
Abstract
Introduction
Blunt trauma patients (BTPs) with cirrhosis are at an elevated risk for hemorrhagic complications, including traumatic brain injury (TBI). This study assessed whether BTPs with cirrhosis experience higher rates of TBI and severe TBI compared to those without cirrhosis and whether alcohol use disorder (AUD) further impacts these outcomes.
Methods
We analyzed data from the 2017-2022 Trauma Quality Improvement Program (TQIP) for BTPs aged ≥18 years
Results
Among 4 182 335 BTPs, 53 190 (1.3%) had cirrhosis. Cirrhotic patients had higher rates of TBI (26.3% vs 17.8%, P < .001), severe TBI (7.2% vs 3.2%, P < .001), complications (11.9% vs 4.6%, P < .001), longer hospital stay (6 vs 4 days, P < .001), and mortality (9.7% vs 2.9%, P < .001) compared to non-cirrhotics. After adjusting for age and injury severity, on multivariable analysis, cirrhotic patients were independently associated with an increased risk of severe TBI (OR 2.02, 95% CI 1.88-2.17, P < .001). Among cirrhotics, those with AUD had higher rates of TBI (31.4% vs 23.1%, P < .001), severe TBI (10.6% vs 5.3%, P < .001), and increased adjusted mortality risk (OR 1.18, 95% CI 1.11-1.27, P < .001).
Conclusion
Cirrhosis is associated with a significantly increased risk of TBI and severe TBI among BTPs, AUD further amplifies these risks. Awareness of these associations is essential for risk stratification and management in trauma care.
Level of Evidence
IV.
Key Takeaway
• Blunt trauma patients with cirrhosis have a 2-fold increased risk of severe traumatic brain injury and a 3-fold increased risk of mortality. • Cirrhotic patients with a concomitant past medical history of Alcohol Use disorder had a higher rate of TBI and severe TBI compared to patients with cirrhosis without a diagnosis of AUD. • These findings highlight the need for heightened clinical vigilance and individualized management strategies, including potential modifications to existing trauma protocols, for blunt trauma patients with cirrhosis.
Introduction
The incidence of liver cirrhosis in the general population is approximately 1%. Although the percentage is low, one study revealed that roughly half of those individuals with cirrhosis will present to the emergency room. 1 This chronic disease is well-documented in previous literature to significantly increase morbidity and mortality in emergent trauma patients as well as those undergoing elective surgeries.2,3 These findings can be partially explained by the complex pathophysiology of cirrhosis, which includes coagulopathy characterized by thrombocytopenia, abnormal fibrinolysis, and reduced clotting factors, 4 as well as impaired cerebral autoregulation and fluid shifts. 5 These sequelae of cirrhosis further elevate the risk of hemorrhagic complications and adverse outcomes in trauma patients. In addition, prior research has identified cirrhosis as a risk factor for traumatic brain injury (TBI). 6 Notably, alcoholic liver disease (ALD) has been associated with a worse prognosis than nonalcoholic causes of cirrhosis such as hepatitis C virus or nonalcoholic fatty liver disease, with ALF identified as an independent risk factor for increased mortality. 7 These outcomes appear to be particularly pronounced in active alcohol consumers, highlighting the importance of assessing alcohol use as part of clinical risk stratification. 7
Cirrhosis, with its myriad of systemic effects, can increase the risk for a TBI due to impaired motor and cognitive senses leading to higher rates of injuries as well as the disruption of the liver’s function of natural anticoagulants causing propensity for hemorrhage.4,8 However, there is a paucity of data related to how cirrhosis affects the severity of TBI in a national cohort of blunt trauma patients (BTPs). We hypothesized that BTPs with cirrhosis will exhibit higher rates and associated risk of TBI and severe TBI when compared to patients without cirrhosis. Likewise, we predicted that patients with cirrhosis and concurrent alcohol use disorder (AUD) would increase the association with TBI compared to cirrhotic patients without AUD. This information may help with prognostication and improve provider vigilance when caring for this population.
Methods
This study was deemed exempt by our Institutional Review Board and a waiver of informed consent was granted due to use of a national de-identified database. This retrospective cohort study utilized the 2017-2022 Trauma Quality Improvement Program (TQIP) database, a nationally representative dataset capturing trauma cases from verified trauma centers across the United States. All BTPs ≥18 years old were included. Patients with a history of prior anticoagulant use were excluded to minimize the confounding effect of pharmacologic anticoagulation on TBI risk and outcomes (Fig. S1). The study population was divided into two groups based on the presence or absence of cirrhosis: BTPs with a pre-existing diagnosis of liver cirrhosis and BTPs without a diagnosis of liver cirrhosis. Within the cirrhosis group, patients were further stratified by the presence or absence of AUD.
The primary outcome was the incidence and associated risk of TBI, while the secondary outcome was mortality. TBI severity was categorized using the Abbreviated Injury Scale (AIS) grade as mild (AIS 1-2), moderate (AIS 3-4), and severe (AIS 5-6). Additional outcomes included in-hospital mortality, hospital length of stay (LOS), intensive care unit (ICU) LOS, ventilator days, unplanned return to the operating room, and overall in-hospital complications. Disposition decisions such as being sent to a skilled nursing facility (SNF) were obtained. We also collected patient demographic information including age, sex, and comorbidities. The mechanism of injury and the injury profile, including injury severity score (ISS) and injuries to the head, chest, abdomen, spine, and extremities. Data regarding type of TBI was collected, including epidural hematoma (EDH), subdural hematoma (SDH), and subarachnoid hemorrhage (SAH).
Statistical Analysis
Bivariate analyses comparing cirrhotic and non-cirrhotic patients were performed with Mann-Whitney-U test to compare continuous variables and chi-square to compare categorical variables. Continuous variables were reported as medians with interquartile range or means with standard deviations, and categorical variables were reported as percentages. To assess the relationship between cirrhosis and both TBI risk and severity, as well as in-hospital mortality, multivariable logistic regression models were constructed. Variables were selected based on author consensus and review of the literature.9,10 These included age, ISS, specific comorbid conditions, frailty, and vitals on arrival such as hypotension (SBP <90 mmHg), tachycardia (HR >120/min), and tachypnea (RR >22/min). The adjusted risk was then reported with an odds ratio (OR) and 95% confidence intervals (CI). All P-values were two-sided, with a statistical significance level of <.05. All analyses were performed with IBM SPSS Statistics for Windows (Version 29, IBM Corp., Armonk, NY).
Results
Demographics and Injury Profiles for BTPs With and Without Cirrhosis
Demographics and Comorbidities of Cirrhotic and Non-cirrhotic Patients
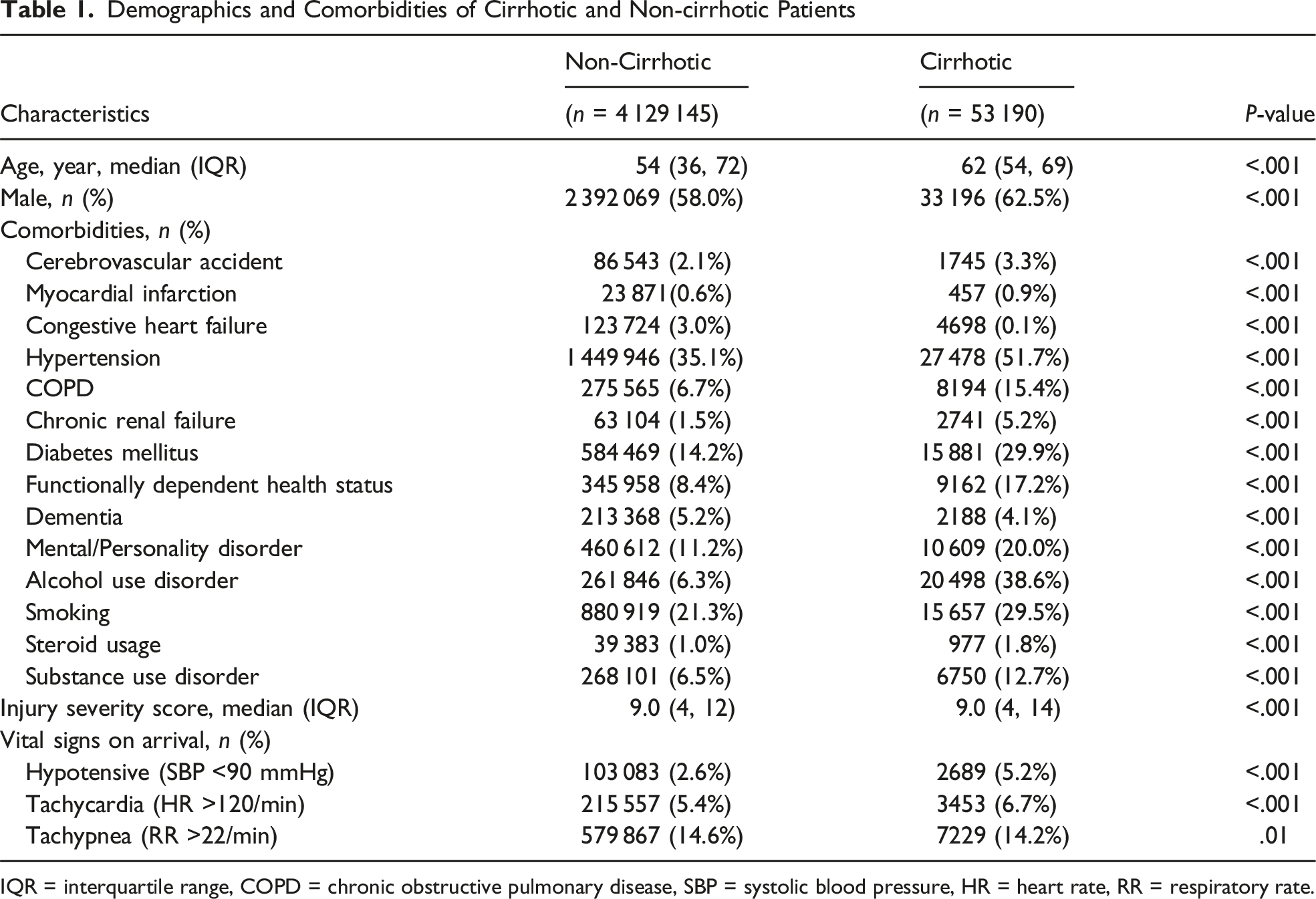
IQR = interquartile range, COPD = chronic obstructive pulmonary disease, SBP = systolic blood pressure, HR = heart rate, RR = respiratory rate.
Injury Profiles of Cirrhotic vs Non-cirrhotic Patients

AIS = abbreviated injury score.
Demographics and Injury Profiles for Cirrhotic Patients With and Without AUD
Demographics and Comorbidities of Cirrhotic Patients With vs Without AUD
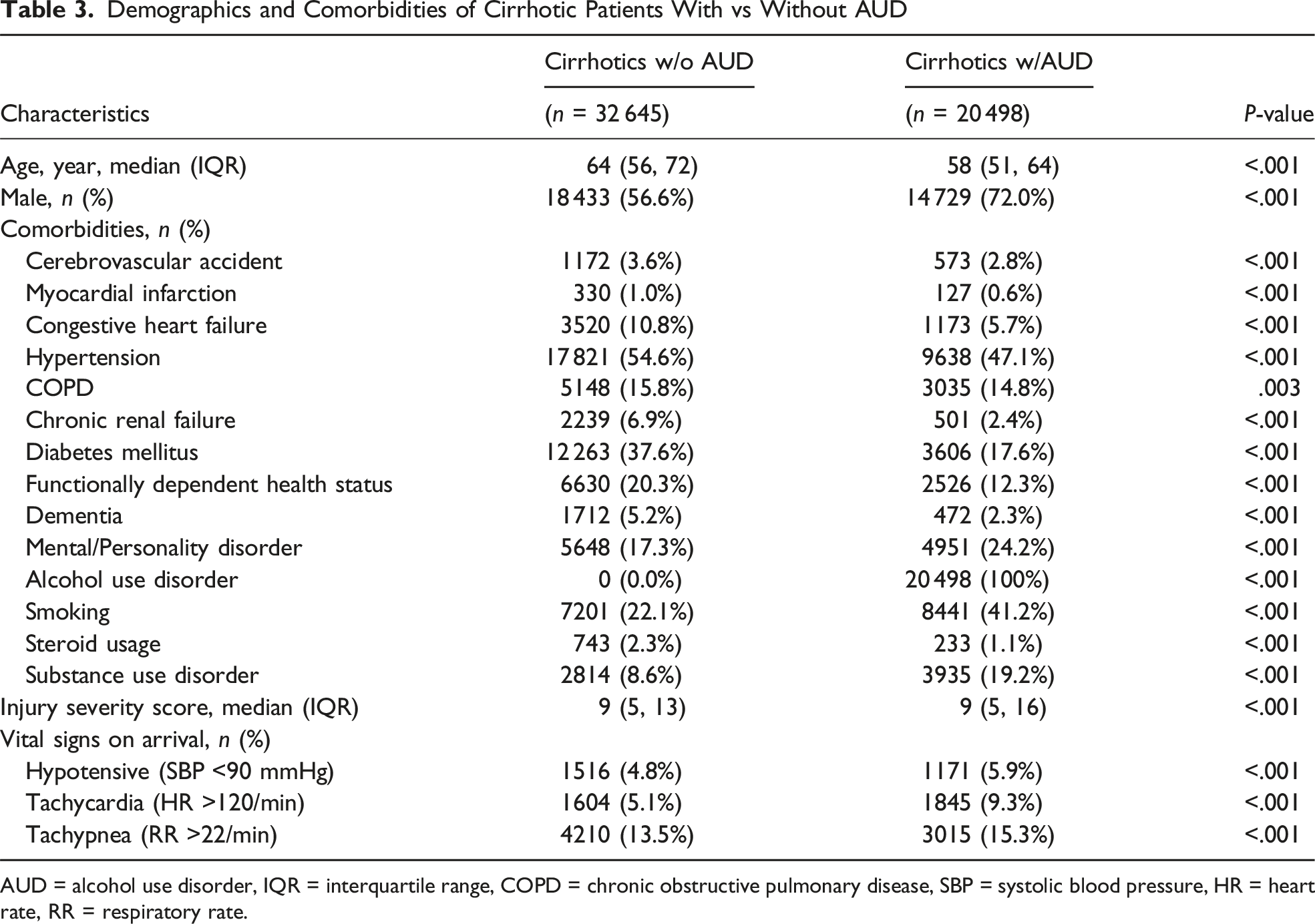
AUD = alcohol use disorder, IQR = interquartile range, COPD = chronic obstructive pulmonary disease, SBP = systolic blood pressure, HR = heart rate, RR = respiratory rate.
Incidence of TBI and Associated Risk of Severe TBI in BTPs With and Without Cirrhosis
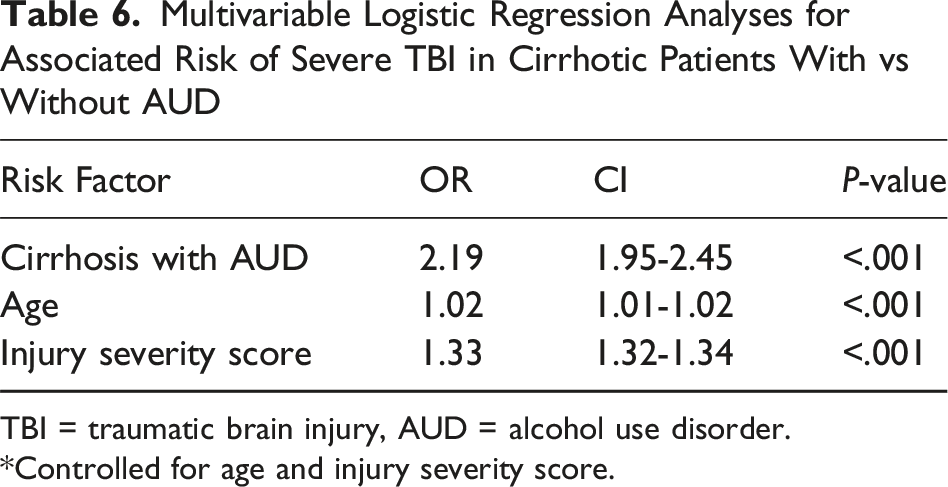
Multivariable Logistic Regression Analyses for Associated Risk of Severe TBI in Cirrhotic vs Non-Cirrhotic Patients
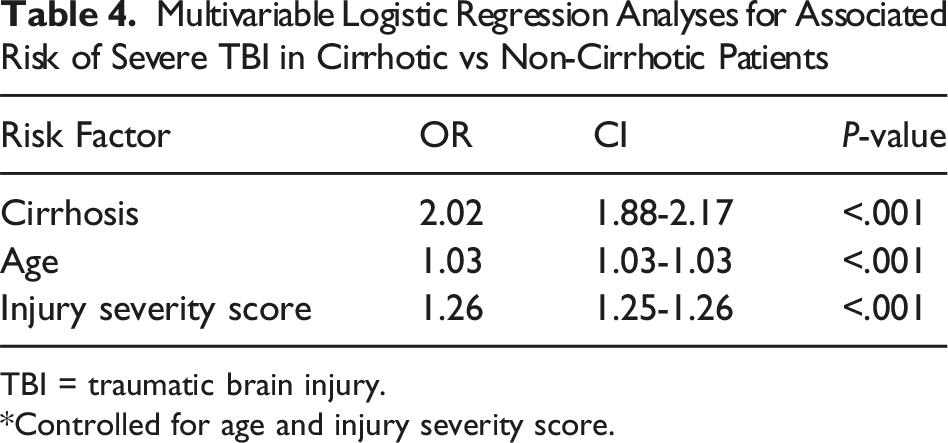
TBI = traumatic brain injury.
*Controlled for age and injury severity score.
Incidence of TBI and Associated Risk of Severe TBI in Cirrhotic Patients With and Without AUD
Injury Profiles of Cirrhotic Patients With vs Without AUD
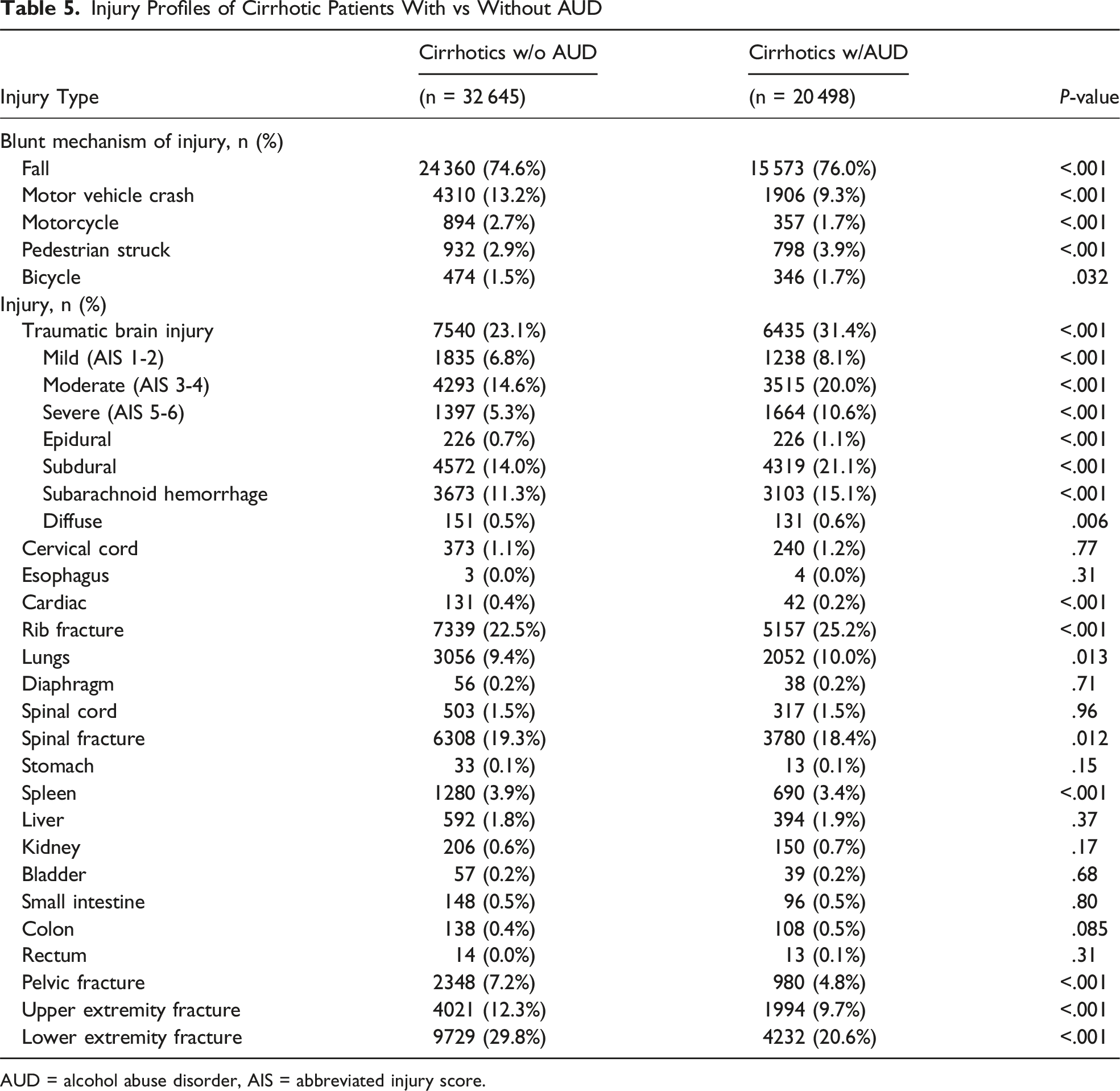
AUD = alcohol abuse disorder, AIS = abbreviated injury score.
Multivariable Logistic Regression Analyses for Associated Risk of Severe TBI in Cirrhotic Patients With vs Without AUD
TBI = traumatic brain injury, AUD = alcohol use disorder.
*Controlled for age and injury severity score.
Multivariable Logistic Regression Analyses for Associated Risk of Overall TBI in Cirrhotic Patients With vs Without AUD
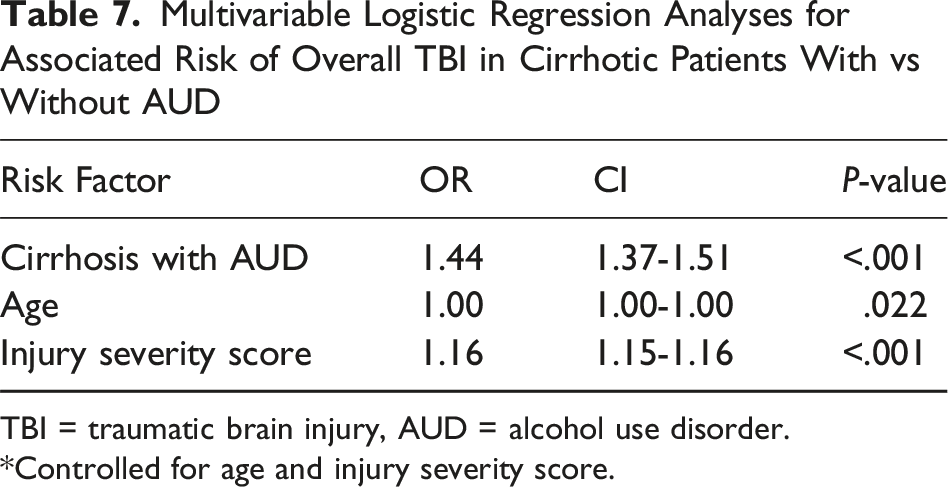
TBI = traumatic brain injury, AUD = alcohol use disorder.
*Controlled for age and injury severity score.
Hospital Outcomes and Complications for BTPs With and Without Cirrhosis
Clinical Outcomes and Complications Cirrhotic vs Non-cirrhotic Patients
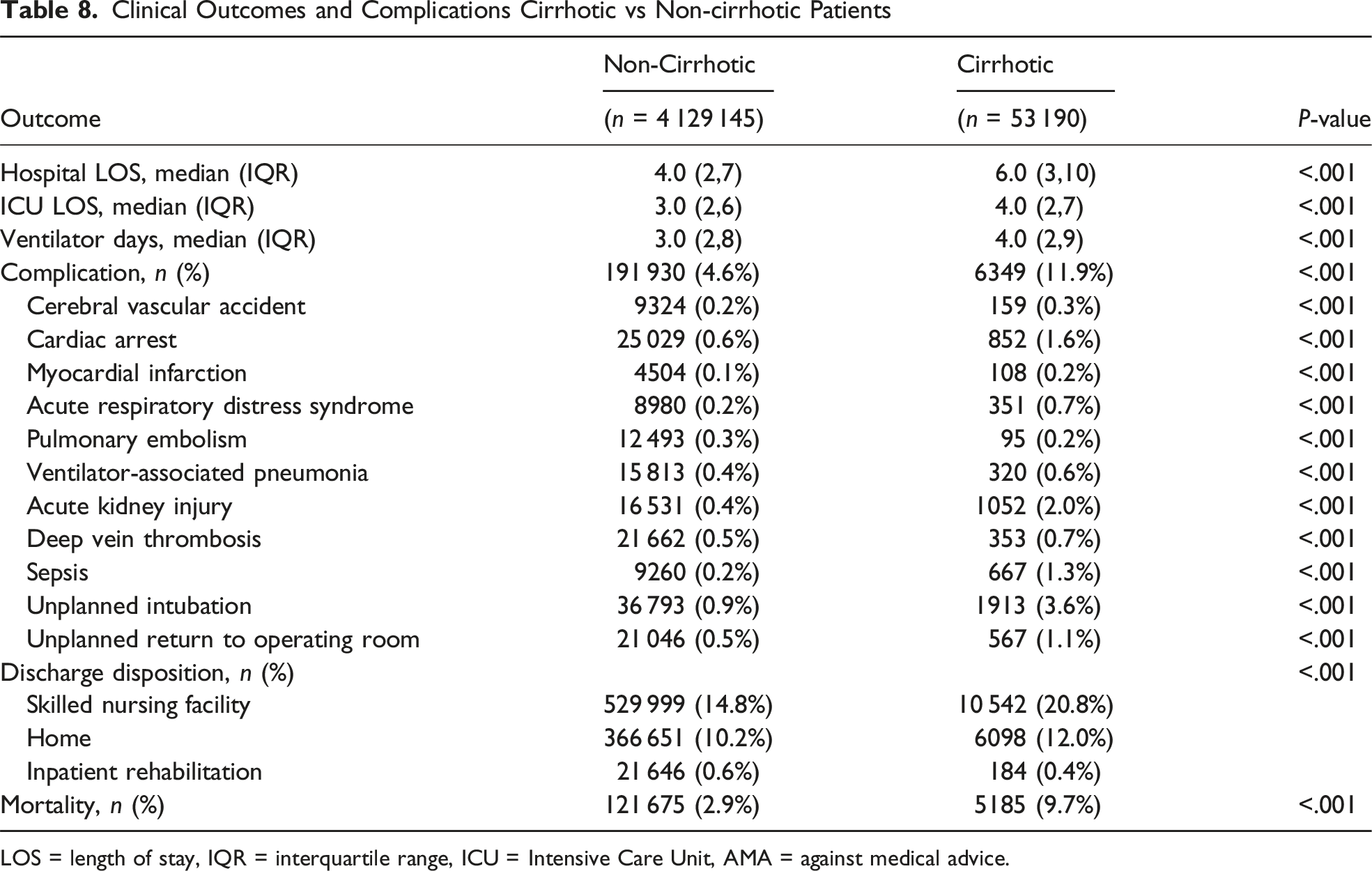
LOS = length of stay, IQR = interquartile range, ICU = Intensive Care Unit, AMA = against medical advice.
Hospital Outcomes and Complications for Cirrhotic Patients With and Without AUD
Clinical Outcomes and Complications of Cirrhotic Patients With vs Without AUD
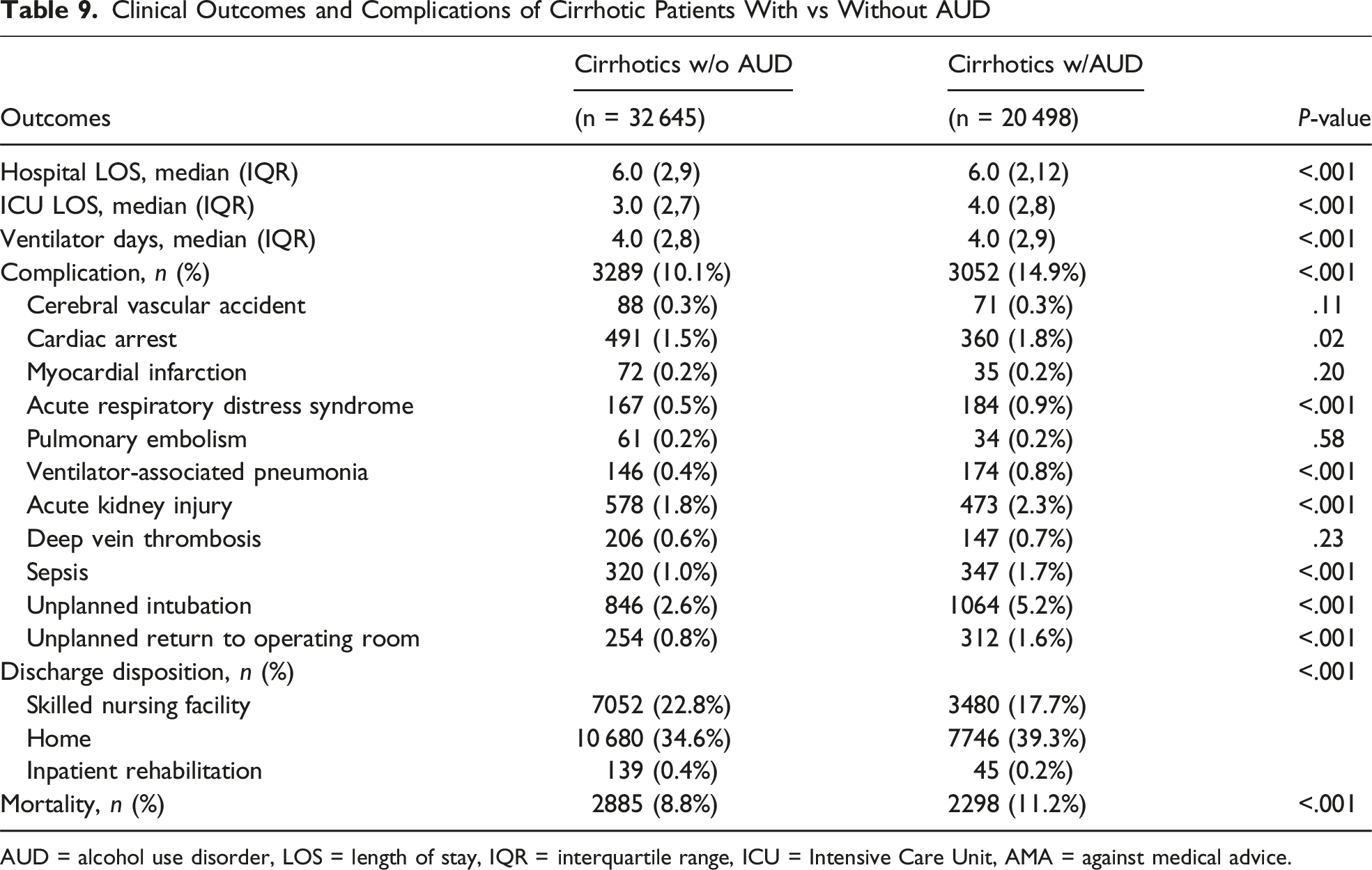
AUD = alcohol use disorder, LOS = length of stay, IQR = interquartile range, ICU = Intensive Care Unit, AMA = against medical advice.
Associated Risk of Mortality for BTPs With and Without Cirrhosis
Multivariable Logistic Regression Analyses for Associated Risk of Mortality in Cirrhotic vs Non-cirrhotic Patients
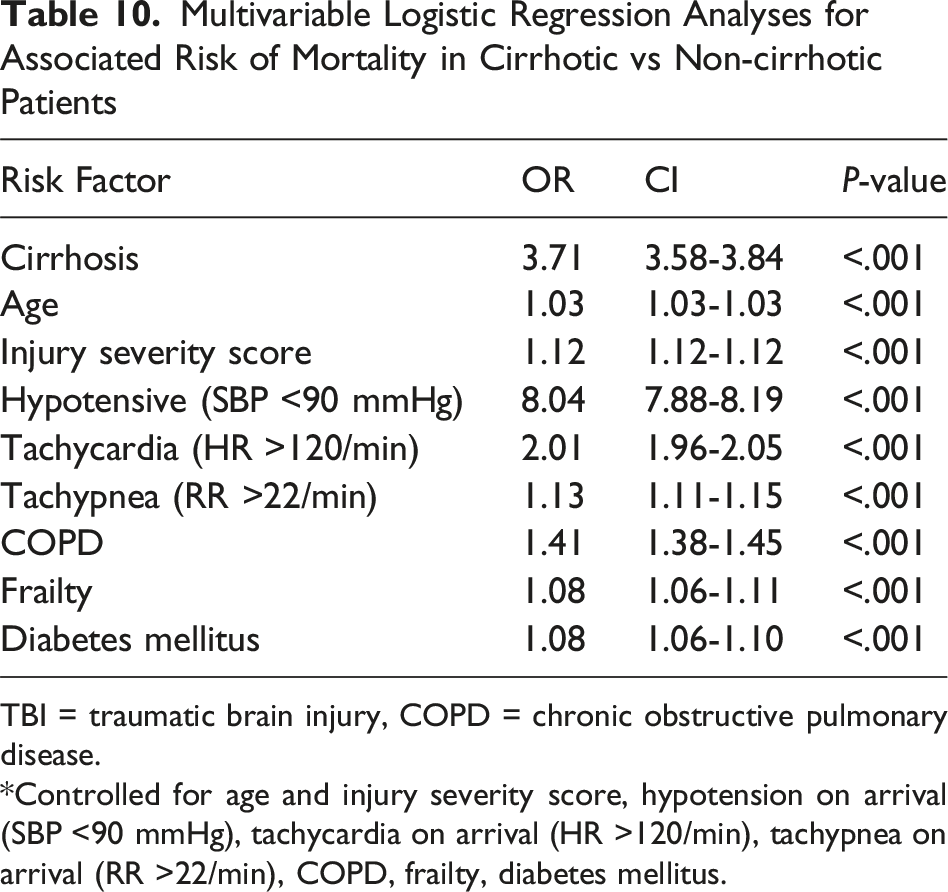
TBI = traumatic brain injury, COPD = chronic obstructive pulmonary disease.
*Controlled for age and injury severity score, hypotension on arrival (SBP <90 mmHg), tachycardia on arrival (HR >120/min), tachypnea on arrival (RR >22/min), COPD, frailty, diabetes mellitus.
Associated Risk of Mortality for Cirrhotic Patients With and Without AUD
Multivariable Logistic Regression Analyses for Associated Risk of Mortality in Cirrhotic Patients With vs Without AUD
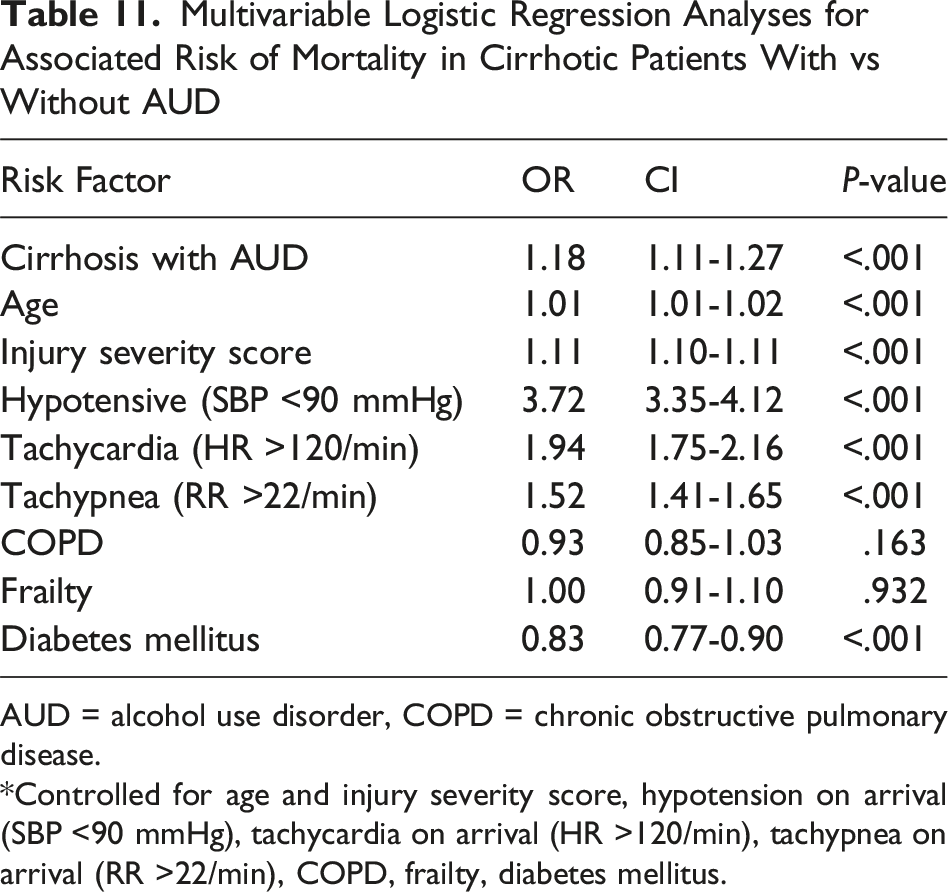
AUD = alcohol use disorder, COPD = chronic obstructive pulmonary disease.
*Controlled for age and injury severity score, hypotension on arrival (SBP <90 mmHg), tachycardia on arrival (HR >120/min), tachypnea on arrival (RR >22/min), COPD, frailty, diabetes mellitus.
Discussion
TBIs represent a significant public health concern. This study investigated the impact of liver cirrhosis on the incidence and severity of TBI in BTPs using a national trauma database and found that cirrhotic patients was associated with an increased rate of TBI and an over 2-fold independent increased risk of severe TBI compared to non-cirrhotic patients. Furthermore, the presence of cirrhosis was also associated with increased complications, LOS, and a mortality rate more than triple that of patients without cirrhosis. In addition, cirrhotics with AUD demonstrated higher rates of TBI across all severities and types, elevated complications rates, and an increased risk of severe TBI and in-hospital mortality compared to cirrhotics without AUD.
In this national analysis of BTPs, approximately 1% had cirrhosis, and we observed not only an increased incidence of TBI overall, but also a higher rate of severe TBI, which remained significant on multivariable analysis demonstrating a 2-fold increased associated risk. Likewise, we found that among cirrhotic patients, those with concomitant AUD had significantly higher rates of TBI overall and across all severities. Cirrhosis with AUD had a more than 2-fold increased risk of severe TBI in a separate multivariable model. These findings are in line with previous studies that similarly demonstrated a relationship between cirrhosis and increased brain injuries. 6 There can be several explanations why cirrhotic patients would have higher rates and risk of suffering a TBI. Advanced cirrhosis often leads to cerebral atrophy, which is characterized by decreased brain density in both grey and white matter as demonstrated by neuroimaging studies. 5 The loss of cerebral structure places stress on bridging veins due to the increased space between the brain and skull which increases the risk of ICH including SDHs as observed in our study and others. 11 In addition to these structural vulnerabilities, alcohol-related cirrhosis compounds the risk through cognitive and motor impairments. Ritz et al 12 demonstrated that over half of patients with long-term alcohol misuse exhibited executive dysfunction, and more than 40% showed signs of ataxia. These deficits were significantly associated with liver fibrosis and alcohol withdrawal symptoms and may contribute to risky behaviors including falls, poor medication adherence, and unsafe decision-making. 12 These findings are supported by our own results which showed increased rates of falls among cirrhotic patients with concomitant AUD compared to those without. Hepatic encephalopathy further contributes to TBI as it inducing neurocognitive impairment, including psychomotor speed, attention, and visuo-spatial abilities, thereby increasing the likelihood of falls and injuries. 13
The interplay of coagulopathy and cirrhosis is complex with variable presentations of hypercoagulable and hypercoagulable states. As the liver produces most clotting factors, cirrhosis-related coagulopathy often involves thrombocytopenia, reduced clotting factor production, and abnormal fibrinolysis, increasing the risk of both bleeding and clotting complications.4,14 Maegele et al indicated that nearly two-thirds of severe TBI patients exhibited coagulopathy upon admission. 15 This pre-existing coagulopathy in cirrhosis can exacerbate TBI by increasing the risk and severity of intracranial hemorrhage. 14 Furthermore, TBI itself can induce or worsen coagulopathy, 15 creating a dangerous cycle of bleeding and clotting dysfunction in cirrhotic patients. Thus, it may not be surprising to see an increased associated risk of severe TBI in the cirrhotic cohort. This information may help inform trauma providers to have increased vigilance when caring for cirrhotic trauma patients with TBI.
Cirrhosis is strongly associated with mortality in numerous populations.1,2,7,16-18 Cirrhotic patients in our study had a more than three times increased associated risk of mortality compared to that of non-cirrhotic patients. This alarming finding is consistent with multiple studies demonstrating substantially increased mortality risk in cirrhotic trauma patients.16-18 For instance, Georgiou et al found a 12% mortality rate in cirrhotic trauma patients compared to 6% in non-cirrhotic patients, while Christmas et al reported an even higher mortality rate of 33% in their cirrhotic cohort vs just 1% in the control group.16,18 This increased mortality can be partially explained by an increased rate of complications. Our analysis corroborates the increased rate of many complications including CVAs, cardiac arrest, ARDS, sepsis, unplanned intubation, and unplanned return to the operating room. A similar pattern was observed among cirrhotic patients with AUD, who demonstrated higher rates of sepsis, ARDS, cardiac arrest, unplanned intubation, and unplanned return to the operating room. However, on multivariable analysis, cirrhosis appeared to independently be an increased risk for mortality. Likewise, while we observed higher in-hospital mortality among cirrhotics with AUD compared to those without, the adjusted odds ratio in multivariable analysis was relatively small. Although this association reached statistical significance, likely due to the large sample size, the absolute difference may not be clinically meaningful.
Prior nontrauma research suggests that multidisciplinary care including hepatology expertise may help mitigate morbidity in cirrhotic patients. 19 Together this information can help providers prognosticate outcomes for patients and families, and should act as a call to action to increase primary prevention efforts and research into multidisciplinary trauma care for patients with cirrhosis to attempt to help this at-risk population. Standard trauma algorithms, such as the Brain Injury Guidelines, assist in directing imaging and disposition decisions based on injury severity but were not developed with high-risk populations like cirrhotic patients in mind. 20 Given our findings of increased TBI severity and complications in this group, cirrhotic patients may fall outside these protocols and require enhanced neurologic monitoring and tailored clinical decision-making. The degree of morbidity and mortality in the cirrhotic trauma patient cohort underscores the urgent need for enhanced vigilance and the development of individualized management strategies tailored to the specific needs for this patient group. Our findings emphasize the need for prompt management of head injuries in cirrhotic trauma patients. Heightened vigilance should include early identification of intracranial bleeds, enhanced neurologic assessments, evaluation of liver function tests and clotting markers, prompt consideration for surgical intervention, and potential for intracranial pressure monitoring. Early reversal of coagulopathy and a multidisciplinary team approach may help reduce TBI-related morbidity and mortality. Optimizing resource utilization through a combination of early intervention, multidisciplinary care, and preventative strategies is essential for improving outcomes and reducing the economic burden associated with TBI and complications associated with patients with cirrhosis.
This study has several limitations inherent to its retrospective database design including selection and reporting bias, and coding errors. Furthermore, the TQIP database only includes data from trauma centers and thus may not be generalizable to non-trauma centers. In addition to our TQIP database, it only collects index hospitalization data and lacks pertinent variables including ongoing physiological parameters, laboratory values, specific timing of interventions, and social determinants of health, which all affect outcomes. Also, our definition of “severe TBI” (AIS 5-6) does not incorporate key examination findings (eg, GCS), CT imaging findings, (eg, Rotterdam score), as well as neurosurgical operative interventions (eg, Decompressive craniotomy). Future prospective studies should incorporate these and other potential confounders such as the severity of cirrhosis (ie, Model for End-Stage Liver Disease (MELD) and/or Child-Pugh Score) and presence of encephalopathy. Although we included data on cirrhotic patients with AUD as a surrogate for alcoholic cirrhosis, the TQIP database does not capture the underlying etiology of cirrhosis potentially underestimating alcoholic cirrhosis in patients with mixed etiologies, or whether patients had a history of alcoholic cirrhosis but had since stopped drinking and no longer met criteria for AUD at the time of trauma. Despite these limitations, our study, leveraging the large, nationally representative sample of the TQIP database, provides valuable insights into the heightened rate of TBI and complications, as well as the increased associated risk of severe TBI cirrhotic trauma patients, which should help guide future research, prognostication, and clinical vigilance.
This national analysis demonstrates that cirrhosis is associated with an increased risk of severe TBI among BTPs, a finding further underscored by the over 3-fold increase in mortality and elevated complication rates observed in our cirrhotic cohort. Moreover, AUD was found to be associated with higher rates of TBI across all severities and types, increased risk of both overall and severe TBI. These findings highlight the urgent need for primary prevention, individualized management strategies, and a multidisciplinary approach to mitigate the increased morbidity and mortality in this vulnerable population. Further research into targeted interventions, including enhanced protocols and a multidisciplinary care model incorporating hepatology expertise, is warranted to optimize outcomes in cirrhotic BTPs.
Supplemental Material
Supplemental Material - Higher Rates of Traumatic Brain Injury in Blunt Trauma Patients With Cirrhosis: Worse Outcomes With Concomitant Alcohol Use Disorder
Supplemental Material for Higher Rates of Traumatic Brain Injury in Blunt Trauma Patients With Cirrhosis: Worse Outcomes With Concomitant Alcohol Use Disorder by Phat Nguyen, Areg Grigorian, Jeffry Nahmias, Negaar Aryan, Mallory Jebbia, Sigrid Burruss, Theresa L. Chin, and Lourdes Swentek in The American Surgeon™
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.