
Abstract
Introduction
In 2019 alone, unintentional injuries accounted for approximately 170 000 deaths in the United States (US). 1 While the development of regional trauma systems has significantly diminished morbidity and mortality linked to trauma,2–4 challenges of risk prediction remain a significant hurdle. While valuable in assessing injury severity and estimating outcomes, current trauma mortality prediction scores carry notable flaws, particularly in the early phases of trauma care.
Multiple trauma mortality prediction tools have been developed in order to enhance triage and direct resource allocation.5–10 Unfortunately, none are widely used in clinical practice. In 1989, Champion and colleagues introduced the Revised Trauma Score (RTS), a triage scoring system that incorporates physiologic parameters including the Glasgow Coma Scale (GCS), systolic blood pressure (SBP), and respiratory rate (RR) to predict mortality. 9 However, calculation of the RTS is too complicated for use in the emergency department (ED) and lacks injury specific data. Other trauma scores such as the Injury Severity Score (ISS) and Trauma and Injury Severity Score (TRISS) require information not readily available upon patient presentation, and none are intended specifically for use in patients requiring urgent or emergent surgery after trauma. Simpler scoring systems, such as the Glasgow Coma Scale, Age, and Systolic Blood Pressure (GAP) score, have been introduced to utilize readily accessible information but lack specificity for patients requiring urgent surgical intervention—a critical need considering that over 10% of all trauma activations necessitate emergency surgery, and represent a far larger proportion of those with significant injuries, at highest risk for death. 11
Recognizing this need, this study aimed to develop a novel, easy-to-use and user-friendly Immediate Operative Trauma Assessment Score (IOTAS) tool designed for immediate application in predicting mortality among trauma patients requiring urgent or emergent surgical intervention. In addition, we aimed to compare this against RTS, hypothesizing improved mortality risk prediction accuracy.
Methods
This study was deemed exempt by our institutional review board as it utilizes a national deidentified database. The 2017-2021 Trauma Quality Improvement Program (TQIP) database, a prospectively maintained database including data from over 850 participating centers in the US, was queried to identify patients
The methodology involved two primary phases: first a development phase of the IOTAS, and then a validation phase. Randomization was performed with the Markov chain approach to produce two equally sized datasets. 12 Both groups included patients undergoing any type of urgent or emergent surgery, with no specific surgical procedure exclusions. The primary outcome assessed was in-hospital mortality. In addition, patient demographic information was collected including age, GCS score, and vitals upon arrival.
In developing the IOTAS, a three-step methodology was employed, which has been previously described.13–15 First, multiple logistic regression models were created to determine the risk of death using only variables available at the time of patient arrival and within the derivation dataset. These variables were chosen based on a consensus among co-authors and by a review of the literature for known risk factors of mortality in trauma.16–18 All variables chosen were available upon arrival to the ED, thus allowing us to derive a score consisting of only immediately available variables. Next, variables were then included in a multivariable forward stepwise logistic regression model to identify independent risk factors for mortality using P-value <.05 as the cutoff for statistical significance. The variables that were ultimately selected were age ≥65 years old, GCS <9, tachycardia (HR >120/min) and hypotension (SBP <90 mmHg) upon arrival. The binary nature of all the variables were selected to ensure IOATS was simple and practical to use. The weighted average and relative impact of each independent risk factor was then used to derive the IOTAS. This was done by using the odds ratio and dividing by the lowest common denominator (ie, the lowest odds ratio). This process produced non-integer values which were subsequently rounded to the nearest whole number. To account for error, several iterations were developed for an easy-to-use scoring tool. After each iteration, the receiver operating characteristics (ROC) curve was examined to ensure consistency in the concordance (C) statistic. The C statistic, or area under the receiver operative characteristic (AUROC) curve, measures model success and refers to the ability to discriminate between outcome of interest (death) vs cases without that outcome (survival). 19
Finally, the IOTAS was validated using the validation dataset. The tool’s predictive accuracy was assessed using its C statistic and ability to predict mortality. The IOTAS was then compared to the well-established RTS within the validation set using AUROC. Additional subset analyses of only blunt trauma, only penetrating trauma, alcohol/illicit drug screen-positive, alcohol/illicit drug screen-negative, and a subgroup without traumatic brain injury were performed. These were chosen as some risk prediction tools have been found to perform better for blunt or penetrating trauma and traumatic brain injury can skew risk prediction as well.6,20–23 All analyses were performed with IBM SPSS Statistics for Windows (Version 29, IBM Corp., Armonk, NY).
Results
Mechanisms of Injury and Injuries of Patients Included in the IOTAS Derivation Data Set.
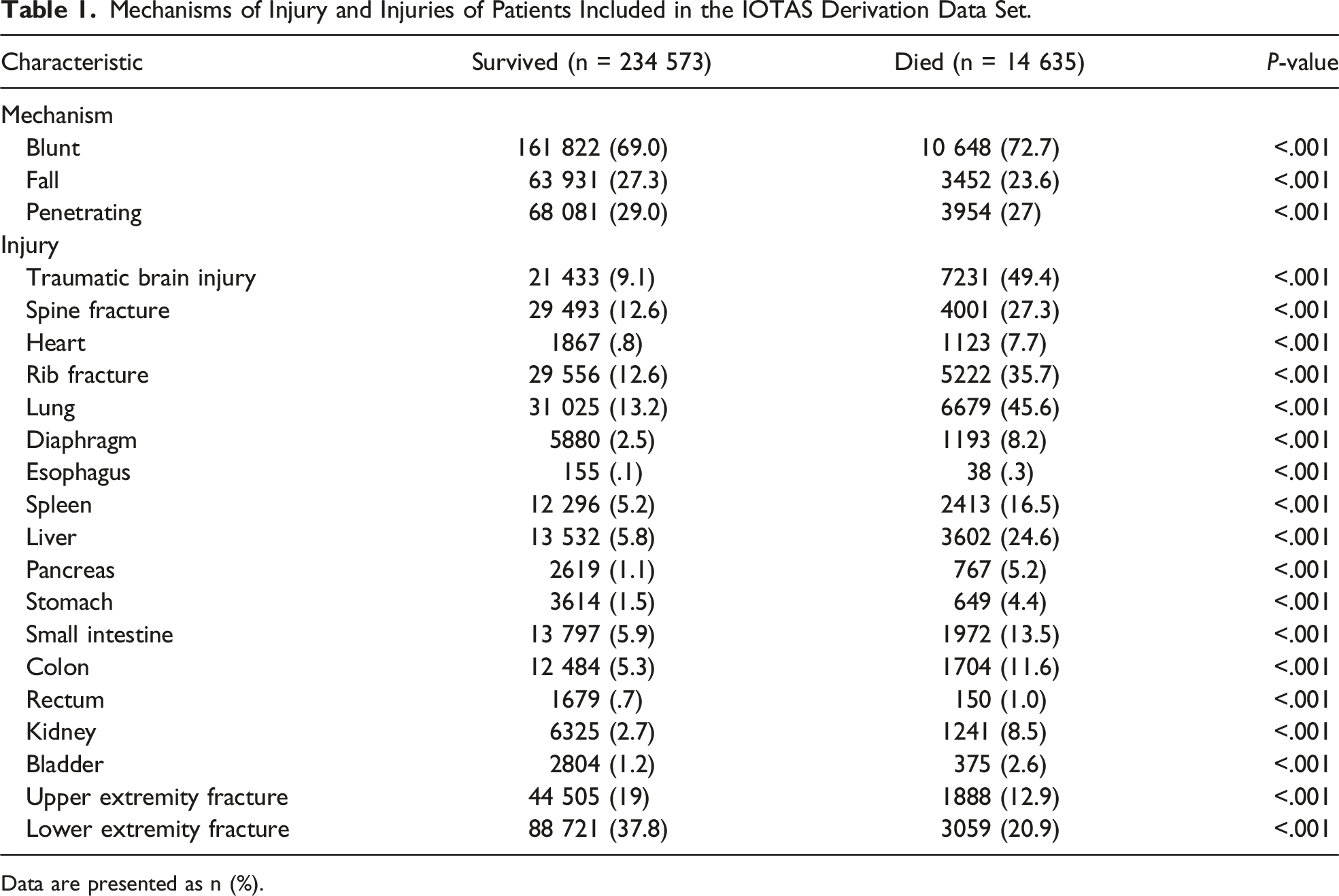
Data are presented as n (%).
Development of the Immediate Operative Trauma Assessment Score (IOTAS) to Determine Risk of Death in Urgent/Emergently Operated Trauma Patients.
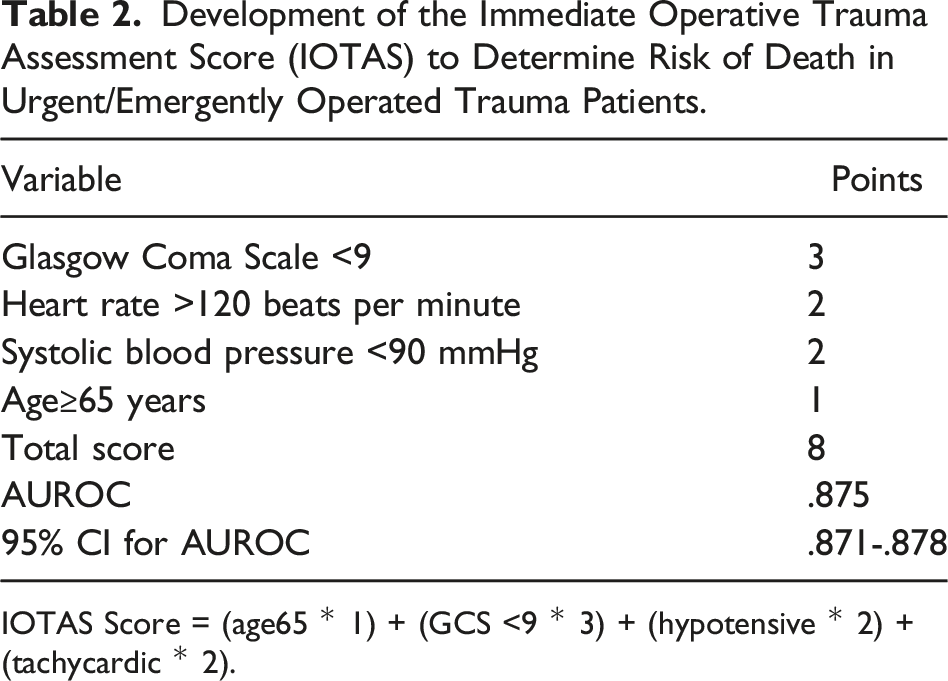
IOTAS Score = (age65 * 1) + (GCS <9 * 3) + (hypotensive * 2) + (tachycardic * 2).
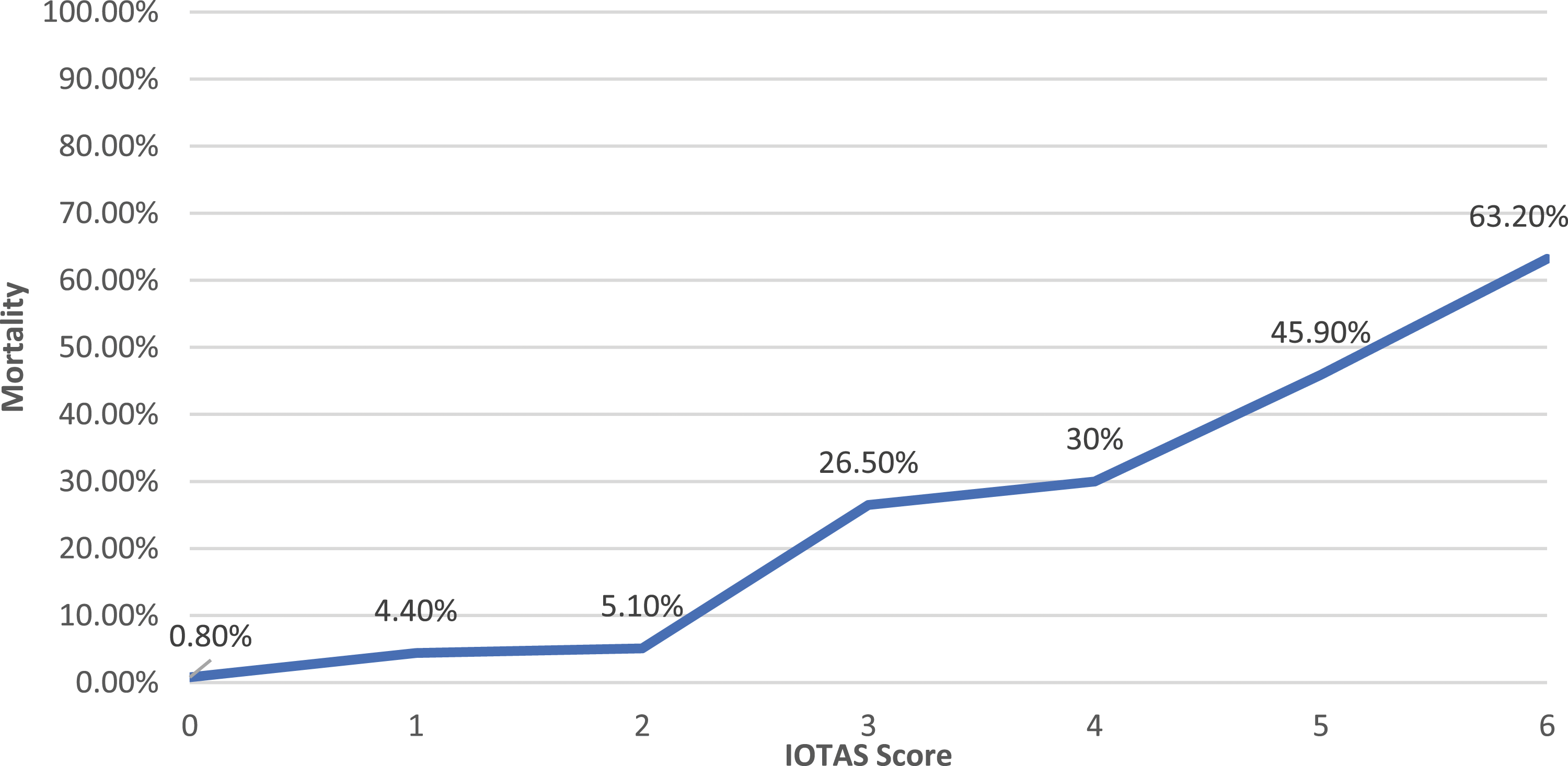
Immediate Operative Trauma Assessment Score (IOTAS) mortality rate.
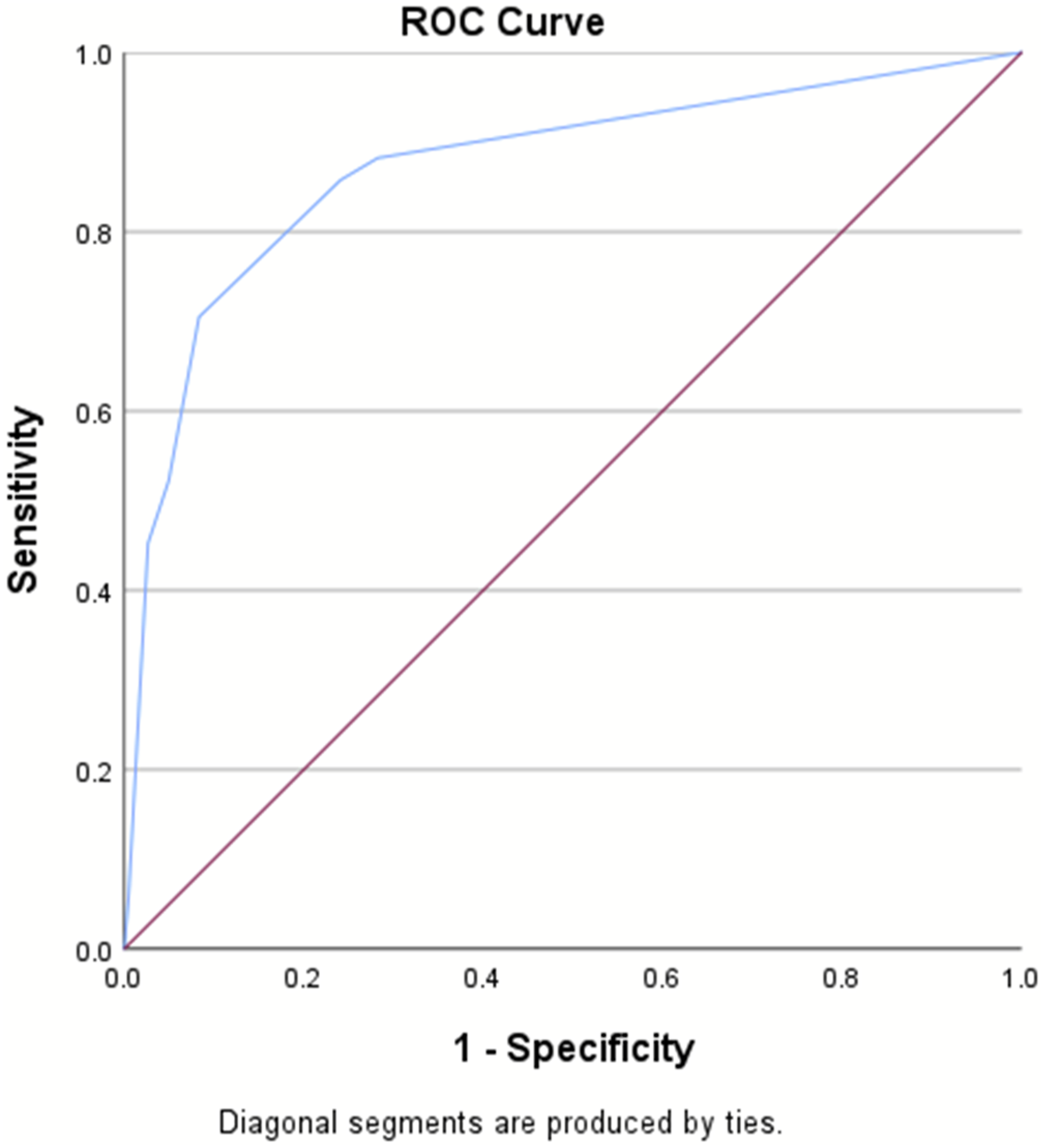
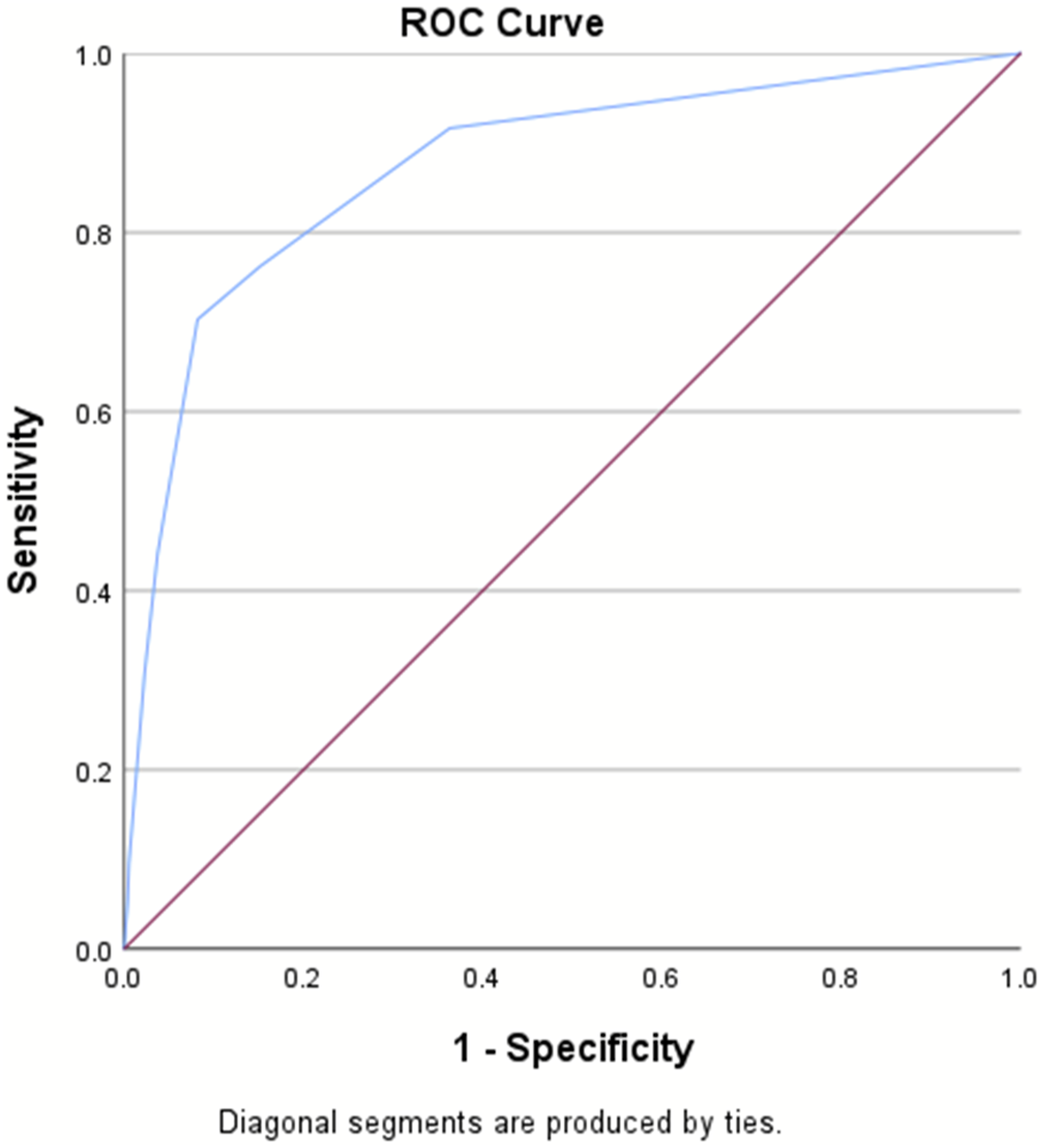
AUROC for the IOTAS in Derivation and Validation Sets and the RTS.

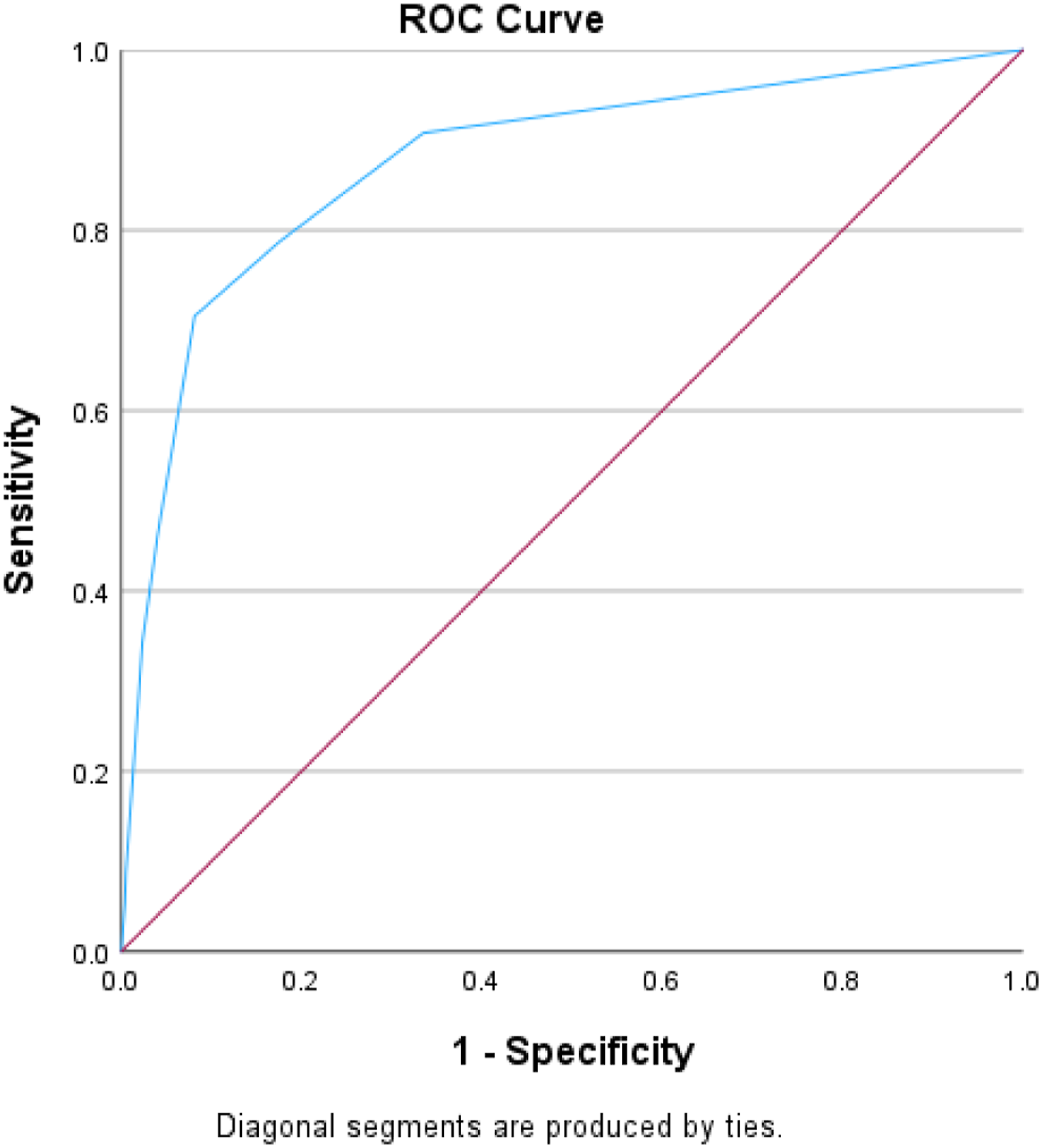
AUROC for the IOTAS in derivation set (AUROC = .88).
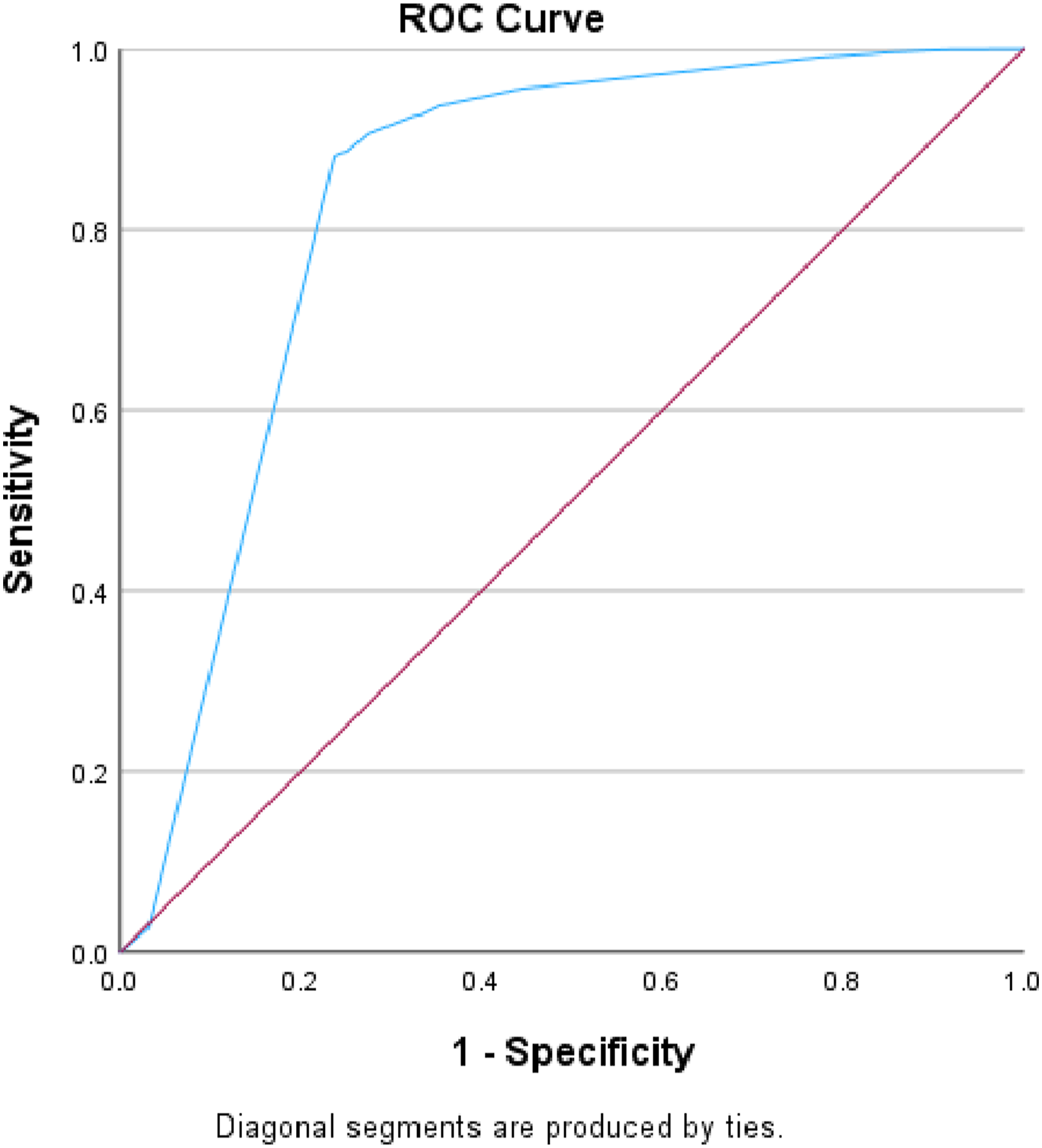
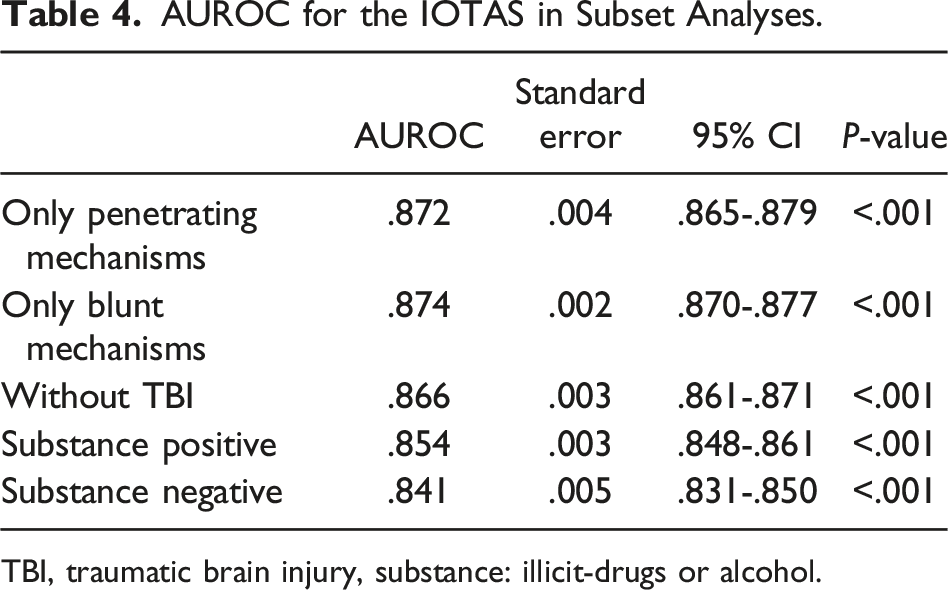
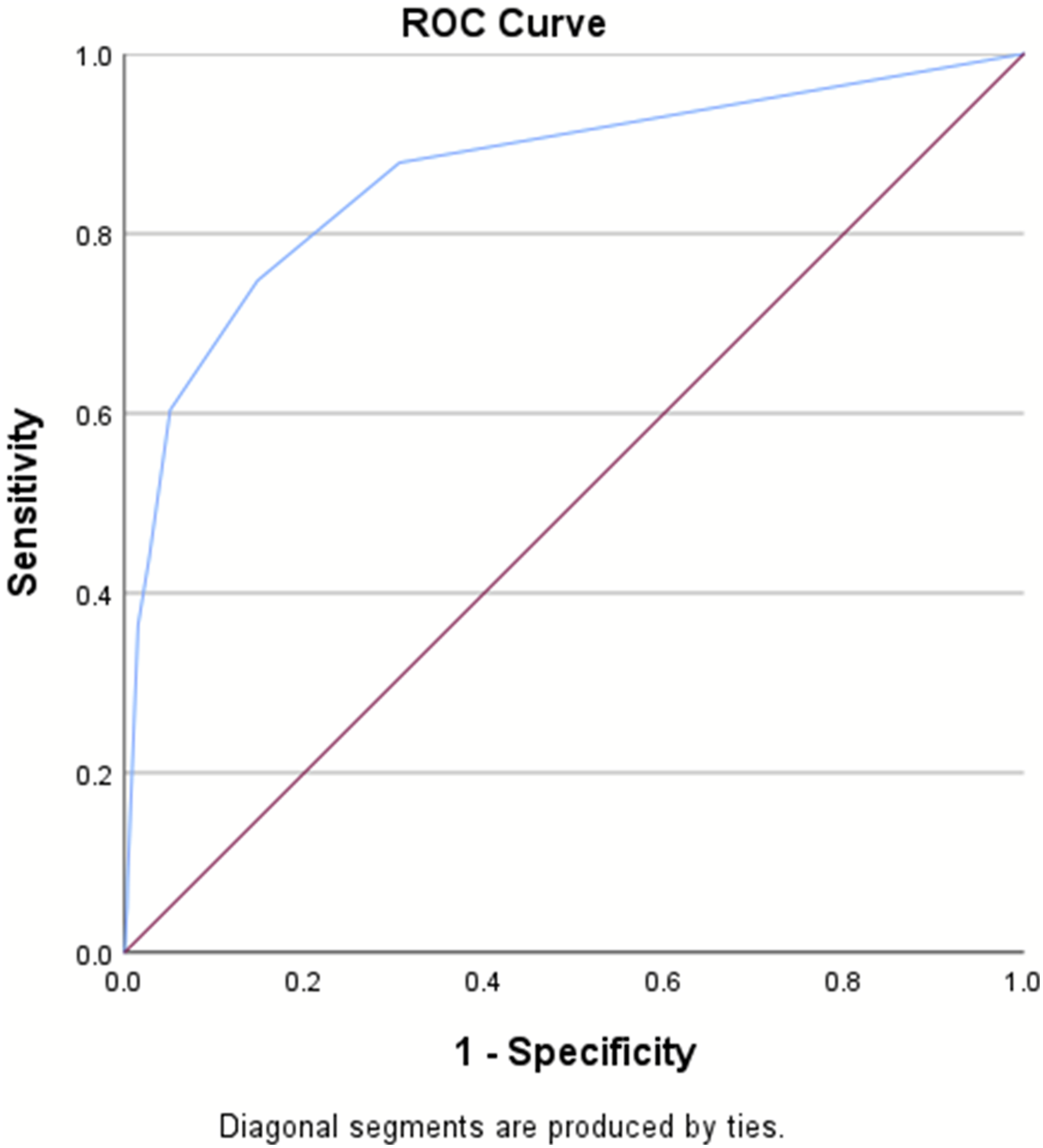
There were 250 182 patients included in the validation set, with an in-hospital mortality rate of 5.8%. The AUROC for the validation set remained consistent at .87, surpassing the RTS’s AUROC of .83 (Table 3, Figures 3–4). The IOTAS continued to perform well in subset analyses of patients presenting with only penetrating mechanisms of injury (AUROC = .87) and only blunt mechanisms (AUROC = .87), as well as a subgroup without traumatic brain injury (AUROC = .87), substance-positive (AUROC = .85), and substance-negative (AUROC = .84) (Table 4, Figures 5–7). Area under the receiver operator characteristics curve for the IOTAS in validation set (AUROC = .87). Area under the receiver operator characteristics curve for the revised trauma score (RTS) (AUROC = .83). AUROC for the IOTAS in Subset Analyses. TBI, traumatic brain injury, substance: illicit-drugs or alcohol. Area under the receiver operator characteristics curve for the IOTAS in subgroup analysis without traumatic brain injury (AUROC = .87). Area under the receiver operator characteristics curve for the IOTAS subgroup analysis with only penetrating injuries (AUROC = .87). Area under the receiver operator characteristics curve for the IOTAS subgroup analysis with only blunt injuries (AUROC = .87).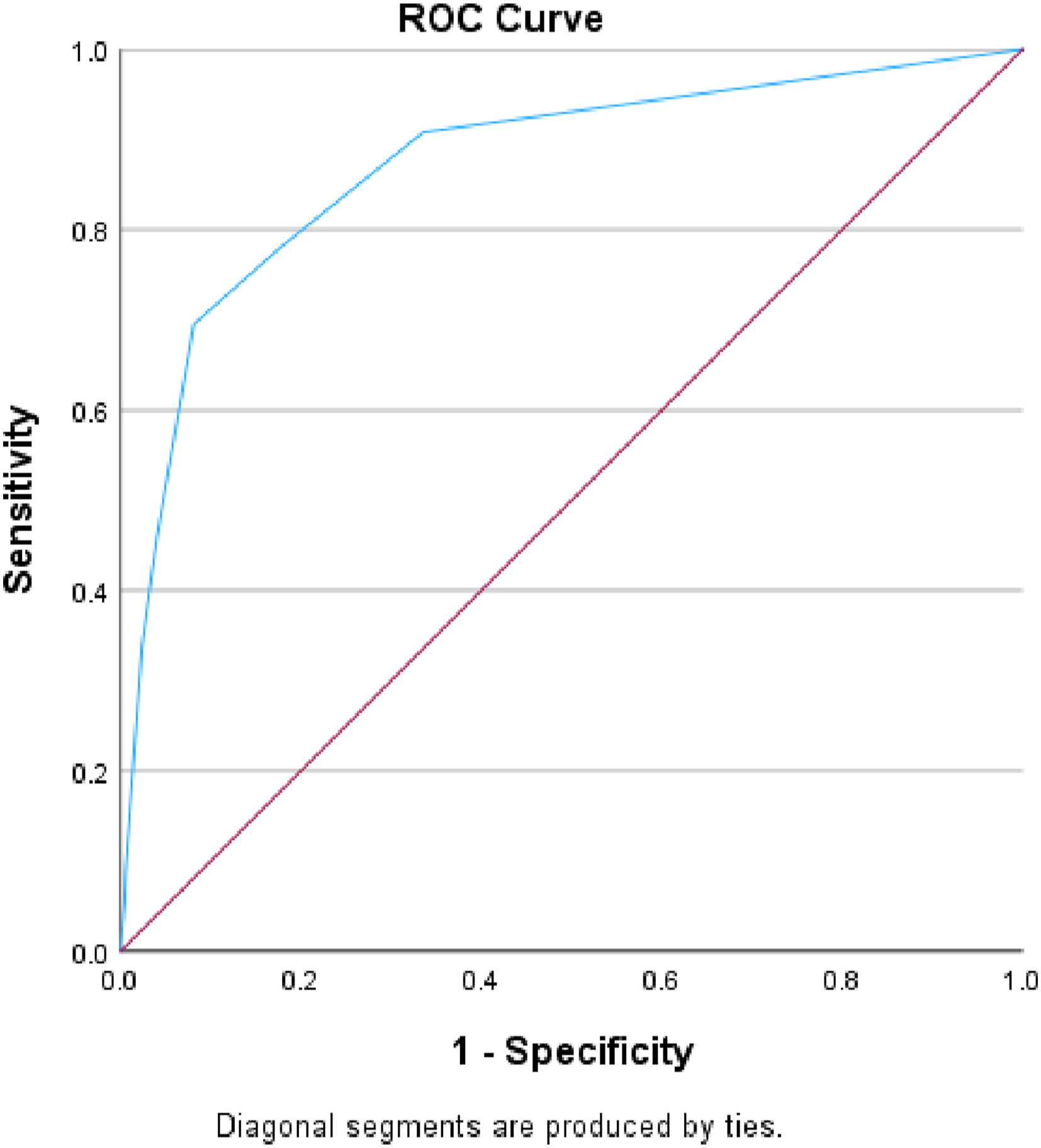
Discussion
Definitive management of the severely injured trauma patient is time sensitive. Existing trauma mortality prediction tools often present challenges: they are either too complex for immediate use or require data not available during the initial assessment of a trauma patient. Moreover, none of these tools are specifically designed for patients in need of urgent or emergent surgical intervention. The aim of this study was to design a practical mortality prediction tool (IOTAS) using immediately available variables, and then compare its efficiency to the widely-known RTS. We demonstrated that IOTAS outperforms the RTS, and thereby may help guide clinicians in practice when counseling trauma patients and their families and can be utilized to compare outcomes between trauma centers.
Multiple trauma scoring tools have been developed and used. The RTS remains one of the most frequently referenced tools and incorporates physiologic parameters including GCS, SBP, and RR. It is not only pivotal in assessing the severity of traumatic injuries but also plays a crucial role in quality control outcomes for trauma centers and provides a “common language” for research studies, facilitating the comparison of trauma populations across different clinical outcome studies. The RTS also comprises the content of the TRISS, 9 which has been shown to strongly predict probability of survival because it incorporates mechanism of injury, anatomic and physiological variables. 23 However, calculation of either the RTS or TRISS is too cumbersome to be performed in the ED and require a complete knowledge of the patient’s injuries, limiting their utility in the early phases of trauma care. Further limitations of the RTS include the poor interrater reliability, particularly when used in the emergency setting. 24 RR, a component of the RTS, is less reliable than other variables due to influences of patient age, mechanism of injury and mechanical ventilation. 10 Validation studies of the RTS have also recognized RR as having poor predictive value for mortality compared to GCS and SBP. 25 Moreover, increasing age, a crucial factor in mortality prediction, is incorporated in IOTAS but absent in the RTS.26,27 To overcome these limitations, the IOTAS employs a binary scoring system that relies solely on readily available variables, while also integrating factors known to significantly influence mortality risk. Furthermore, IOTAS is derived from a cohort of trauma patients undergoing urgent or emergent surgery, enhancing its applicability in high-acuity trauma care, where rapid and accurate decision-making is paramount.
The GAP score, introduced in 2011, represents another evolution in trauma mortality scoring tools. 10 Derived and validated from data in the Japanese Trauma Data Bank (2004-2009), the GAP score is an adaptation of the earlier Mechanism, Glasgow Coma Scale, Age, and Systolic Blood Pressure (MGAP) score derived by Sartorius and colleagues. 28 The GAP score strategically omits the ‘mechanism’ element to enhance its generalizability, particularly relevant given the predominance of blunt injuries over penetrating injuries in their study cohort. 10 While the GAP score efficiently predicts short-term mortality and mirrors the RTS in terms of trauma severity prediction, the IOTAS introduces several enhancements. The IOTAS not only incorporates all the variables of the GAP score but also introduces heart rate (HR), a vital parameter for assessing hypovolemic shock. Isolated vital signs have previously been shown to be unreliable in the assessment of hypovolemic shock; however, the Shock Index (ratio of HR to SBP) is a well-studied and validated physiologic indicator of hypovolemic shock. 29 In the development of IOTAS, tachycardia (HR >120/min) on arrival was identified as independent predictor for mortality and was therefore incorporated into the final version of the scoring tool. And finally, its design is characterized by a binary, yes-or-no approach for each component, simplifying its use in high-pressure emergency settings.
The incorporation of GCS into trauma scoring systems is widely accepted due to its proven significance as a strong predictor of in-hospital mortality.30,31 However, an inherent limitation within the GAP score arises from the weighted value assigned to GCS in categorizing trauma severity and mortality risk. Notably, patients with a normal GCS (GCS 15) are automatically excluded from the “severe” (>50% risk of death) classification according to the GAP score criteria. 10 In addition, substance abuse can impair neurological function, leading to alterations in consciousness levels and cognitive abilities, potentially influencing GCS scores on presentation. These discrepancies in GCS assessments due to substance abuse can introduce variability and inaccuracies into trauma scoring tools that incorporate GCS as a predictor, potentially effecting the precision of mortality risk predictions in clinical settings. To overcome these constraints, the IOTAS integrates a more comprehensive set of variables and continued to perform well in subset analyses, demonstrating reliability in patients screening positive for illicit-drugs or alcohol, patients screening negative for illicit-drugs or alcohol, and in patients without traumatic brain injury. This not only enhances the reliability of the IOTAS but also allows its use in a wide range of trauma patients requiring urgent or emergent operation. Furthermore, unlike other scoring systems that rely on incorporation of specific injury mechanisms, the IOTAS is able to maintain efficacy across both penetrating (AUROC = .87) and blunt mechanisms (AUROC = .87) without explicitly incorporating the mechanism into the scoring system. Thus, it can be applied to urban or rural trauma and potentially used to compare differing types of trauma centers (eg, predominantly penetrating or blunt volume).
This retrospective database study has several limitations inherent to large dataset studies including the potential for misclassification, missing data, reporting bias, and coding errors. It is possible that there are other variables more predictive of mortality risk that are not present within the TQIP database or not evaluated in this study. Additionally, we were unable to calculate mortality risk in IOTAS scores greater than 6 due to sample size limitations. We suspect these rates would continue to increase at higher IOTAS scores; however, further studies with larger sample sizes (possibly with additional years of TQIP data) would be required to verify this assumption. Furthermore, the study does not account for the dynamic nature of trauma care, where patient conditions can rapidly evolve, potentially affecting the applicability of the scoring system in real-time decision-making. Despite these limitations, the IOTAS is derived from and validated using a large national dataset thereby demonstrating generalizability and provides a novel mortality scoring system using only immediately available variables to predict mortality risk in a less studied but high-risk cohort of those undergoing urgent/emergent operations.
Conclusion
In summary, the IOTAS is a validated, practical, and reliable tool to accurately predict mortality in trauma patients requiring urgent or emergent surgical procedures. The IOTAS demonstrates superior performance over the RTS, and effectiveness across various patient subgroups, including those without traumatic brain injury, those screening positive for illicit-drugs/alcohol, and those with either penetrating or blunt trauma mechanisms. Additionally, since this tool is used to predict mortality in those requiring urgent or emergent operations, IOTAS is likely more applicable to critically ill trauma patients. The versatility of IOTAS underlines its potential; however, future multicenter validation studies are needed prior to widespread adoption.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.