
Abstract
Background
Surgical stabilization of rib fractures (SSRF) remains controversial as studies search for the patient population who would benefit most from SSRF. This study aimed to identify the predictive risk factors in patients with chest wall injuries who underwent SSRF and sustained in-hospital complications.
Methods
This study is a retrospective review of the 2016-2019 Trauma Quality Improvement Program database. Data included age, sex, comorbidities, Abbreviated Injury Score (AIS), injury pattern, interventions, and complications. All adult patients who suffered ≥1 rib fracture following an isolated thoracic injury (AIS ≥2 but < 6 and AIS ≤ 1 in all other regions) and underwent SSRF were eligible for inclusion.
Results
A total of 1823 patients were included in this study of whom 4.8% (N = 87) of patients suffered an in-hospital complication. Patients who suffered a complication were generally older, male, had a higher cardiac risk, were more severely injured, and tended to have a longer time to SSRF (3.8 vs 2.5 days, P < 0.001). The top 5 predictors of in-hospital complications were RCRI, thorax AIS, time to SSRF, age, and sex. These variables were sufficient for achieving an acceptable discriminative ability for complications (AUC (95% CI): 0.78 (0.73-0.83)).
Discussion
Cardiovascular risk, thoracic injury severity, and delayed SSRF were correlated with elevated risk of complications. As time to surgery constitutes the sole changeable factor, prompt intervention may substantially diminish postoperative morbidity. These findings can enhance risk classification and assist therapeutic decision making for SSRF.
Key Takeaways
• Cardiovascular risk (RCRI), thoracic injury severity, and delayed surgery were the most significant predictors of in-hospital complications after surgical rib stabilization. • Patients who are older, male, comorbid, and have elevated cardiac risk scores are at a significantly higher risk for complications and should be prioritized for early intervention and enhanced postoperative care. • Among the primary predictors, the duration until surgical stabilization is the sole modifiable variable, underscoring the significance of prompt intervention to mitigate the risk of complications.
Introduction
Traumatic thoracic injury is one of the leading causes of death in the trauma population. 1 Thoracic injuries, including rib fractures, are among the most common traumatic injuries and present significant challenges in patient management, particularly due to the high risk of respiratory complications. Rib fractures following blunt thoracic trauma occur in about 10-20% of all trauma. 2 Rib fractures may lead to compromised respiratory function, increasing the likelihood of in-hospital complications such as pneumonia, acute respiratory distress syndrome, and other respiratory-related issues.3,4 Rib fractures have also been identified as a marker of severe injury and are associated with chronic pain, disability, and low quality of life.3,5
Traditionally, pain control and respiratory support have been the key interventions for rib fracture treatment. 6 Surgical stabilization of rib fractures (SSRF) initially began in the 1950s and has continued to advance and become a more promising option for the management of flail chest and severe rib fractures. 7 Surgical stabilization of rib fractures has shown promise in reducing the risk of complications of rib fractures by improving chest wall stability, pain control, and overall respiratory function. 8 However, despite its benefits, SSRF is not without risks, and identifying patients at higher risk for early postoperative complications remains essential for targeted clinical intervention. 9 Additionally, one study showed that approximately half of the patients had implant-related irritation, and about 10% required hardware removal. 9 Who benefits most and when SSRF should be performed continue to be controversial topics. 9
Currently, there is an established connection between rib fractures and unfavorable outcomes with factors such as advanced age, coexisting comorbidities, and specific injury features contributing considerably to the likelihood of complications. 10 For instance, previous studies have identified that both the presence of rib fractures and an increasing number of rib fractures are associated with mortality and pulmonary complications, including pneumonia.11,12
There remains a paucity of literature on predictors of adverse outcomes in patients following SSRF. Understanding these variables can help physicians with risk stratification, which is critical for optimizing treatment processes and preventing complications. The purpose of this study was to use a well-validated national data set to determine which variables have the highest value for predicting early complications in patients who underwent SSRF following isolated thoracic injury.
Methods
Given that the current investigation used an anonymized, retrospective data set for all analyses, the relevant institutional review board waived the need for ethical approval. The investigation was conducted per the Declaration of Helsinki and the STROBE guidelines. The 2016-2019 Trauma Quality Improvement Program (TQIP) database from the American College of Surgeons was queried for the information needed for the current investigation. This data included age, sex, comorbidities, Abbreviated Injury Scale (AIS), injury pattern, interventions, and complications. All adult patients (age 18 or older) who suffered a rib fracture because of an isolated thoracic injury and underwent SSRF were eligible for inclusion. An isolated thoracic injury was defined as a thorax AIS ≥2 and an AIS ≤ 1 in all other regions. Patients with a thorax AIS of 6 were excluded, as these injuries are generally not considered survivable. Patients were also excluded if any of the explanatory variables were missing to allow for a complete case analysis.
Calculating the Revised Cardiac Risk Index
The RCRI uses six independent and readily available variables: renal insufficiency (defined as acute kidney injury or chronic kidney disease), history of cerebrovascular disease, diabetes mellitus, ischemic heart disease, congestive heart failure, and high-risk surgery. For each variable present, each subject received one point. High-risk surgery is defined as any intraperitoneal, intrathoracic, or supra-inguinal vascular procedure. 13 Surgical stabilization of rib fractures alone was not counted as high-risk surgery.
Statistical Analysis
To describe the sample population, patients were grouped based on whether they did or did not suffer an in-hospital complication. Normally distributed continuous data were summarized using means and standard deviations, while non-normally distributed continuous data were presented using medians and interquartile ranges. The statistical significance of differences between the groups was evaluated using the t test for normally distributed variables and the Mann-Whitney U-test for non-normally distributed variables. Counts and percentages were used for categorical variables. For categorical variables, the Chi-squared test or Fisher’s exact test was applied as necessary. The primary outcome was in-hospital complications (myocardial infarction, cardiac arrest with cardiopulmonary resuscitation (CPR), stroke, deep vein thrombosis, pulmonary embolism, acute respiratory distress syndrome, pneumonia, or surgical site infection).
A logistic regression (LR) model was constructed with in-hospital complications as the response variable. The variables that were included as predictors were age, sex, Injury Severity Score (ISS), highest AIS in each region, time to surgery, intrathoracic injuries, RCRI, 13 shock index, vitals on admission to the emergency room (systolic blood pressure, pulse rate, temperature, oxygen saturation, and respiratory rate), Glasgow Coma Scale (GCS) on admission to the emergency room, as well as comorbidities (hypertension, previous myocardial infarction, congestive heart failure, history of peripheral vascular disease, cerebrovascular disease, dementia, functionally dependent health status, chronic obstructive pulmonary disease, smoking status, chronic renal failure, diabetes mellitus, cirrhosis, coagulopathy, currently receiving chemotherapy for cancer, metastatic cancer drug use disorder, alcohol use disorder, and major psychiatric illness).
The relative importance of the explanatory variables for predicting in-hospital complications was determined using the permutation importance (PI). The PI was determined by evaluating how much a given value (1 - Area under the receiver-operating characteristic curve (AUC)) was changed by the omission of a given variable. Instead of solely eliminating each variable from the data set, the PI method substitutes the variable with noise from other cases by shuffling each variable’s values to mask the variable’s information during evaluation. This process was repeated 10 times to account for the stochastic nature of permutations. The relative importance of each variable in the model was summarized as the mean increase in 1-AUC compared to the AUC in a model including all variables without masking.
As a final step, a new LR model was constructed using the top 5 most important variables based on their PI. The AUC, sensitivity, and specificity that maximized Youden’s index (sensitivity + specificity – 1), as well as the accuracy, were calculated for this model along with their respective 95% confidence intervals (CIs). The CIs for the AUC were calculated using the variance of the AUC as defined by DeLong et al, using the algorithm presented by Sun and Xu. The remaining CIs were approximated with the aid of 2000 stratified bootstrap replicates.
Statistical significance was defined as a two-sided P-value less than 0.05. Analyses were performed using the statistical software R 4.0.5 (R Foundation for Statistical Computing, Vienna, Austria) using the tidyverse, DALEX, pROC, haven, cowplot, and parallel packages.
Results
Demographics of Rib Fracture Patients Managed Using SSRF
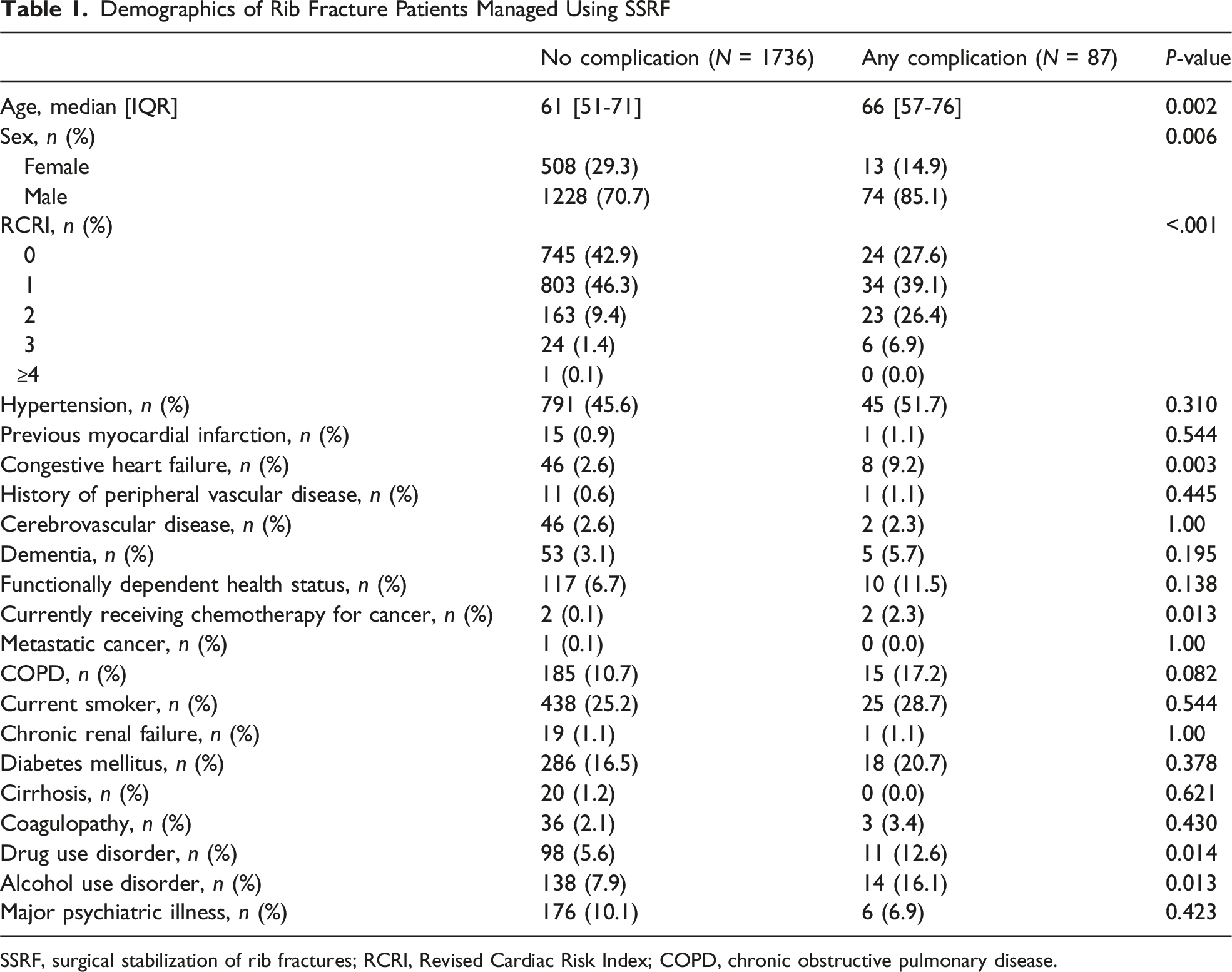
SSRF, surgical stabilization of rib fractures; RCRI, Revised Cardiac Risk Index; COPD, chronic obstructive pulmonary disease.
Clinical Characteristics of Rib Fracture Patients Managed Using SSRF
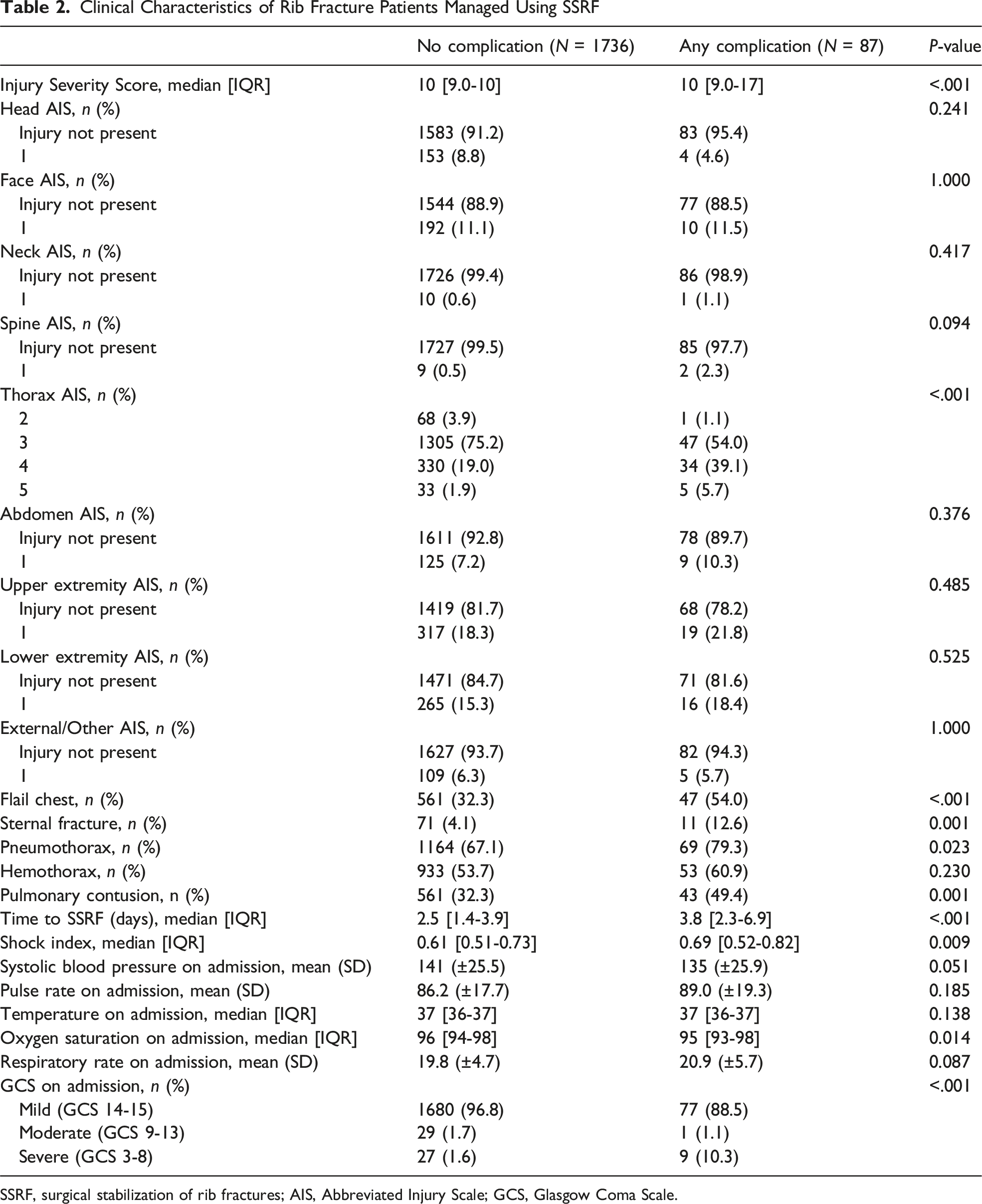
SSRF, surgical stabilization of rib fractures; AIS, Abbreviated Injury Scale; GCS, Glasgow Coma Scale.
Crude Outcomes in Rib Fracture Patients Managed Using SSRF
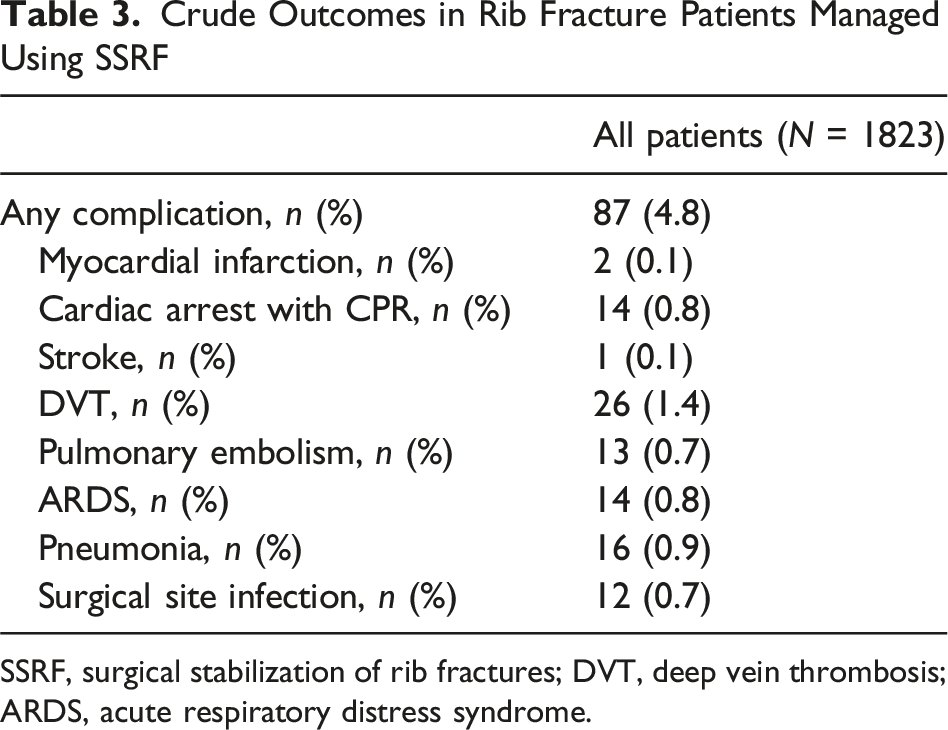
SSRF, surgical stabilization of rib fractures; DVT, deep vein thrombosis; ARDS, acute respiratory distress syndrome.
When ranking the relative importance of variables for predicting in-hospital complications, the top 5 predictors were the RCRI, thorax AIS, time to SSRF, age, and sex (Figure 1). The top 5 predictors were sufficient for achieving an acceptable discriminative ability for complications (AUC (95% CI): 0.78 (0.73-0.83)), according to Hosmer and Lemeshow (Table 4). Top Ten Predictors of Complications. RCRI, Revised Cardiac Risk Index; AIS, Abbreviated Injury Scale; SSRF, surgical stabilization of rib fractures Predictive Ability of Model Using the Top 5 Most Important Variables for Predicting The model for complications uses the RCRI, thorax AIS, time to SSRF, age, and sex as predictors. RCRI, Revised Cardiac Risk Index; AIS, Abbreviated Injury Scale; SSRF, surgical stabilization of rib fractures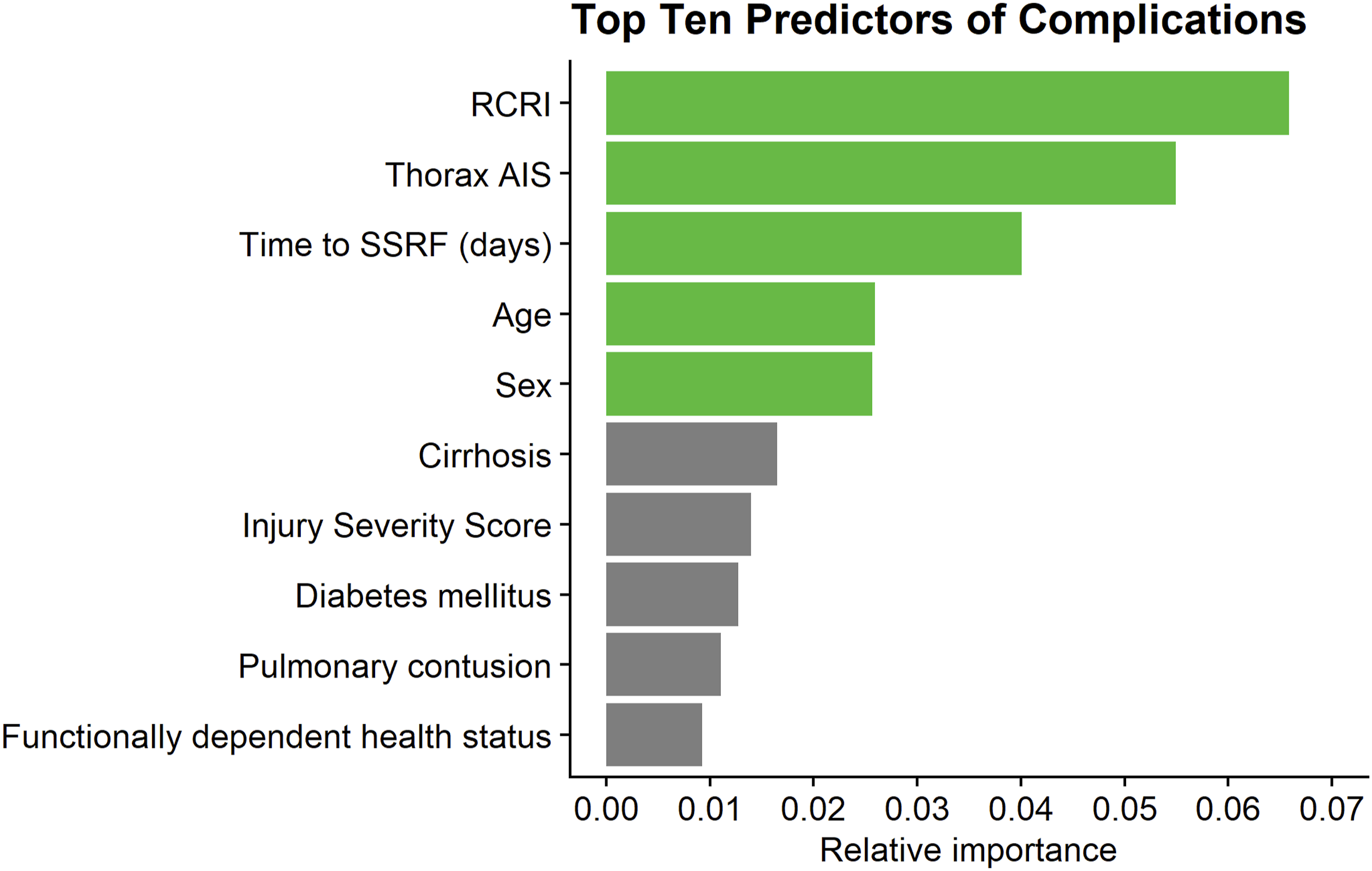

Discussion
To the authors’ knowledge, this is the first study investigating predictors for complications after surgical stabilization for rib fractures in patients with isolated thoracic injuries. The 5 most important variables identified were pre-admission cardiac risk (RCRI), severity of the thoracic injury (thorax AIS), time to surgical rib fixation, age, and sex. Of note, 3 out of the top 5 variables (RCRI, greater age, and male sex) constitute well-known cardiovascular risk factors. Only one factor, time to SSRF, is directly modifiable.
Prior studies have demonstrated comparable findings regarding the importance of the RCRI. For instance, Bass et al 13 conducted a study encompassing all geriatric patients with conservatively managed rib fractures retrieved from the 2013 to 2019 TQIP data set. The study’s authors reported that patients with an elevated RCRI suffered from a significantly increased risk of in-hospital mortality, myocardial infarction, cardiac arrest with CPR, and ARDS. This pattern has also been mirrored in a range of severe injuries, including isolated traumatic spinal injury, 14 isolated severe traumatic brain injury, 15 and hip fractures.13,16 Using this tool, it may consequently be possible to identify patients who would most likely benefit from enhanced postoperative monitoring and critical care expertise. It could also be useful for aiding in goals of care discussions with patients and their families.
Patients who experienced an in-hospital complication in the current investigation also tended to have a prolonged time to SSRF. These findings align with those obtained in prior investigations. Forrester et al 17 demonstrated similar results in their retrospective analysis, using the TQIP database. In this investigation, SSRF more than 3 days after admission was associated with a nearly three-fold increased odds of composite in-hospital complications, a roughly 4-day increase in total hospital LOS, and an approximately 2-day increase in median ICU LOS, when compared with SSRF within 2 days. Likewise, Prins et al demonstrated that in patients with severe chest wall trauma, early SSRF, performed within 48 to 72 h after admission, correlated with shorter hospital and intensive care unit stays, shorter periods of mechanical ventilation, and lower hospitalization expenses. Furthermore, SSRF was linked to a lower incidence of tracheostomy and pneumonia. 18 Wang et al 19 demonstrated that early SSRF in patients with multiple rib fractures could significantly reduce ICU length of stay, overall hospital length of stay, and duration of mechanical ventilation as well as lower the inflammatory response, protect against infection, and substantially decrease the risk of postoperative complications associated with multiple rib fractures. The rates of complications such as pneumonia (7.43% vs 2.99%, P = 0.045) and atelectasis (8.42% vs 1.49%, P = 0.001) were also markedly higher in patients who underwent delayed SSRF than those who received early intervention. Finally, Pieracci et al 20 reported that each additional day in the hospital before SSRF was independently linked to a 31% increased risk of developing pneumonia, a 27% increased risk of prolonged mechanical ventilation, and a 26% increased risk of requiring a tracheostomy. The timing of SSRF and patient selection have been a matter of lively debate during the recent decade. The results from the current study show it to be the only modifiable factor for decreasing the risk of postoperative complication among the top predictors, thus highlighting the need not only for the right patient selection but also for timely intervention.
This study is significantly strengthened by the use of the TQIP data set, a nationwide database contributed to by over 900 sites. However, it is not without its limitations, the primary factor being the retrospective nature of the TQIP data set with pursuant risk of selection bias and misclassification. This also limited the analysis to variables available in the data set and precluded the inclusion of granular data on pain management, the technique used for SSRF, and the specific cause of surgical delay which could been subjected to changes over the study period. Additionally, as the analysis depended on complete cases only, the exclusion of patients with missing data could introduce further biases, potentially impacting the external validity of the findings. Lastly, the use of permutation importance for predictor ranking, though robust, may not fully capture the complex interactions for factors not captured in the database. Future research can improve on these limitations by implementing prospective studies that incorporate more detailed perioperative data to better clarify their influence on patient outcomes.
The key variables for predicting in-hospital complications among patients undergoing surgical stabilization of rib fractures after suffering an isolated thoracic injury consist of cardiovascular risk factors, injury severity, and time to fixation. Other than optimizing perioperative cardiovascular and renal function, time to SSRF is the key variable for mitigating postoperative complications.
Footnotes
Author Note
This work was presented at the 23rd European Congress of Trauma and Emergency Surgery in Lisbon, Portugal (28-30 April 2024).
Ethical Considerations
The relevant institutional review board waived the need for ethical approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. Lukas P. Neff Also is a co-founder of Certus Critical Care Incorporated and have stock options and equity associated with that. He is also a consultant for Plakous Therapeutics and have stock options associated with that, as well as X-Pan medical.
Author Contributions
Conception and study design: EW, MPF, BS, and SM. Literature review: EW, LE, MG, and SM. Data acquisition: BS and SM. Data analysis and Interpretation: MPF, YC, and SM. Drafting of the manuscript: EW, MPF, LE, MG, and SM. Critical revision: All authors critically reviewed and accepted the manuscript submitted.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available upon reasonable request.