prospectively maintained database of all patients with PC who underwent CRS-HIPEC with curative intent from 2013-2020 at Vanderbilt University Medical Center (Nashville, TN). We utilized this database to collect patient demographic information, such as gender, age, race, BMI, American Society of Anesthesiologists (ASA) class, as well at treatment information. Oncologic data, such as tumor origin and grade were based on final pathology report from the surgical specimen at the time of CRS-HIPEC. Additionally, the peritoneal surface disease severity score (PSDSS), peritoneal carcinomatosis index (PCI), and complete cytoreduction score (CCR) were obtained from the surgeon’s CRS-HIPEC operative note.
Laboratory biomarkers were calculated based on the patient’s most recent laboratory testing prior to CRS-HIPEC. NLR, PLR, and MLR were calculated by dividing the absolute neutrophil, platelet, or monocyte count by the absolute lymphocyte count, respectively. The primary outcomes of this study were the following: overall survival (OS), defined as time (months) from diagnosis of peritoneal carcinomatosis to death and recurrence-free survival (RFS), defined as time (months) from CRS-HIPEC to recurrence. The secondary outcomes were rate of Clavien-Dindo grade III/IV complication, postoperative hospital length of stay, and hospital re-admission within 30 days after discharge.
Statistical Analysis
The R package “XGBoost,” a machine-learning algorithm, was used to prioritize predictors for each outcome and perform internal validation for all fitted models. This supervised learning method prevents model overfitting seen in traditional modeling packages. Additionally, this algorithm includes variable ranking, thus providing a more precise predictive model. Prediction accuracy was measured by RMSE for continuous outcomes, AUC for binary outcomes, and C-index for time-to-event outcomes. For survival outcomes, the number of risk groups was determined using the K-means method. The feature importance cutoff value was set at SHAP>0.1 for both the primary and secondary survival outcomes. To better understand and estimate the impact of each predictor variable on patient survival, we further fitted Cox regression models to the survival outcomes (OS and RFS). To avoid model overfitting, we used the backward selection approach (R package “fastbw”) to reduce the full models. All statistical analyses were performed using R version 3.4.2.
Results
Patient Characteristics
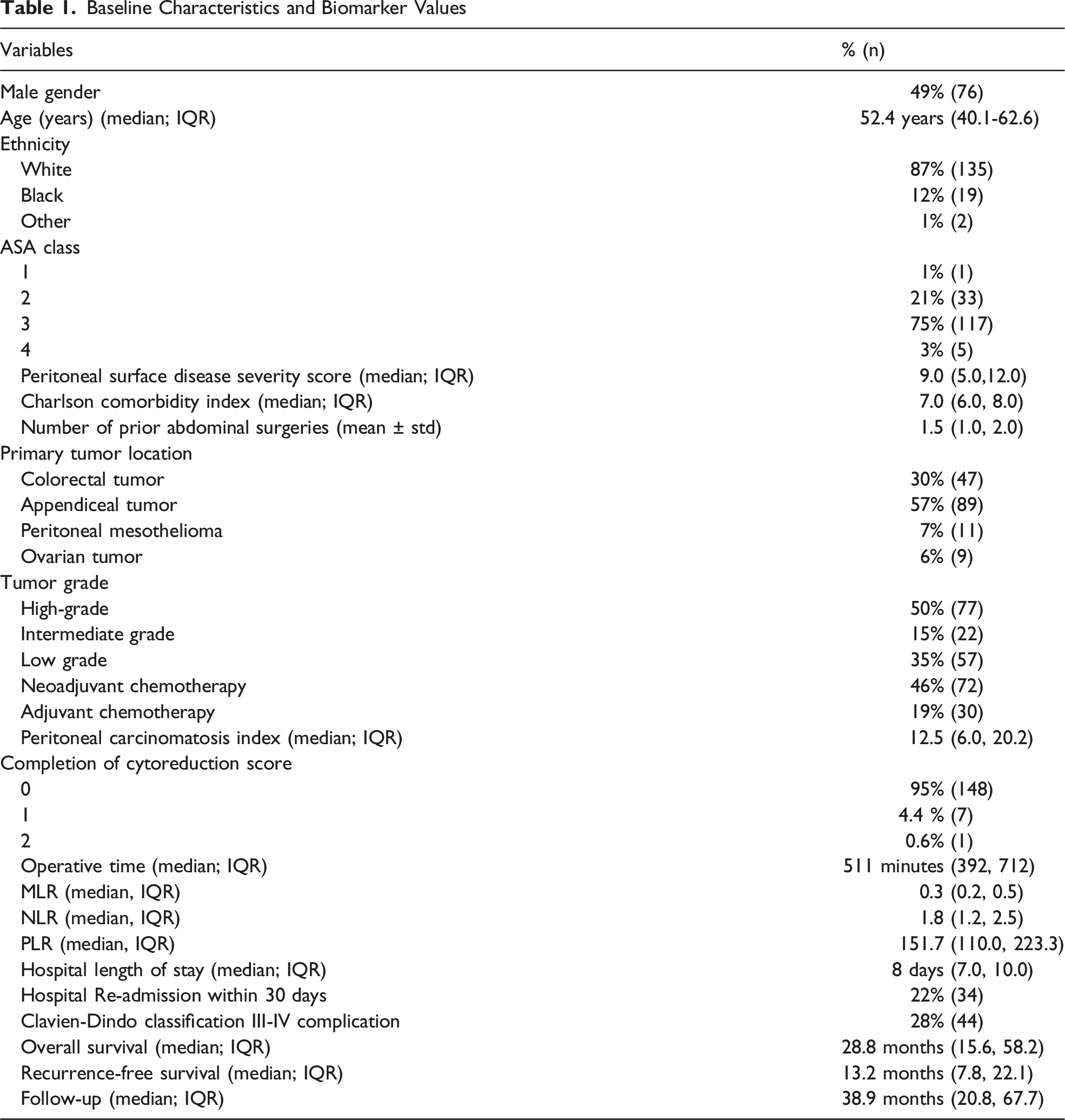
Baseline Characteristics and Biomarker Values
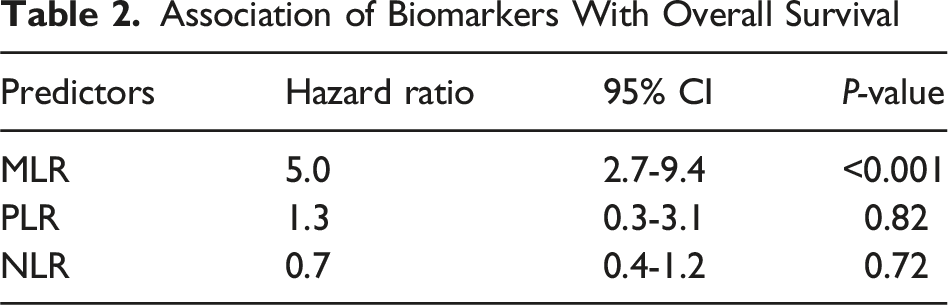
Association of Biomarkers With Overall Survival
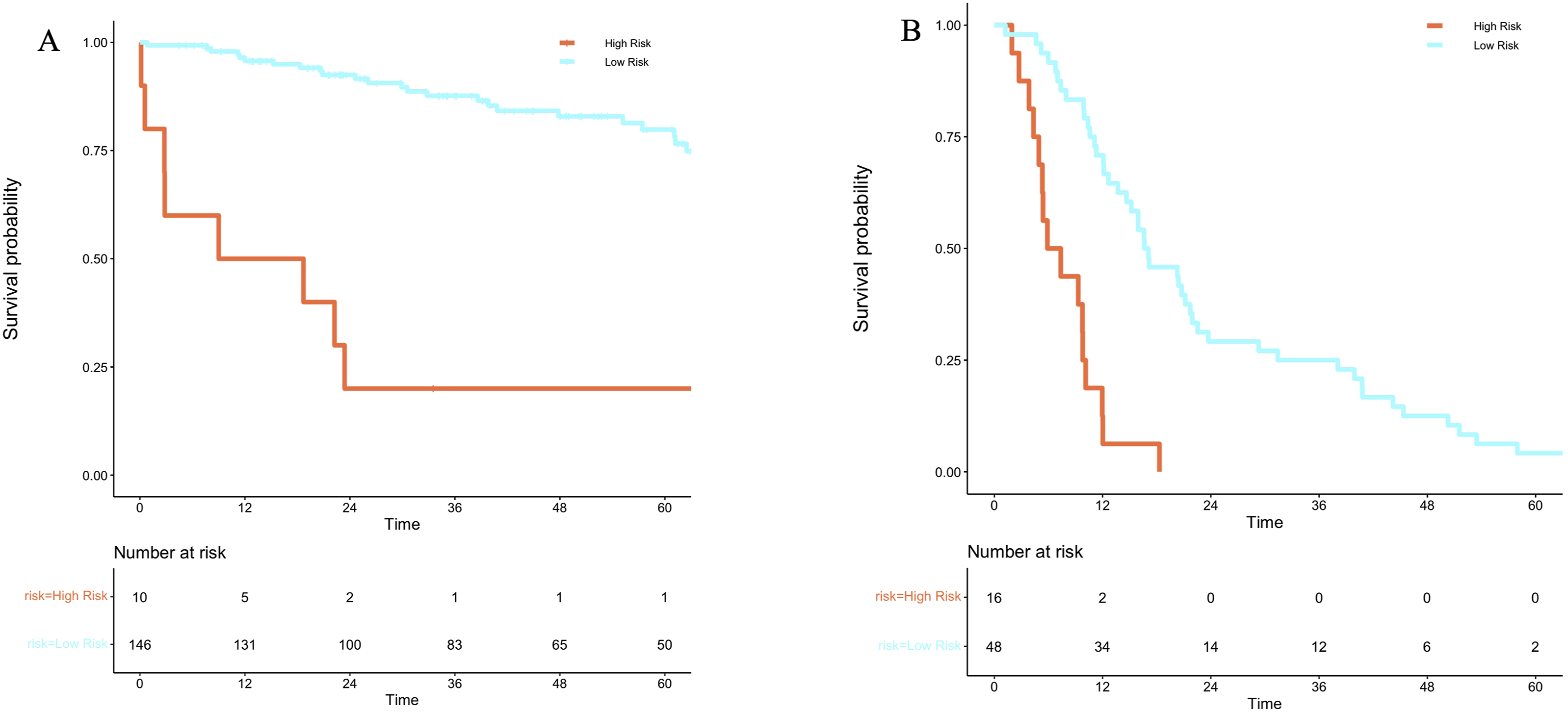
Using machine-learning method with XGboost model, the top predictors of worse overall survival with SHAP >0.1 were as follows: tumor grade, operative time, and MLR (Figure 1A). Using the same model, high and low-risk groups were identified based on differences in overall survival (Figure 2A). Median OS was 15.6 months in the high-risk group compared to 40 months in the low-risk group. Patients in the high-risk group are more likely to be male, have a higher PSDSS (12 vs 9; P = 0.002), high-grade disease (80% vs 34% P = 0.02), higher PCI score (15.5 vs 12.0; P = 0.04), and have a median MLR, PLR, and NLR of 0.7, 275.9, and 3.0, respectively compared to 0.3, 149.2, and 1.8, in the low-risk group (P = 0.01, 0.02, 0.04; Supplement Table 1). Cox regression analysis demonstrated that increased MLR was the sole evaluated biomarker independently associated with worse overall survival (HR 5.0, 95% CI 2.7-9.4; P < 0.001; Table 2). Predictors of Worse (A) Overall Survival and (B) Disease-Free Survival (A) Overall and (B) Disease-Free Survival Based on Risk Stratification Association of Biomarkers With Overall Survival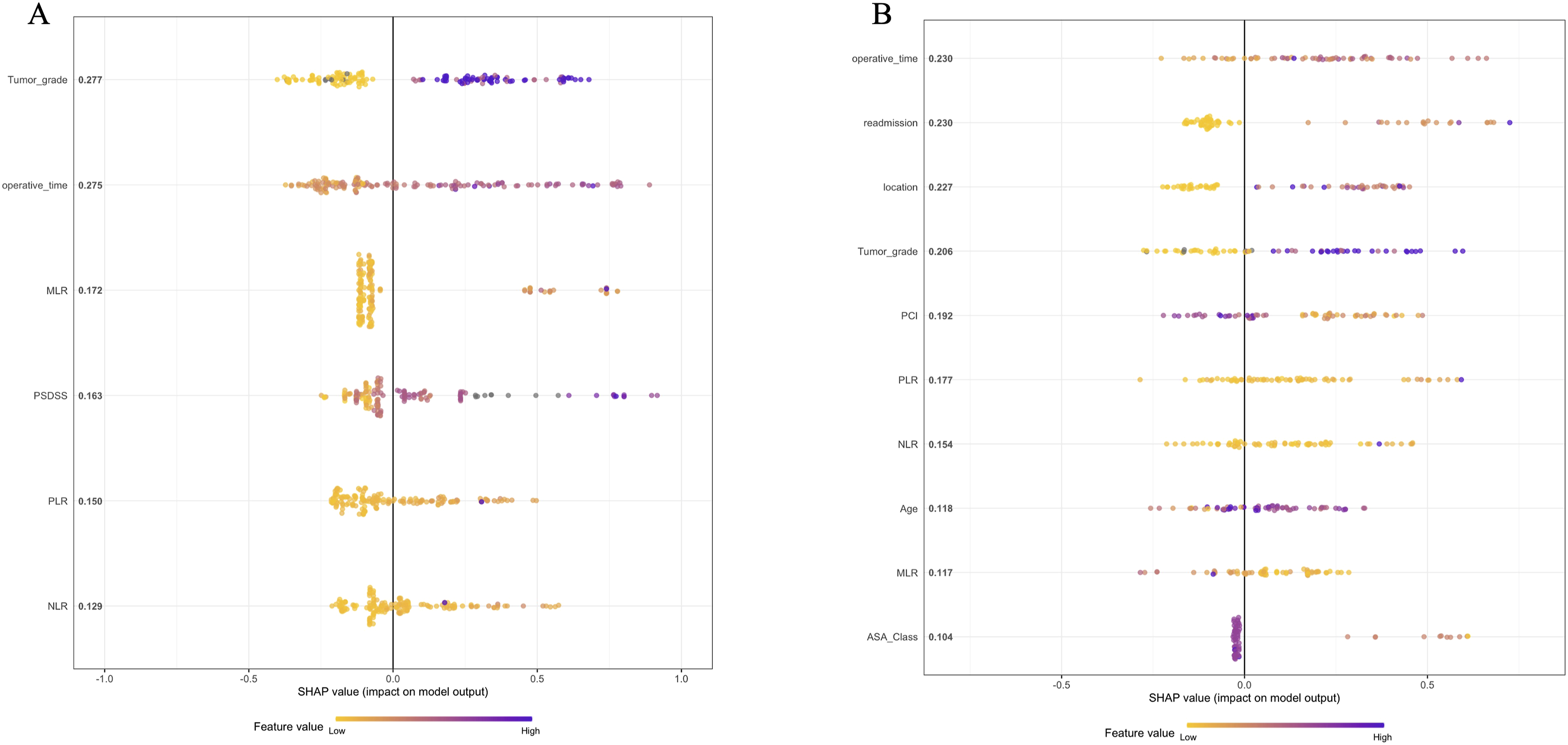
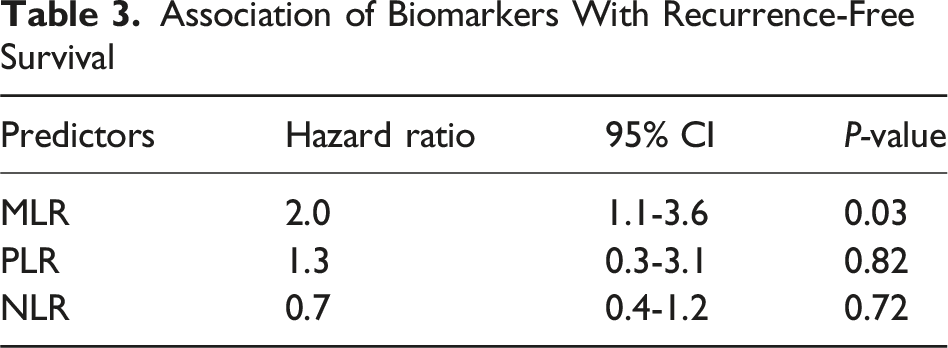
Association of Biomarkers With Recurrence-Free Survival
Association of Biomarkers With Recurrence-Free Survival
Association of Biomarkers With Postoperative Outcomes
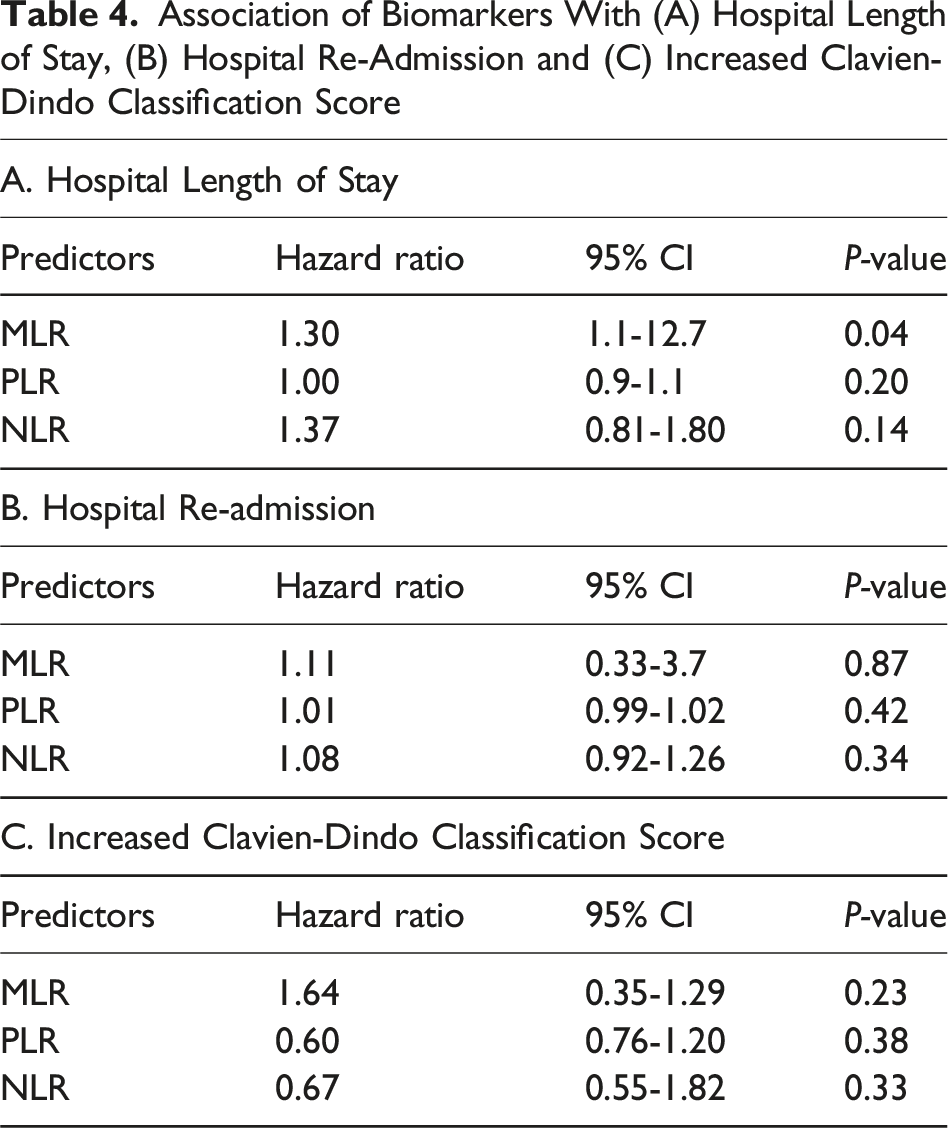
Using the same model as above, the top predictors of Clavien-Dindo grade III/IV complication were NLR, age, PCI, and MLR (Figure 3). However, none of the biomarkers were associated with increased rate of Clavien-Dindo III/IV complication or hospital length of stay. Increased MLR was associated with increased rate of hospital re-admission within 30 days after discharge (HR 1.3, 95% CI 1.1-1 P = 0.04; Table 4). Predictors of Clavien-Dindo Grade III/IV Complication Association of Biomarkers With (A) Hospital Length of Stay, (B) Hospital Re-Admission and (C) Increased Clavien-Dindo Classification Score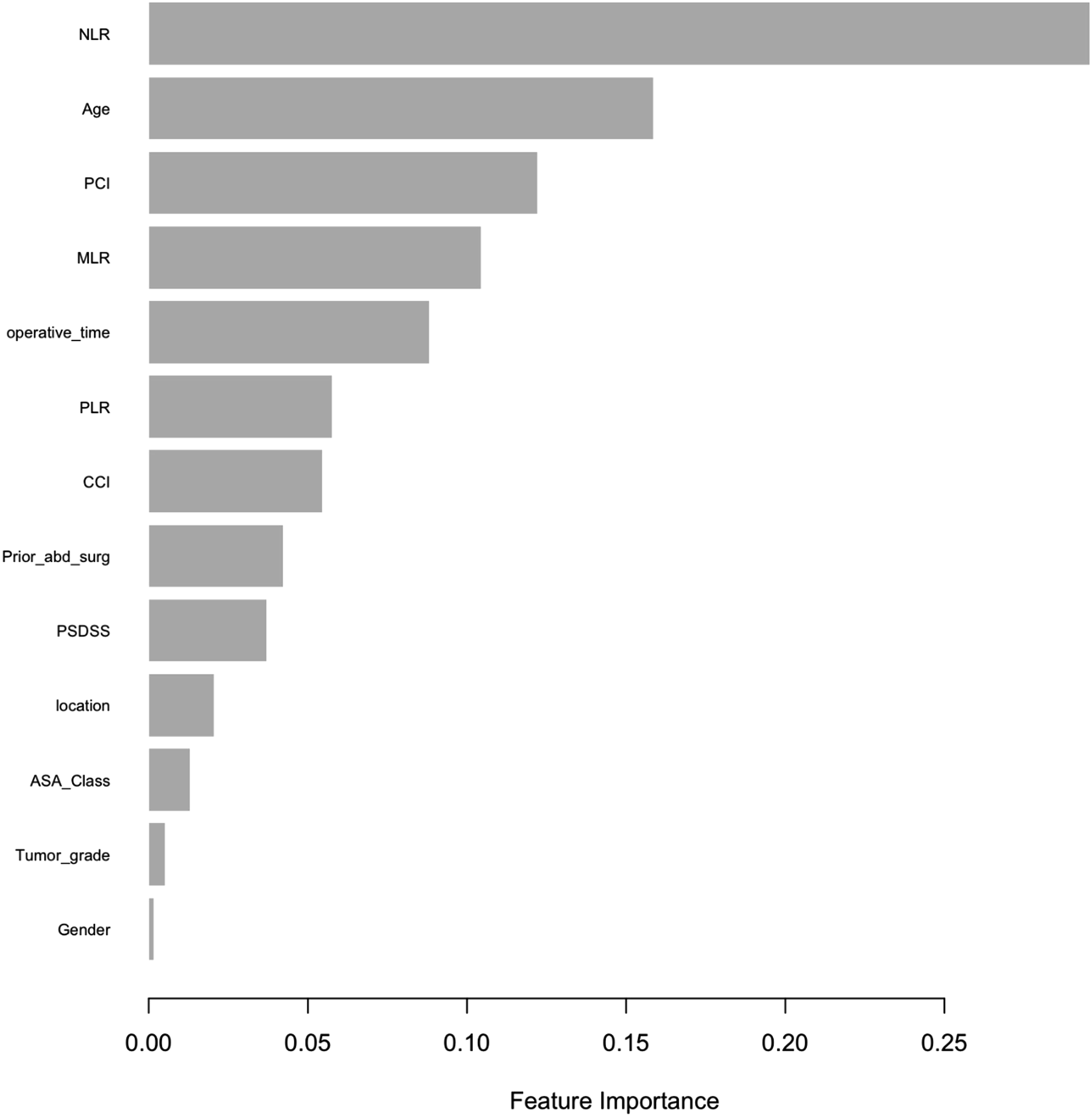
Discussion
In this retrospective study of 156 consecutive patients who underwent CRS-HIPEC with curative intent, increased preoperative MLR, was associated with shortened overall and disease-free survival as well as rate of hospital re-admission. To date, this is the largest study investigating the predictive and prognostic role that serological inflammatory biomarkers may have in patients undergoing CRS-HIPEC, which have been corroborated in similar investigations. Recent similar analyses demonstrated that increased MLR was associated with worse OS and DFS in patients with early-stage lung cancer who underwent lobectomy as well as patients with gastric cancer undergoing neoadjuvant chemotherapy.10,16 However, such studies among others did not simultaneously investigate the association with postoperative outcomes. While some studies have demonstrated that increased serologic biomarkers, including NLR, are associated with worse postoperative outcomes, such studies used postoperative or real-time laboratory measures as diagnostic rather than predictive markers.17,18
Furthermore, several studies have used varying laboratory value thresholds to compare patient outcomes, which may not provide significant clinical relevance when counseling patients preoperatively. A similar recent study examined 94 patients with colorectal peritoneal metastases who underwent CRS-HIPEC fond that increased NLR and positive lymph nodes were independently associated with worse overall and disease-free survival in a multivariate analysis. 19 However, this study specifically compared patients with biomarker values in the top quartile to the rest of their patient cohort to determine its association with survival. The top quartile of patients in this patient cohort had a significantly higher NLR compared to the patients in our current study (3.57 vs 2.5). Additionally, the average PCI in our patient cohort is twice as high as the PCI in the aforementioned study (13 vs 6), thus indicating baseline and oncologic differences in these patient cohorts. These data may be more reflective of patients with more severe disease at the time of CRS-HIPEC. Nonetheless, our findings are supported by recent data, specifically that increased NLR is associated with worse OS and DFS in patients with appendiceal peritoneal metastases undergoing CRS-HIPEC. 20
The molecular and immunologic mechanism by which peritoneal metastasis occur is still not well understood, but it is believed that the distinct immune cell populations within the highly complex peritoneal ecosystem provide a suitable environment for tumor cells to proliferate.21,22 This study identifies specific immune cells that are elevated in patient serum, which may be reflective of the peritoneum. Monocytes and monocyte-derived dendritic cells have been identified within the peritoneal cavity in patients with gastric peritoneal carcinomatosis to lead to reduced antigen-presenting capacity and increased pro-angiogenic capacity, which contributes to the immune-evasion mechanism of these tumors.22-24 Similarly, neutrophils have been shown to be recruited by colon tumor cells, which in turn stimulate several signaling pathways to promote tumor progression and metastasis. 23 Ongoing and future translational studies are needed to elucidate the mechanism by which these identified immune cells promote peritoneal metastasis. Our findings provide preoperative prognostic markers that provide clinically valuable information to assist in optimized patient-centered decision-making.
The limitations of this study include its retrospective design, heterogenous patient population, and analysis of patients from a single institution. Further studies are needed to identify how these preoperative inflammatory biomarkers can be combined with known patient factors, such as tumor origin and grade, tumor markers, and other laboratory values. Nonetheless, the findings of this study support the idea that preoperative serologic biomarkers have clinical utility in predictive oncologic and postoperative outcomes in patients with PC undergoing CRS-HIPEC. Elevated preoperative inflammatory biomarkers may not necessarily be used to prohibit patients from undergoing CRS-HIPEC. However, these could be utilized by providers as they counsel patients on potential oncologic outcomes and postoperative complications, particularly for frail patients, those with medical comorbidities who may not be ideal surgical candidates or patients who are unsure about proceeding with surgery. Such values provide context for the underlying disease biology beyond what is radiologically resectable. Future prospective studies are warranted in this patient population and clinical context for further validation and specification.
Conclusion
In this institutional retrospective study of 156 patients with peritoneal carcinomatosis undergoing CRS-HIPEC, preoperatively increased MLR was independently associated with worse overall and disease-free survival as well as increased rate of hospital re-admission. Such findings require further prospective validation and can potentially be used to optimize preoperative patient counseling in the setting of patient-centered decision-making.
Supplemental Material
Supplemental Material - Prognostic Value of Systemic Inflammatory Biomarkers in Patients Undergoing Cytoreductive Surgery With Hyperthermic Intraperitoneal Chemotherapy
Supplemental Material for Prognostic Value of Systemic Inflammatory Biomarkers in Patients Undergoing Cytoreductive Surgery With Hyperthermic Intraperitoneal Chemotherapy by David N. Hanna, Muhammad O. Ghani, Alexander Mina, Andrew Hermina, Kun Bai, Fei Ye, Christina E. Bailey, Kamran Idrees, and Deepa Magge in The American Surgeon™.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health – National Cancer Institute T32CA106183.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.