
Abstract
Neurogenic Thoracic Outlet Syndrome (nTOS), the most prevalent type of thoracic outlet syndrome, results from compression of the compression of the brachial plexus as it traverses the scalene triangle and rectopectoralis minor space. It typically presents with upper extremity pain, hand weakness, paresthesia, and muscle atrophy that is often exacerbated by arm elevation or overhead activity. Etiology commonly includes congenital anatomical variants, trauma, and repetitive overhead activity. Diagnosis remains challenging as a result of significant symptom overlap with cervical radiculopathy, brachial plexopathies, and entrapment neuropathies. Work up involves a combination of thorough history and physical with electrophysiologic testing, diagnostic injections and imaging such as MRI or duplex ultrasonography. Initial therapy indicates physical therapy with a focus on decompression and postural correction. In patients with persistent symptoms, motor deficits or failed conservative management, surgical decompression using transaxillary, supraclavicular or minimally invasive techniques is indicated. Rib-sparing surgical decompression is increasingly favored given lower complication rates. Postoperative rehabilitation focuses on restoring range of motion and shoulder girdle strength. This review serves to outline clinical presentation, diagnostic strategies and operative options for nTOS while emphasizing an individualized, stepwise approach to optimize outcomes and minimize risk.
Introduction
Thoracic outlet syndrome (TOS) is a group of syndromes involving the compression of neurovascular structures that traverse the thoracic outlet. 1 This thoracic outlet comprises of the subclavian vein, subclavian artery, and brachial plexus passing through interscalene triangle, costoclavicular space, and retropectoralis minor space. 2 TOS has 3 clinical categories, venous, arterial, and neurogenic, and 5 subtypes, arterial vascular, venous vascular, true neurologic, traumatic neurovascular, and disputed.2,3 Neurogenic thoracic outlet syndrome (nTOS) is a subset of this group of syndromes caused by brachial plexus compression. 1 It is characterized by sensorimotor manifestations that are exacerbated by movement. 1 Although TOS itself is a rare syndrome, with an incidence of 1-3 cases per 100,000, nTOS comprises 95%-99% of TOS cases and is recognized by the Society of Vascular Surgery as the primary form of TOS.4-6 nTOS is more common in athletes, musicians and other professions that require an increased involvement of the upper limb. 6 nTOS commonly presents with intrinsic hand muscle atrophy, hand weakness, neurologic sensory deficits, and non-specific pain in the upper limb. Proper identification and diagnosis of nTOS is challenging yet important for determining therapeutic approaches. 7 This review will provide an overview of the etiology, presentation, workup, management, and surgical options as they relate to nTOS.
Anatomy
The thoracic outlet is defined as the space between the supraclavicular fossa to the axilla. The inlet and outlet of the space is formed by the bony circle comprised of the sternum and vertebra connected by the first rib on either side and includes the clavicle, the subclavian artery and vein, the brachial plexus, the scalene triangle, the quadrangular space and the pectoralis muscle. The scalene triangle is bordered anteriorly by the anterior scalene muscle, the middle scalene muscle posteriorly, and the superior aspect of the first rib inferiorly. 8 Distal to the scalene triangle, the quadrangular space is formed by the long head of the triceps brachii medially, the humeral shaft laterally, and the teres minor and major superiorly and inferiorly, respectively. 9
Etiology
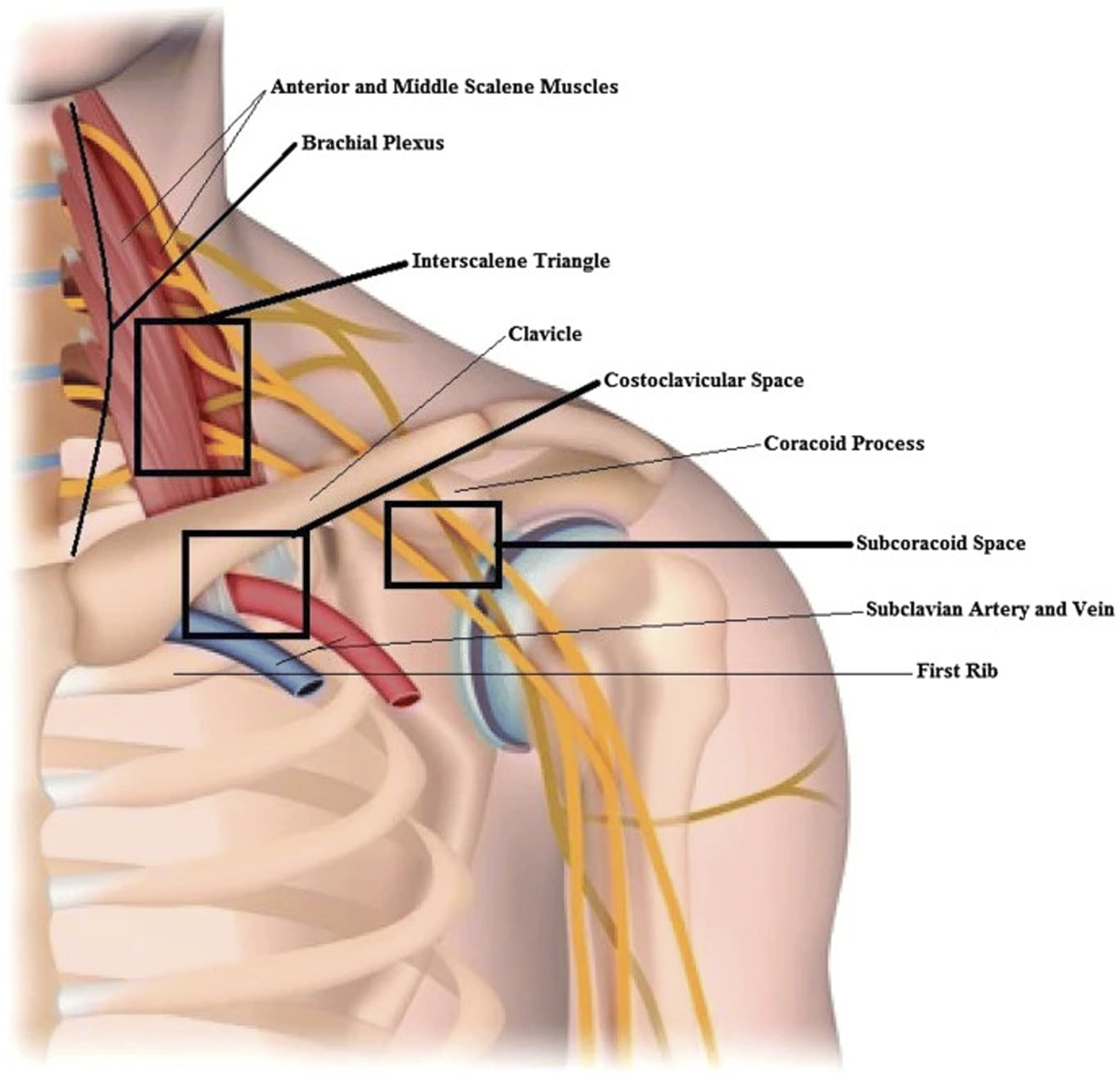
The major structures vulnerable to compression in TOS are the brachial plexus and subclavian vessels. As these structures traverse the thoracic outlet, there are four majors areas of compression (Figure 1).
11
These include the fossa created by the sternal-costovertebral “bony circle,” the scalene triangle, the space between the first rib and the clavicle, and the pectoralis minor triangle, with neurogenic compression most commonly occurring in the interscalene triangle.11-14 Thoracic Outlet Anatomy. Figure Adapted From Jones et al.
10
Compression of the brachial plexus within the thoracic outlet can be as a result of anatomical anomalies, trauma or repeated motions. Abnormalities in thoracic outlet anatomy that contribute to nTOS include the presence of a cervical rib, fibrous and muscular bands, atypical neurovascular structures, variation in the insertion of the anterior scalene, scalenus minimums muscles, or pectoralis muscles. 15 Anatomical abnormalities are a significant contributor to the etiology of nTOS, with 20% of cases accountable to a cervical rib with no other factors. 16
nTOS can also be as a result of trauma, usually through high velocity motor vehicle accident that results in hemorrhage, hematoma, or displaced fracture leading to brachial plexus compression. 17 These high velocity motor vehicle accidents can result in whiplash injuries through forceful bending of the neck anteriorly and posteriorly during the acceleration-deceleration. 18 Whiplash injuries have been shown to have pathogenic significance in the development of nTOS after motor vehicle accidents.5,19
Repetitive motions can also contribute to the etiology of nTOS. Hypertrophy of overused muscles can narrow the space within the thoracic outlet syndrome and compress the brachial plexus. Overuse injuries can also cause compression via swelling, hemorrhages, and fibrosis. 10 Recently, emphasis of the role hyperactivity of the pectoralis minor plays in nTOS pathophysiology has increased as well. This hyperactivity contributes to shortening and fibrosis and leads to decrease in retropectoralis minor space volume due to a chronically protracted scapula position. 20 Patients with this compression at the pectoralis minor space are subcategorized as having neurogenic pectoralis minor syndrome (NPMS). 6 This is contrasted against those who have compression of solely the scalene triangle that are categorized simply as having nTOS. 6
Presentation
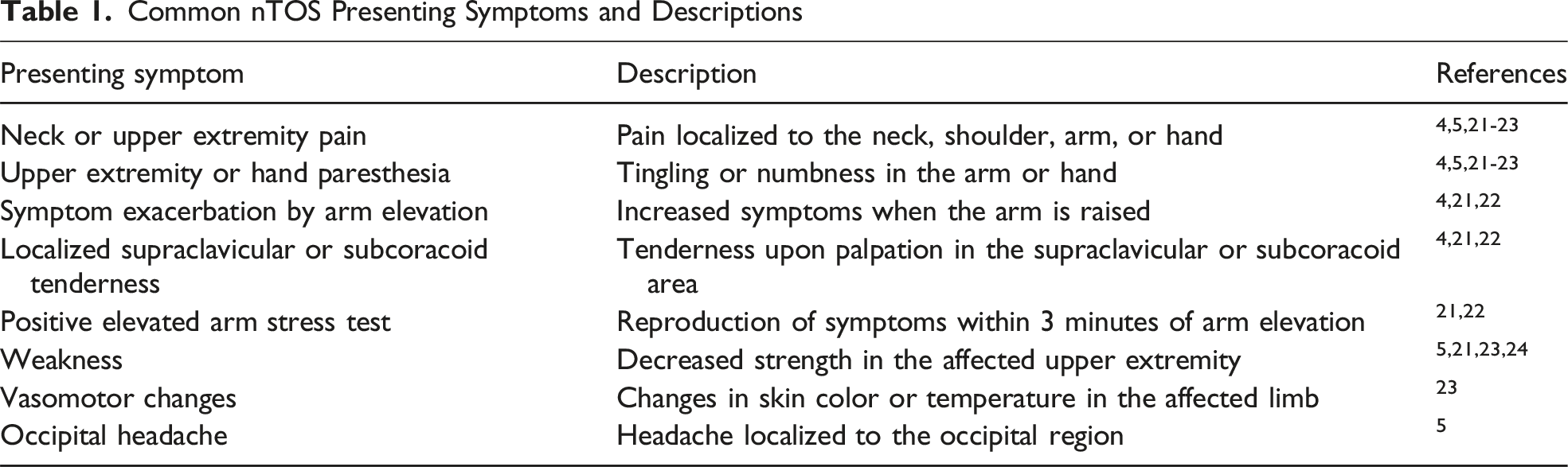
Neurogenic Thoracic Outlet Syndrome most often presents with pain, paresthesia, numbness among other symptoms (Table 1). 5 The penetrance of these symptoms are variable with pain presenting in 73%-90% of previous studies, paresthesia in 32%-98% of previous studies, and numbness in 42%-80% of previous studies. 21 It is important to note that the pain in nTOS can be dependent on arm movement, specifically when the arm is abducted or retroverted. 21 Weakness of the ipsilateral hand, arm and shoulder can be present as well. Multi-study analysis shows a 92%-100% prevalence of hand or finger symptoms in previous studies, 85%-92% prevalence of arm symptoms, 55%-88% prevalence of shoulder symptoms, and 37%-50% prevalence of neck/head symptoms. 21
Common nTOS Presenting Symptoms and Descriptions
Work Up
Diagnosis is difficult because of extensive overlap with other pain and entrapment syndromes. nTOS must be differentiated from other brachial plexopathy causes including “trauma, mass lesions, vascular lesions, brachial plexitis, and cervical spinal cord or foraminal stenosis.” 7 The current standards set by The Society of Vascular Surgery require three of four possible criteria to be met for a nTOS diagnosis. These criteria include (1) signs and symptoms consistent with thoracic outlet pathology including pain and/or tenderness, (2) signs and symptoms consistent with central nerve compression, (3) lack of other pathologies from which the presentation could arise, (4) a positive scalene muscle test injection. 6
Diagnosis of nTOS is based off of history, exam, electrodiagnostic studies and cross sectional imaging. 7 When taking patient history it is important to look for previous trauma to clavicle or thoracic outlet. 21 Additionally, occupation or physical activity that requires increased upper limb use or strenuous upper body positioning should be noted. 6 On physical exam, it is important to note weakness or atrophy in muscle groups (often in the hands) corresponding to compression of any trunk of the brachial plexus. 7 This should be followed by an inspection of the affected limb, cervical spine, neck (scalene triangle), as well as a shoulder examination. 25 nTOS may also present with pain upon palpation of supraclavicular scalene triangle or subcoracoid pectoralis minor insertion site. 25 One of the most informative indications of nTOS is a positive Hoffman-Tinel sign upon deep subclavicular palpation.7,21 Provocative testing including the Adson test, elevated arm stress test (EAST), upper limb tension test (ULTT), supraclavicular pressure test, and costoclavicular maneuver could also be utilized during physical exam, though most are of moderate sensitivity and low specificity.6,21
In the diagnostic process, electrophysiological studies may allow objective differentiation of nTOS from other similarly presenting pain syndromes.26-28 Tsao et al found that EEG studies in nTOS patients show evidence for chronic axon loss process in the lower trunk of the brachial plexus, with the T1 affected disproportionately compared to C8 sensory and motor fibers. 26 This results in studies that primarily involve the T1 root such as the medial antebrachial cutaneous sensory nerve (MABC) and median motor nerves were abnormal in 89% of patients while nerves primarily involving the C8 root were less likely to be affected. 26 Concurrently, meta-analysis found that primarily T1 innervated MABC and C8 innervated ulnar nerves showed asymmetric sensory nerve action potential amplitudes while the median (T1 derived) and ulnar nerves showed asymmetric compound motor action potential amplitudes. 28
“Usually appropriate” for nTOS according to SVS guidelines and The American College of Radiology include US duplex Doppler subclavian artery and vein, which can be used to evaluate potential compression of the costcocervical space, with 31% showing ipsilateral venous or arterial compression with abduction on preoperative scan according to Orlando et al.6,29,30 This can be diagnostically significant when considering the same patients show contralateral compression on Doppler on the asymptotic side 8% of the time. 30 MRI is also often employed in the diagnostic process of nTOS to provide precise localization of compressed anatomical structures relevant to nTOS and allows evaluation of the severity of nerve impingement. 31 Yet another option includes CT chest with IV contrast, which is limited by resolution of nerve structures but can be used to assess bony structures and narrowing of anatomical spaces to aid in secondary confirmations of the diagnosis. 32 Alternatively, a chest radiography or cervical spine series can be utilized to assess presence of a cervical rib and/or elongated C7 transverse process.6,29 Additionally, scoring assessments such as the QuickDASH questionnaire, Cervical Brachial Symptom Questionnaire (CBSQ) and TOS disability scale can be used to assess presence and severity of symptoms and effectiveness of management strategies. 6
Determining whether a patient will benefit from thoracic outlet decompression commonly involves using anterior scalene muscle block, or administration of local anesthetics like lidocaine into the anterior scalene, middle scalene or pectoralis minor muscles. Administration of the block is radiologically guided, usually using MRI, US, or fluoroscopy, and is preceded by local anesthetic administration into skin and subcutaneous tissue.33-35 Scalene muscle block has been shown to have diagnostic value in TOS cases as temporary improvement of symptoms can be seen in those with TOS following an anterior scalene muscle block.34,36,37 Importantly, studies have also found a positive correlation between the degree of percent improvement after scalene muscle block administration and degree of percent improvement following thoracic outlet decompression.35,38 Alternatively, botulinum toxin injection has also shown to have positive predictive value in relation to post thoracic outlet decompression outcomes for nTOS patients in particular.39,40
Management and Outcomes
The first line treatment for nTOS is often physical therapy. In fact, there is satisfactory improvement of symptoms with physical therapy alone in 27% of patients according to one study. 41 Physical therapy in this case would be targeted toward reducing compression across the thoracic outlet while maintaining functional arm use. Manual techniques that address soft tissue/joint mobility restrictions, altered movement mechanics across the cervical spine and shoulder, and pain upon movement are the primary components of a physical therapy approach. Strengthening exercises should be used in conjunction to these and is targeted toward the core and diaphragm to limit the overuse of anterior neck/chest muscles. 42 A conservative approach of this type should be considered in the absence of motor symptoms. 41 In contrast, with weakness, hypertrophy or atrophy of upper limb muscles surgery should be performed promptly. 41
Surgical approaches should be considered when physical therapy alone is unsuccessful in relieving symptoms and is primarily aimed at decompression of relevant neuromuscular structures. This involves the resection of atypical anatomical structures and the anterior/middle scalene muscles, fibrotic tissue that may involve the brachial plexus, and first rib. 43
Complications of a thoracic outlet decompression may include brachial plexus injury in 1%-3% of cases, pneumothorax in 3%-26% of cases, subclavian vein/thoracic duct injury, and injury to sympathetic chain causing Horner syndrome. 21
Common nTOS surgical approaches include transaxillary, supraclavicular, and thoracoscopic. In the transaxillary approach, the patient is positioned in lateral decubitus. An incision is made between the pectoralis major and latissimus dorsi muscles. This provided easy access to the first rib and anterior scalene muscles. Electrocautery is used to dissect the anterior and middle scalene muscles from their origins at the first rib. The rib is, then, elevated and resected (Figure 2).
43
Transaxillary Approach for First Rib Resection. Figure Adapted From Tracci.
44
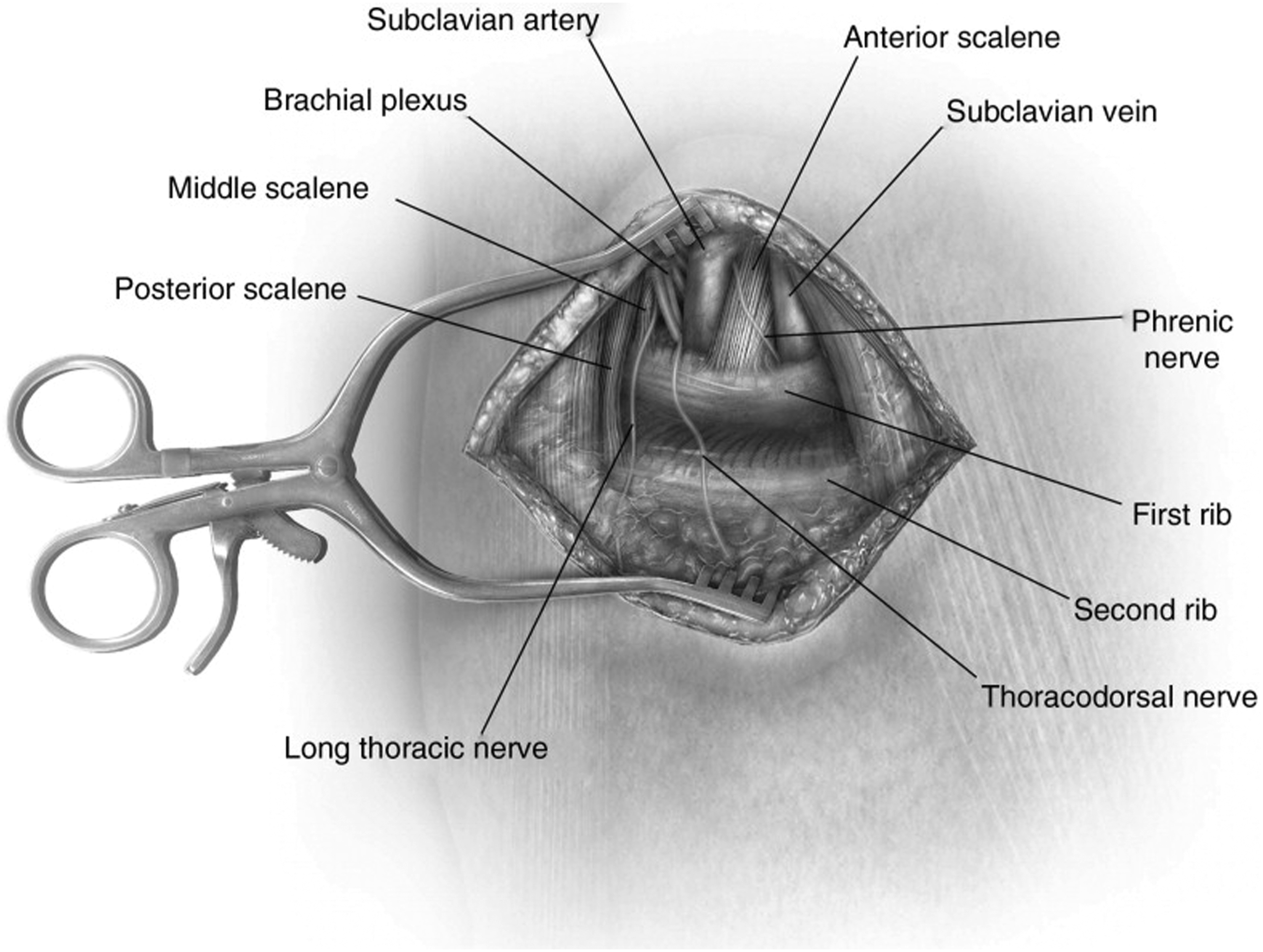
Another common approach is supraclavicular. As the name implies, this requires a transverse incision in the supraclavicular fossa, 1-2 cm superior to the clavicle, and subsequent dissection of the platysma. To preserve supraclavicular nerve function, the lateral head of the sternocleidomastoid muscle and the scalene fat pad are carefully dissected before electrocautery is used to dissect the anterior and middle scalene muscles. This is followed by resection of the first rib (Figure 3). 43 Comparing the two major approaches, the supraclavicular approach provides increased feasibility of the scalenectomy due to better visualization and manipulation of the structures within the thoracic outlet in a shallow visual field. 43 Though it is worth noting that other studies have found that transaxillary and supraclavicular approaches were equally safe and effective in TOS management. 45
More recent developments in nTOS decompression include video assisted thoracoscopic surgery (VATS) which can be aided by robotic technology (Figure 4). VATS requires double lumen intubation to support single lung ventilation as the ipsilateral lung is deflated to create space for the procedure.
47
Thereafter the thoracoscope is inserted in the fifth intercostal space at the midaxillary line.
47
Diathermy is then used to dissect the pleura, intercostal muscles and soft tissue from the first rib before it is resected and the scalene muscles are divided.43,47 Supraclavicular Approach for First Rib Resection. Figure Adapted From Mackinnon and Yee.
46
First rib resections may have favorable outcomes. Nuutinin et al found that after long-term follow up (a mean time frame of 15 years), 80%-90% of patients reported minor or no residual symptoms with stable recovery. 48 Some sparse studies show rib-sparing approaches may be equally effective. Johansen reported that 90.9% of rib-sparing scalenectomies were successful as defined by ≥50% improvement in 3- or 6-month QuickDASH score. 49 Additionally, a meta-analysis from Bolondin et al, indicates that rib-sparing approaches may have higher success rates (97.4% as opposed to 93.2% and 87.9% for supraclavicular and transaxillary approaches, respectively) with lower complication rates (3.6% as opposed to 8.7% and 14.9% for supraclavicular and transaxillary approaches, respectively). 50 To this end, Ruopsa et al found that after a 12 year follow up, 74% of patients reported that the results of their scalenectomy was “good or excellent,” asserting that rib resections may be unnecessary. 51 Still, certain anatomical considerations require first rib resection as it significantly reduces costoclavicular space pressures, helping achieve total decompression in some cases. 52
A systematic review indicates that the transaxillary approach with rib resection has a success rate of 76%, a probability of over 70% improvement at 90%, and a complete relief rate of 53%. 53 This approach has 14% and 5% pneumothorax and neurological injury rates, respectively, and is contraindicated when vascular reconstruction is required in cases such as arterial aneurysm or mural thrombus.43,53 The same review reveals that the supraclavicular approach with rib resection provides, similarly to the tranasxillary approach, a 77% success rate, 87% probability of >70% improvement and a 57% rate of complete relief. 53 This approach has 19% and 4% pneumothorax and neurological injury rates, respectively, and seems to disadvantaged most significantly when considering the access to the most anterior aspect of the first rib, while requiring a most extensive dissection of the supraclavicular nerve, phrenic nerve, long thoracic nerve, and brachial plexus.43,53
VATS provides similar success rates when compared to the more commonly employed transaxillary approach, with each producing a 67% and 63% rate of good or excellent recovery, respectively. 47 Although VATS offers a more clear intrathoracic operative field, the difficulty in visualization of neurovascular bundles prior to dissection may pose an increased risk of incomplete decompression. 43 VATS has shown a 3% risk of brachial plexus injury. 43 More recently, robotic assistance has been integrated into the VATS approach, which allows for 3D images of target anatomy resulting in fewer complications. 54
Postoperative care for patients with nTOS who undergo surgery is centered around prevention of stiffness of the shoulder join through either passive or assisted mobilization of the joint starting immediately after the procedure.
4
Importantly, most postoperative instructions include limiting weightlifting with the affected arm for up to 8 weeks.4,41 This is followed up with resistance and strength training to strengthen and increase functional usage of the shoulder muscles starting at 8 weeks post-op.
4
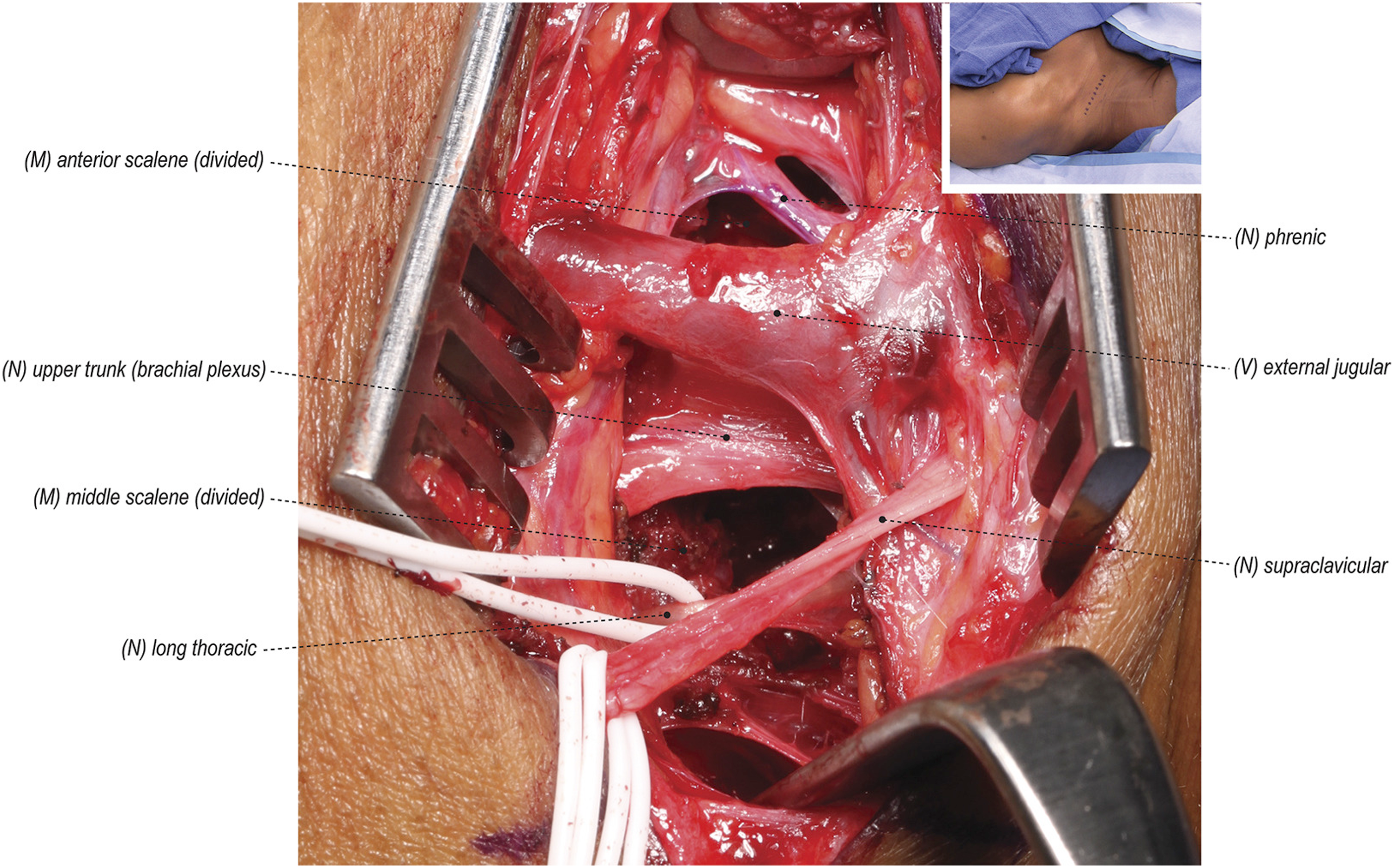
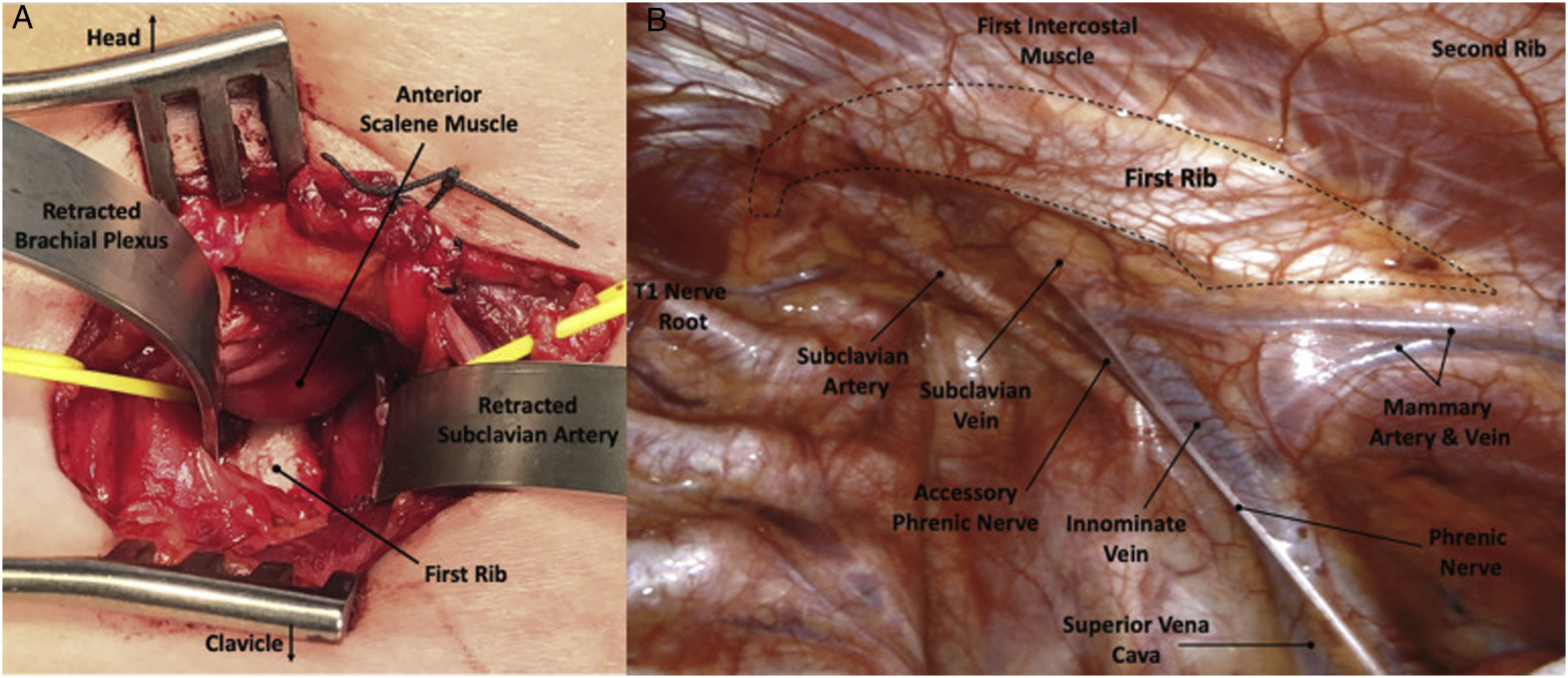
First Rib Exposure via (A) Supraclavicular and (B) Robotic Approaches. Figure Adapted From Burt et al.
55
Conclusion
Neurogenic Thoracic Outlet Syndrome often manifests as a result of neurovascular compression within the thoracic outlet due to trauma, the presence of a cervical rib, or repetitive actions. A nTOS diagnosis requires extensive history, physical examination, and imaging and is often missed or conflated with other similarly present syndromes leading to exacerbation of symptoms. The pain, paresthesia, and numbness can be of minor inconvenience or significantly impact daily living. Despite of a lack of consensus on the best course of treatment, physical therapy and thoracic outlet decompression with or without rib resection offer multiple therapeutic options that have been shown to be successful in the long-term alleviation of symptoms.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.