
Abstract
Introduction
Robotic inguinal hernia repair (RIHR) has been previously compared to laparoscopic (LIHR) and open (OIHR) approaches and found to be safe and effective. However, recent analysis utilizing large national databases is limited.
Objective
To compare the outcomes of RIHR to LIHR and OIHR, including morbidity, mortality and operative time.
Participants
The 2022 ACS National Surgical Quality Improvement database was queried to identify all adult patients with a diagnosis of inguinal hernia who underwent an elective RIHR, LIHR or OIHR. Chi-square and Fisher’s exact tests were used to analyze the categorical data and ANOVA was utilized to analyze continuous variables.
Results
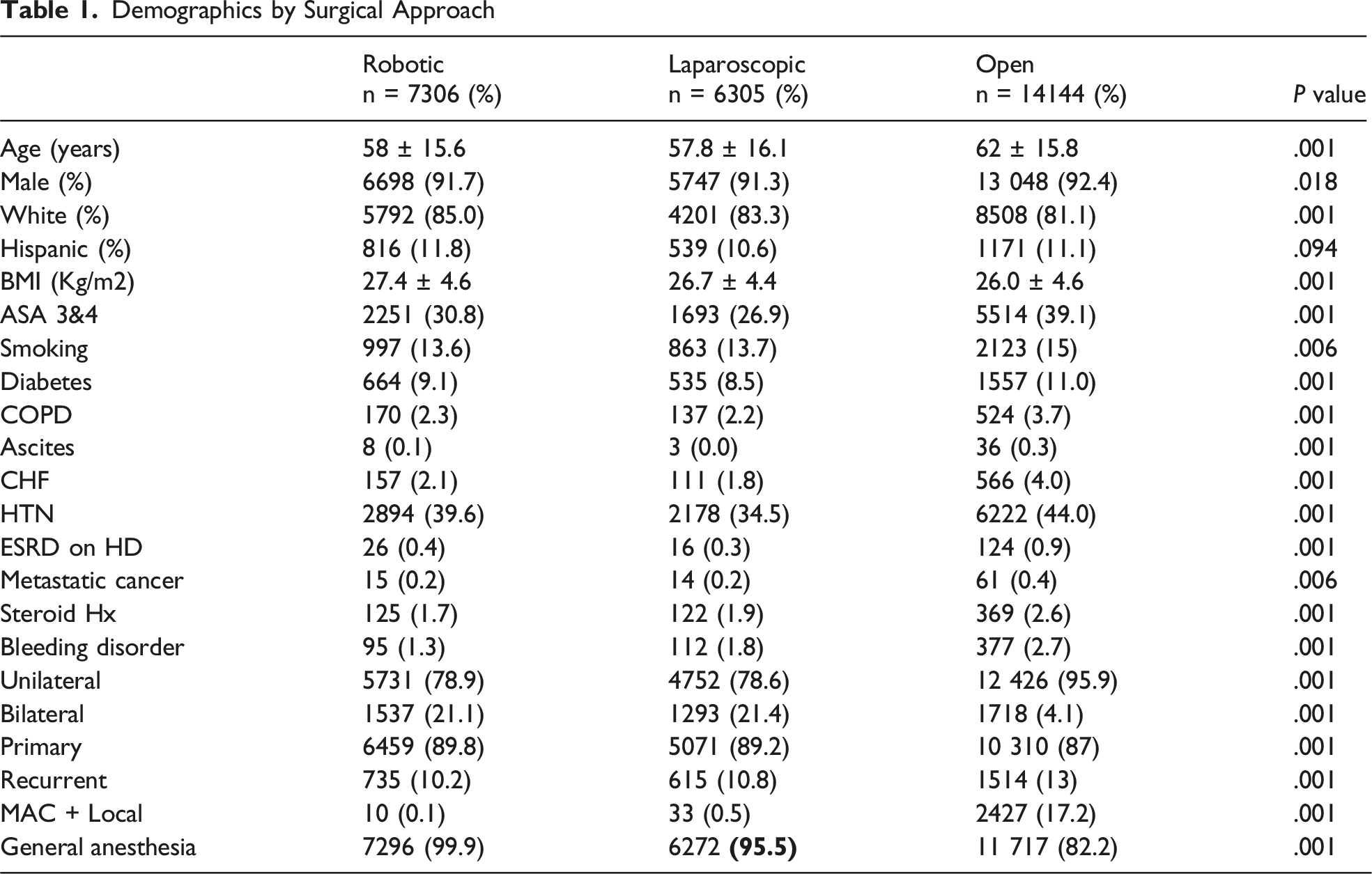
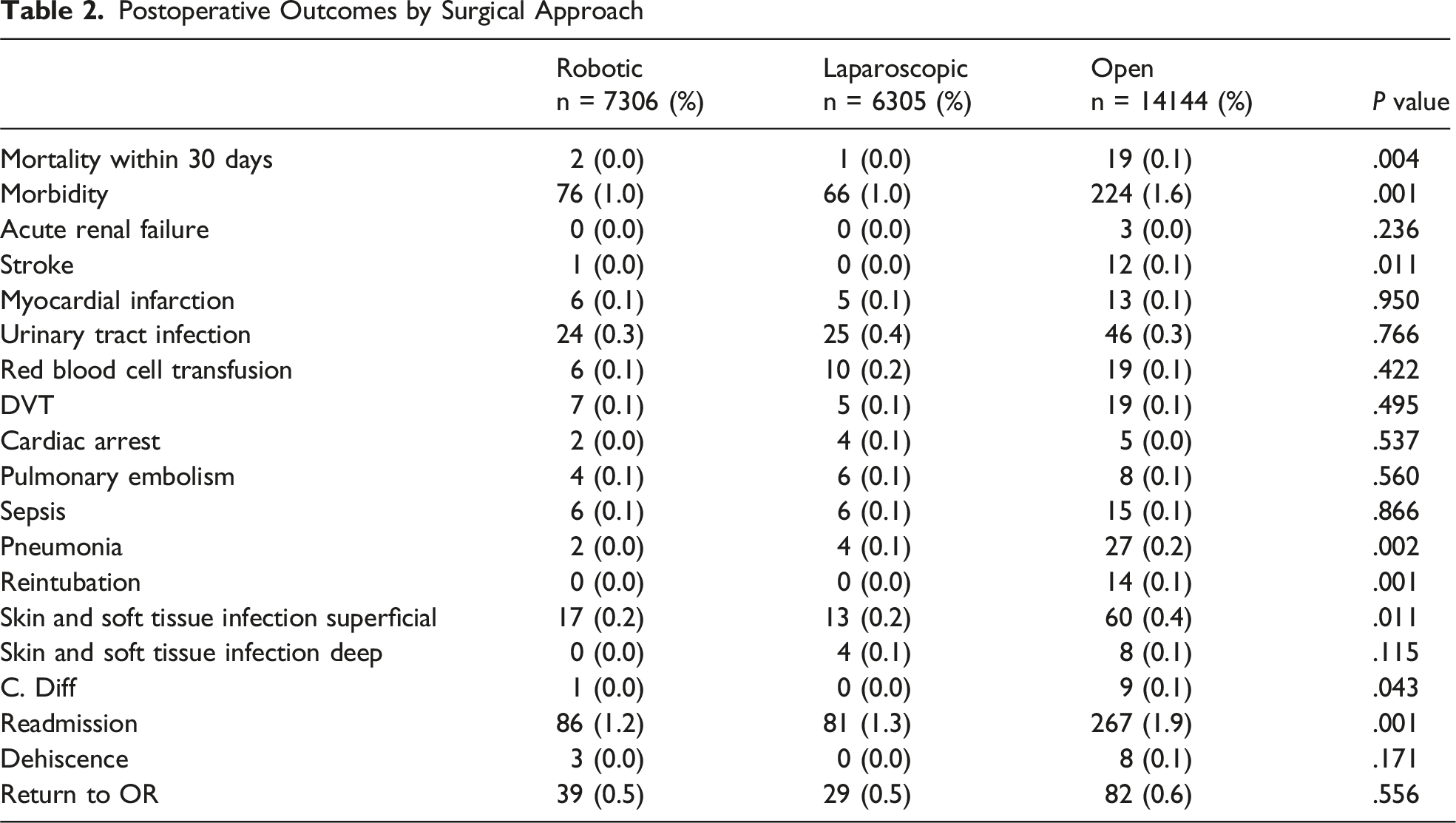
Among 27 755 patients, 7306 underwent RIHR. The robotic approach had the highest average BMI (mean RIHR 27.4 vs LIHR 26.7 vs OIHR 26.0 P =< .001). RIHR was found to be independently associated with longer operative time in multivariate linear regression when compared to the other platforms (LIHR β + −16.894, 95% CI −18.251: −15.538, P = .001 vs OIHR β + −12.056, 95% CI −13.260: −10.852, P = .001). In multivariate logistic regression, approach was not independently associated with mortality (LIHR AOR 0.631, P = .707 vs OIHR. (AOR 3.29, P = .112). However, surgical approach was found to have an independent risk of overall morbidity when compared to OIHR (RIHR AOR 0.702 P = .01 vs LIHR AOR 0.702 P = .01).
Conclusion
In this retrospective study, RIHR is shown to have equivalent morbidity and mortality with longer operative times compared to the other approaches in both initial and recurrent unilateral and bilateral inguinal hernias.
Key Takeaways
• RIHR is shown to have at least equivalent morbidity and mortality compared to LIHR and OIHR. • RIHR is shown to have a longer operative time compared to the other approaches with both initial and recurrent unilateral and bilateral inguinal hernias.
Introduction
Robotic inguinal hernia repair (RIHR) was first described in 2015 by Dominguez et al. 1 Since then, it has been evaluated alongside laparoscopic (LIHR) and open (OIHR) techniques, demonstrating safety, feasibility, and efficacy.1,2 Documented benefits of RIHR include enhanced visualization, reduced acute pain, and improved surgeon ergonomics, whereas drawbacks include potentially higher costs and extended operative times.3,4 Current international guidelines highlight that minimally invasive techniques offer faster recovery times, lower risks of chronic pain, and cost-effectiveness. 5
Previous studies have compared outcomes between RIHR, LIHR, and OIHR in the unilateral hernia patient population; however, no study in the literature has looked at a comparison of short term outcomes, based on surgical approach (OIHR, LIHR, RIHR), recurrence status (primary vs recurrent hernia), and laterality (unilateral vs bilateral).6,7
The objective of this study is to utilize a large database to evaluate the comparative 30-day outcomes of RIHR, LIHR, and OIHR, including mortality, morbidity, operative time, and factors associated with them, including patient’s risk factors, and specific hernia characteristics, such as operative status (primary vs recurrent hernia), and laterality (unilateral vs bilateral).
Methods
Study Design and Data Collection
The study was approved by the Lundquist Institute at Harbor-UCLA, as a non-human subject study. Using the 2022 ACS NSQIP database, adult patients with a diagnosis of an inguinal hernia (ICD10 codes: K40 and subcategories) who underwent an elective inguinal hernia repairs (single procedure without additional CPT codes) were identified using CPT codes (Open: 49 505, 49 507, 49 520, 49 521, 49 525, Minimally invasive: 49 650 and 49 651). This was the first year that robotic data was available in the NSQIP database. Patients who had a minimally invasive procedure and had the field “Robot_used” as “Yes” were categorized as Robotic, and “No” as laparoscopic. Laterality and recurrence were identified using the ICD10 and CPT codes. Data included in the analysis were patients’ demographics, comorbidities, hernia characteristics, and postoperative outcomes.
Outcome Measures
Primary outcomes included 30-day mortality and morbidity. Morbidity was defined as presence of any of the complications collected in NSQIP database. Secondary outcomes focused on operative time, reoperation and readmission rates. Statistical analyses included Chi-square and Fisher exact tests for categorical data and t test and ANOVA for continuous variables. All risk factors with P < .1 were entered into logistic and linear multivariate regression to identify the factors independently associated with mortality, morbidity, and operative times. SPSS, version 28.0 (IBM Corp, Armonk, NY), and 2-sided P < .05 was considered statistically significant. Due to the limitations of the NSQIP database, factors addressing hernia recurrence including smoking, BMI, and other pertinent comorbidities were not specifically assessed.
Results
Demographics by Surgical Approach
Postoperative Outcomes by Surgical Approach
Surgical Approach to Inguinal Hernia Repair vs Operative Time (min)

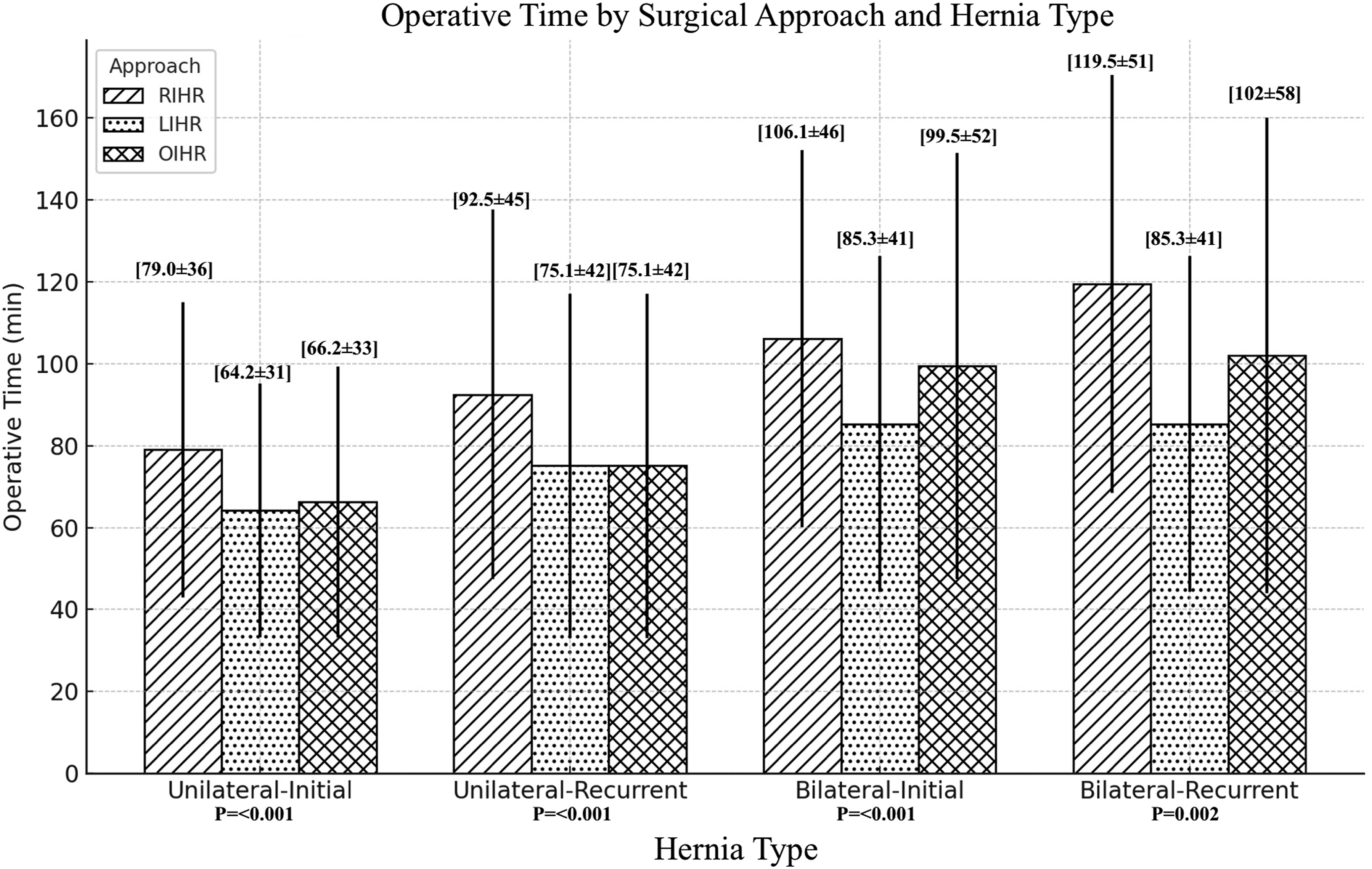
Operative Time by Surgical Approach and Hernia Type
Discussion
In this study which was performed using a large NSQIP data set, RIHR had morbidity and mortality rates comparable to LIHR and OIHR. However, RIHR incurred longer operative times, particularly for complex hernias (eg, bilateral or recurrent). These findings align with existing literature which highlights longer operative times for robotic-assisted repairs. Numerous studies have substantiated that robotic inguinal hernia repair (RIHR) achieves safety and efficacy comparable to laparoscopic (LIHR) and open inguinal hernia repair (OIHR).1-5 However, the clinical indications guiding the optimal selection of these modalities remain a subject of ongoing investigation. Based on the present data set, RIHR has supplanted LIHR as the most performed minimally invasive surgical (MIS) approach for managing unilateral, bilateral, primary, and recurrent inguinal hernias. Additionally, our study showed that RIHR is more often utilized in patients with elevated body mass index (BMI), emphasizing its use in cases with likely increased complexity due to obesity. Conversely, OIHR was the most often used approach for patients with unilateral and recurrent hernias, particularly those presenting with extensive comorbidities. This is likely due to most surgeons’ comfort level with scar tissue within the re-operative field with the open technique where with the MIS approach, the pre-peritoneal plane becomes extensively fibrotic leading to a much more complex dissection.
Notably in our study, the open approach was predominantly utilized in an older demographic characterized by higher American Society of Anesthesiologists (ASA) classifications and a greater prevalence of every NSQIP defined comorbidity compared to the other 2 cohorts. However, OIHR was independently associated with increased postoperative morbidity in the multivariate regression with increased risk of pneumonia, reintubation, soft tissue infections, and Clostridium difficile infections. This increase risk of morbidity did not translate into an independent risk of mortality. These findings align with prior research by Pokala et al, 6 which identified increased rates of postoperative superficial infections in OIHR cohorts.
With an observed decrease in overall morbidity, decreased 30 readmission rate, and decreased SSI rates compared to OIHR within our study, both MIS approaches offer several advantages that merit consideration. With smaller incisions on the abdomen instead of the groin for both LIHR and RIHR, multiple studies have also shown shorter PACU recovery time, decreased use of prescribed pain medication, and faster recovery times compared to the OIHR approach, which can significantly enhance patient satisfaction and quality of life.2-5,8 Both minimally invasive approaches also offer the ability to inspect the contralateral side of the patient for the presence of an occult inguinal, obturator, or femoral hernia. RIHR is particularly advantageous for patients with higher BMI or more complex hernias, as the robotic platform removes the physical burden of operating and allows for multi-arm control by a single individual which may facilitate operating on these more challenging patients. This preference can be seen in the statistically higher average BMI in the robotic cohort. LIHR does not require docking and employs reusable instruments decreasing overall time and total cost compared to RIHR.9-16 Amongst the MIS approaches this data set, RIHR was noted to be the more frequently utilized platform for unilateral, bilateral, primary, and recurrent hernias. However, our study did not account for type of hospital or the presence of residents which could have altered both the selected approach (needing a surgical assist for LIHR) and operative time. For patients who can tolerate general anesthesia and Trendelenburg positioning, both MIS approaches remain excellent platforms for both unilateral and bilateral inguinal hernia repairs.
Our study addresses significant gaps in the understanding of comparative outcomes in robotic-assisted surgery, particularly concerning operative time differences across various hernia presentations (unilateral vs bilateral; primary vs recurrent). Our findings indicate that the time discrepancy between LIHR and RIHR amplifies with increasing surgical complexity: from primary unilateral inguinal hernias (15-min difference) up to recurrent bilateral inguinal hernias (34 min) (Table 3) (Figure 1). This escalating time disparity is noteworthy, given that inherent factors contributing to longer operative durations in robotic surgery such as docking, trocar placement, and patient positioning are largely accounted for in the baseline 15-min difference observed for primary unilateral RIHR cases. Thus, the prolonged operative time in RIHR likely results from a combination of technical and logistical factors. Modifiable factors, including bedside assistance efficiency and the surgeon’s proficiency along the robotic learning curve, may further impact operative duration. Comparatively, LIHR was the faster operation across all hernia presentations (unilateral vs bilateral; primary vs recurrent), only tying with OIHR on the unilateral recurrent presentation (Table 3). With 6305 operations in the LIHR, this clearly shows that this technique is expeditious and remains a cornerstone in general surgeon’s armamentarium. These findings highlight the multifactorial nature of time differentials in RIHR and LIHR and offers the opportunity for targeted interventions to enhance efficiency.
Several studies have examined the learning curve associated with RIHR and its impact on operative times. Ayusa et al (2023) demonstrated a notable improvement in robotic operative efficiency, reporting a 50-min reduction in average operative time over the study period from 2012 to 2020. 16 Similarly, a prior multi-institutional study revealed that after 20 consecutive cases per surgeon (across 10 surgeons), operative times plateaued, with a 17.6-min reduction observed between early and late experiences, decreasing the average duration of unilateral RIHR from 110 min to 88 min. 17 Conversely, Abdelmoaty et al 18 (2018) analyzed cases performed by the top 5 surgeons by volume in their health system of 106 surgeons who still exhibited a persistent 32-min difference in “cut-to-close” times and a 35-min difference in “in-room” times when comparing robotic-assisted to laparoscopic repairs. Our study also continues to demonstrate a consistent surgical time discrepancy between RIHR, OIHR, and LIHR which may result from overlapping learning curves among surgeons, trainees, and support staff, as well as the inherent complexity of robotic systems. Nonetheless, our data could also reflect a true increased in operative time required when performing RIHR.
The lack of hernia characteristics available in NSQIP including size of hernia, previous mesh use, and lack of standardization of surgical technique are limitations in this study. Despite these limitations, this study represents the largest database study to date analyzing the differences between OIHR, LIHR, and RIHR including the total operative time differences for primary, recurrent, unilateral, and bilateral inguinal hernias. Future directions of research should include how the surgeon learning curves effect operative time in procedures for recurrent inguinal hernias.
Our study provides a comprehensive analysis of the comparative outcomes of RIHR, LIHR, and OIHR using a large national database. We demonstrate that RIHR offers advantages such as lower morbidity, reduced readmission rates, and reduced surgical site infections compared to OIHR. However, RIHR, particularly in complex cases, is also associated with significantly longer operative times.
Footnotes
Author Contributions
All authors participated in manuscript writing and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.