
Abstract
Introduction
The burden of traumatic injury in the United States continues to outpace the rate of trauma surgeons entering practice within a larger surgical workforce crisis. Furthermore, a trauma length of stay can be prolonged by many nonsurgical factors, including nonsurgical procedures, medical comorbidities, and socioeconomic barriers to discharge. We hypothesize that using a time-series analysis to predict the likelihood of surgeon-directed procedures can aid trauma centers in redesigning the trauma workflow and more efficiently deploying surgical resources.
Methods
We performed a single-institution, retrospective cohort study, including adult (≥18 years) trauma patients admitted to a level 1 trauma center between 2018 and 2022. Hospital billing and charge data were collected to determine procedure-level data. Procedures were classified as surgeon-directed or non-surgeon-directed. Probabilities were generated based on the likelihood of patients remaining hospitalized and requiring a surgeon-directed procedure.
Results
7382 patients underwent 3138 unique procedures. Of these patients, 6095 (82.6%) had at least one surgeon-directed procedure; 1287 (17.4%) had no surgeon-directed procedure. The length of stay was marginally longer in patients who underwent surgeon-directed procedures. For all patients, the likelihood of needing a surgeon-directed procedure declines each day of admission but stabilizes after day 5.
Conclusions
In our population, the surgical to nonsurgical transition during a trauma admission occurs after day 5. However, this may vary across institutions and not apply to patients requiring complex surgical intervention. Our methods can be used to structure and optimize the deployment of surgical resources only during the period with the highest surgical need.
Key Takeaways
• Care for trauma patients can be complex and resource-intensive, even after recovering from initial injuries. • We performed an adjusted time-to-event analysis of trauma admissions at a busy level I trauma center to determine when trauma patients are unlikely to require surgical intervention. • We found that our patients generally did not require surgeon-directed procedures after 5 days from admission. • We encourage the application of this methodology at other trauma centers to help with the multidisciplinary management of trauma patients and optimize the usage of limited surgical resources. • We do not advocate for removing trauma surgeons from the care of the injured patient.
Introduction
Trauma centers continue to confront workforce shortages and escalating costs of trauma care delivery.1,2 The expenses associated with maintaining trauma center readiness and the necessity for multidisciplinary care present significant operational and organizational challenges.3-7
The approach to redesigning trauma patient care has often focused on expanding the care continuum by adding specialized personnel, such as dieticians and geriatricians.8,9 However, trauma surgeons have consistently remained the primary patient care coordinators. Despite increasingly complex workflows that demand greater coordination, communication, and admissions, the core structure of trauma care in the United States has largely remained unchanged over the past 50 years, with trauma surgeons at the helm.10,11 With the surgeon workforce stretched thin in the U.S., are patients best served and resources best allocated to a trauma service when they no longer require surgeon-directed care (which we define as the point at which patients no longer require procedural intervention under the supervision of an attending surgeon)?1,12-14 In today’s complex inpatient system, much of the effort in caring for trauma patients requiring nonoperative management is centered around addressing chronic comorbidities, arranging safe dispositions, and establishing care with relevant outpatient consultants.15,16 In this setting, patients may fare better on a service with dedicated and trained advanced practice providers or experienced hospitalists rather than a trauma surgeon once they no longer need surgical care.
With an eye for optimizing patient workflows, particularly in busy trauma centers, we hypothesized that in the care continuum of an admitted trauma patient, there is a transition from surgical to medical (nonsurgical) management that may warrant care coordination led by non-surgeon physicians or advanced practice providers outside of the surgical trauma team.
Methods
Study Design
We performed time-to-event and secondary analyses using a retrospective cohort study of admitted trauma patients. The study included patients at a single urban level 1 trauma center admitted between January 1, 2018, and September 30, 2022, and received approval from the Institutional Review Board (protocol 2032314). 17
We identified the trauma cohort using the institutional trauma registry to include adults (≥18 years). Only admitted patients are captured on the institutional trauma registry. We used this cohort to query financial and billing data for each patient. Captured data included all billable procedures, supplies, equipment, and other charges associated with the index inpatient hospitalization. We documented all billable procedures related to facility and physician charges and their associated dates. To identify all billed procedures, we used the billing data to determine when and by whom a procedure was performed. Procedures were then coded as either “surgeon-directed” or “non-surgeon-directed.” A procedure was considered surgeon-directed if a board-certified surgeon performed or supervised the procedure. We included board-certified surgeons from any surgical specialty, including orthopedic surgery, neurosurgery, otolaryngology, and vascular surgery. This was to ensure that all procedures related to the initial injuries would be included in our analysis and reflect our institution’s multidisciplinary approach to caring for the injured patient. Both bedside and operating room procedures were included.
The primary outcome of interest was the likelihood of a surgeon-directed procedure based on hospital day over the first 20 days of trauma admission. Our secondary outcomes included length of stay and trauma activation level (major, minor, or trauma consultation). Potential confounders were identified a priori to determine the impact on survival curves: age, initial systolic blood pressure (SBP), initial Glasgow Coma Scale (GCS), and Injury Severity Score (ISS).
Statistical Analysis
Continuous variables were summarized using medians and interquartile ranges. Continuous variables were compared between cohorts using parametric tests (t-tests) for normally distributed data and nonparametric tests (Mann-Whitney U tests) for non-normally distributed data. Categorical variables were described using counts and proportions and were compared using the chi-squared test. P-values of <0.05 were considered statistically significant. There was no missing procedural data.
We then performed a Cox multivariable regression model to estimate adjusted hazard ratios using our identified confounders. Kaplan-Meier methods were used to calculate daily hazard ratios from admission to hospital day 20. Univariate log-rank analyses were used to generate survival curves for selected covariates. Demographic and clinical cohort comparisons were performed using Stata Software (v.18. College Station, TX: StataCorp LLC). Time-series analyses were performed using R Statistical Software (v4.1.2; R Core Team 2021).
Results
Over the study period, 7382 adult trauma patients were admitted to the trauma center. This cohort had 3138 unique procedure codes attached to their admissions. Of these codes, 2251 (71.7%) were defined as surgeon-directed.
There were 6095 (82.6%) patients who had at least one surgeon-directed procedure during their admission; 1287 (17.4%) had no surgeon-directed procedures during admission. Patients who underwent a surgeon-directed procedure were younger (55 vs 60 years, P < 0.0001). There is a male preponderance in the cohort (57.7%), but a lower percentage of the male population underwent a surgeon-directed procedure (56.3 vs 64.3%, P < 0.001).
Demographic and Clinical Factors of Patients Included in Our Cohort
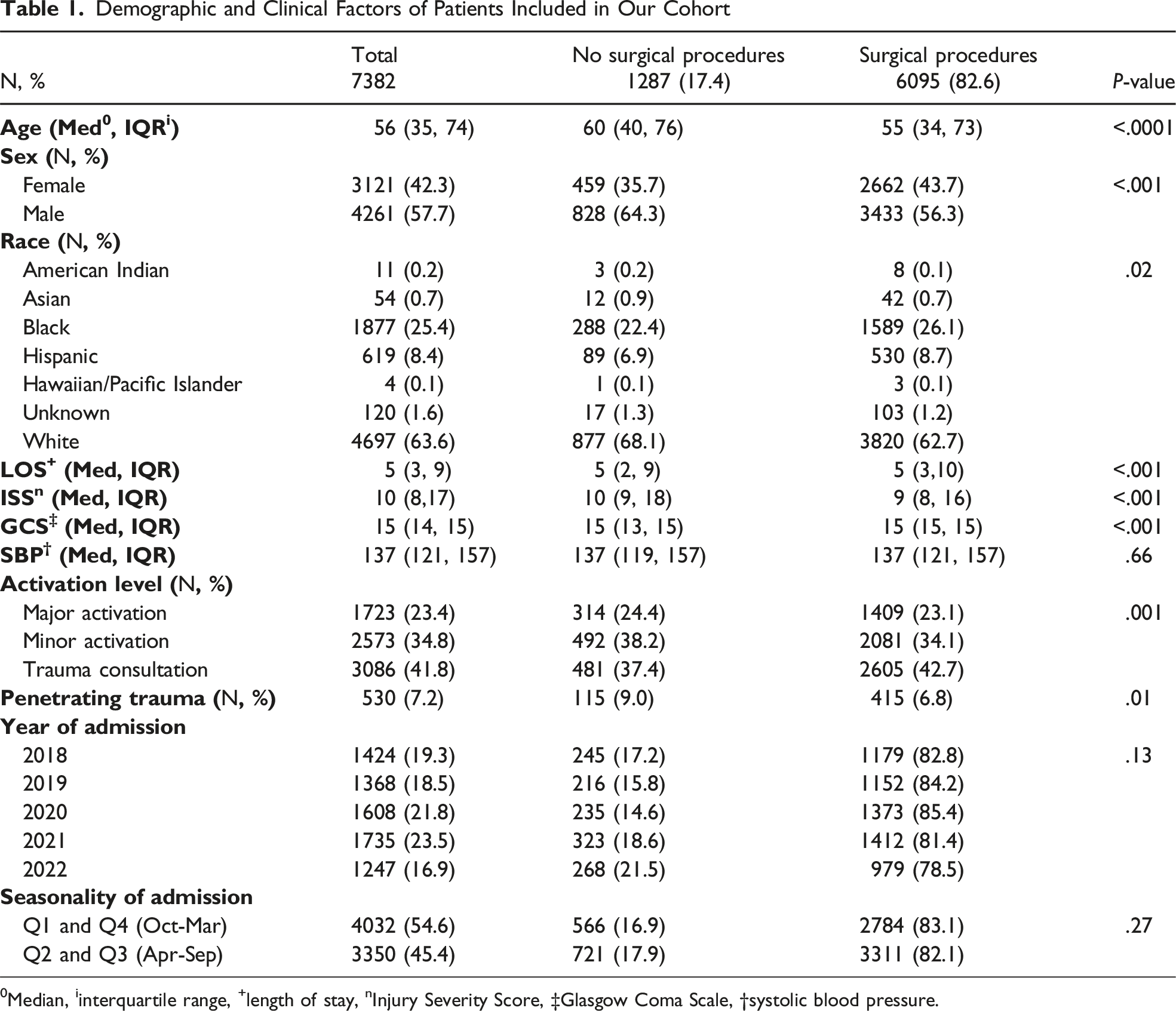
0Median, iinterquartile range, +length of stay, nInjury Severity Score, ‡Glasgow Coma Scale, †systolic blood pressure.
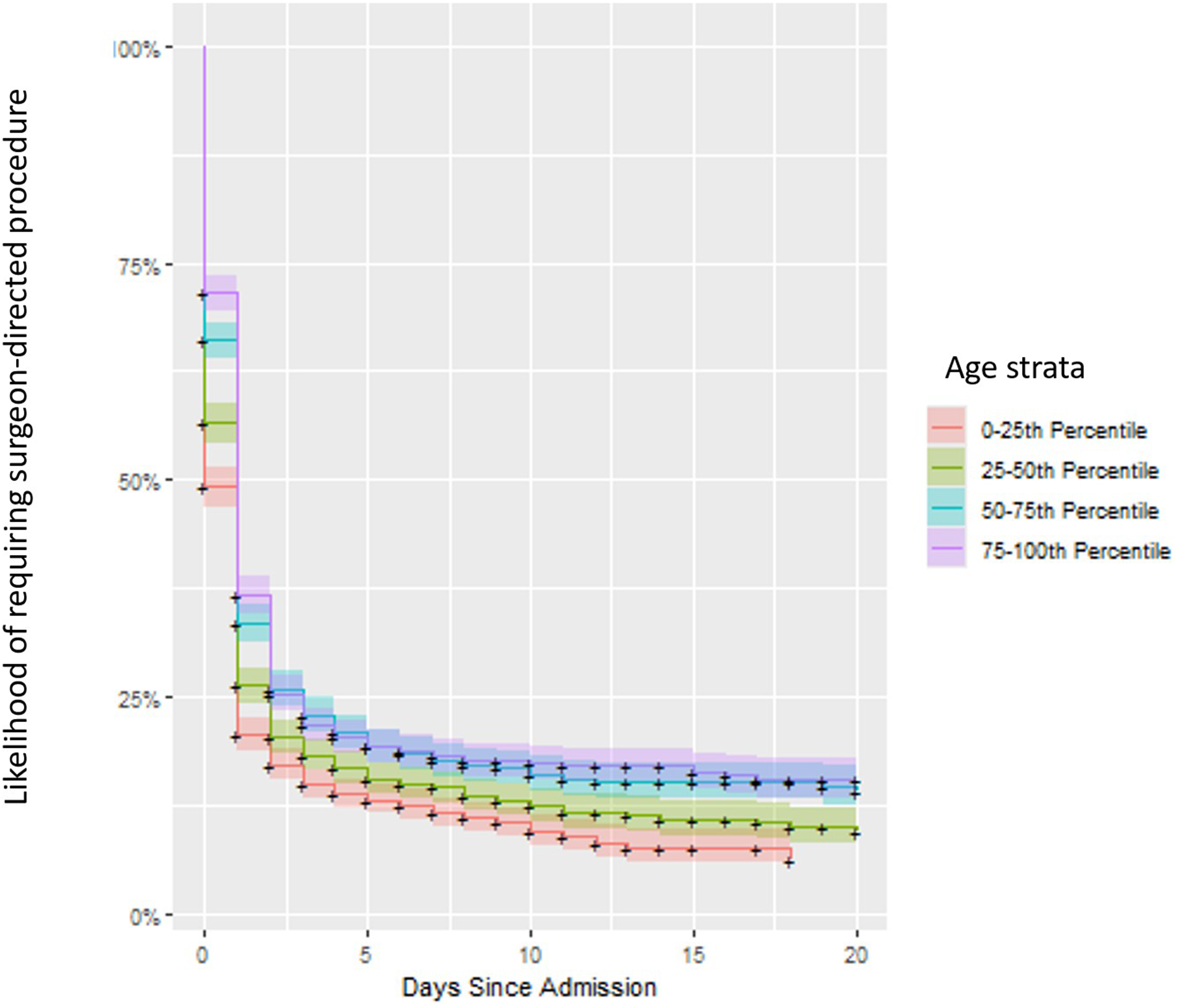
The daily hazard rates for the likelihood of surgeon-directed procedure after adjusting for confounders are listed in Appendix 1. Univariate adjusted log-rank analyses demonstrated that patients admitted without trauma activation had the highest likelihood of a surgeon-directed procedure (P = 0.01). Additionally, increasing age was associated with decreasing likelihood of surgeon-directed procedures (P < 0.001). There was no association between systolic blood pressure on admission and the likelihood of a surgeon-directed procedure. Figure 1 shows that the likelihood of requiring a surgeon-directed procedure drops rapidly from admission to a nadir at around hospital day 5 in our cohort. Figure 2 shows that these trends remained static even after stratifying by age. Additional stratification by trauma activation level and SBP also exhibited similar trends. Smoothed Hazard Curve Indicating Likelihood of Requiring Surgeon-Directed Procedure Over the Course of 20 Days From Admission. The Likelihood of Requiring a Procedure Drops Sharply by Hospital Day 5 in our Cohort. Kaplan-Meier Survival Curves for Each of the Age Groups Binned Into Quartiles With Shaded 90% Confidence Intervals for Likelihood of Requiring a Surgeon-Directed Procedure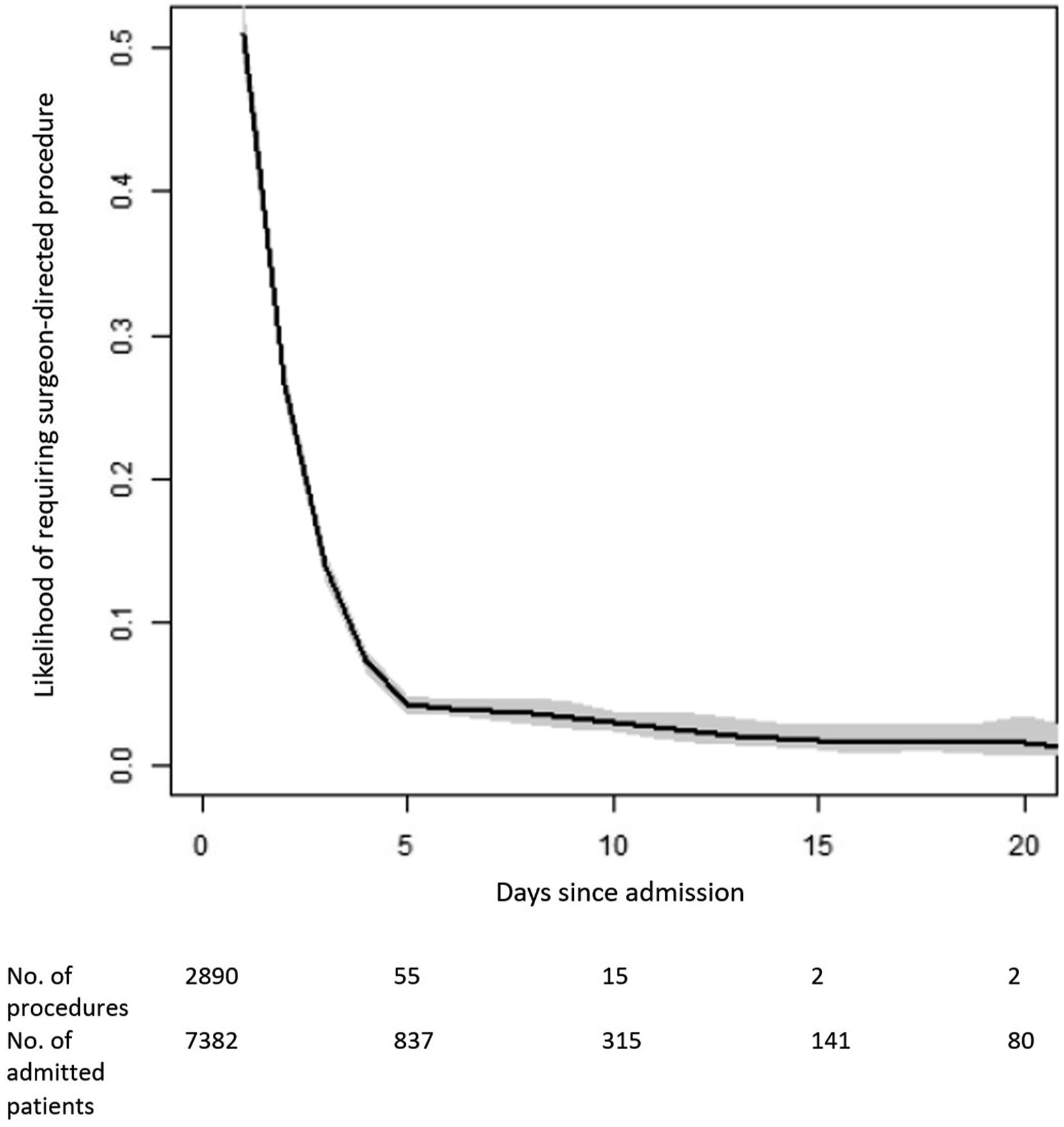
Discussion
This retrospective study evaluated whether there is an approximate day of admission at which a trauma patient’s likelihood of requiring a surgeon-directed procedure is significantly decreased to aid in appropriate workforce deployment and allocation. On multivariable analysis, factors affecting the likelihood of a surgeon-directed procedure included age and lack of initial trauma activation. Importantly, from day 5 onward, most trauma patients admitted to a trauma service at a busy level 1 trauma center no longer required surgeon-directed procedures. Additionally, the median length of stay for all patients in our cohort was about 5 days (ie, 50% of patients were discharged by day 5), which is expected as most patients who required invasive intervention completed their procedures by day 5 of their admission. Because the likelihood of requiring a procedure can influence a patient’s LOS, but not vice versa, we opted not to adjust for LOS in our hazard analysis for requiring a surgeon-directed procedure in Figure 1. Moreover, we considered LOS a secondary outcome, not an exposure. We adjusted for other risk factors that could impact both outcomes.
This novel study shows a discrete time when the likelihood of requiring a surgeon-directed procedure is lowest. To our knowledge, this is the first study of its kind to examine the post-acute risk of requiring surgeon-directed intervention for admitted trauma patients across several years in a diverse level I urban trauma center. This transition point may be vital to optimizing the allocation of resources in a specialty that continues to experience workforce shortages. 18
While advancements in nonoperative management of traumatic injuries have resulted in decreased morbidity for patients, the increasing proportion of nonoperative trauma admissions may be perceived as a burden for surgeons, especially for trainees. 19 Some have raised concerns that this has detracted from the field of trauma surgery, raising the question of whether trauma surgeons are too relied upon for care coordination for surgical subspecialists. 20
Despite this shift towards nonoperative trauma care, our findings demonstrate that many trauma patients require surgeon-directed care, the majority of which occurs in the first 5 days of admission. As shown in earlier studies that examined trauma service admissions, surgical evaluation of patients early in the hospital course is associated with improved clinical outcomes and efficiency, and we continue to advocate for close involvement from trauma services in the critical early admission period. 10 Many patients are discharged after a few days (median LOS of 5 days in our cohort) (often from a dedicated trauma service), even if they require a surgeon-directed procedure. 21 That said, our findings demonstrate that after this critical early period, trauma patients are unlikely to need the resource-intensive services of a trauma surgeon. Thus, we sought to address the question of trauma patients who remain admitted despite having survived the initial course of their presenting injuries or who had minor injuries to begin with but lacked safe disposition.
Within our cohort, older and non-trauma-activated patients requiring admission were less likely to have a surgeon-directed procedure during their admission. This finding suggests that some patients are admitted or remain hospitalized for nonsurgical reasons. Such patients may require the expertise and care coordination of medical or palliative care teams, particularly surrounding issues of safe disposition and goals of care. 22 While general and trauma surgeons are qualified to manage these complex chronic and social concerns, they may struggle with discharge planning and rehabilitation for these patients at a time when the burden of traumatic injuries in the United States continues to rise without a compensatory increase in the general and trauma surgeon workforce.14,22,23
This study builds upon our previous work, highlighting that trauma patients often experience a higher incidence of other medical conditions. 24 For many, trauma admissions represent their first interaction with the health care system, particularly among younger or disadvantaged populations. However, surgeons may not always be the most appropriate primary inpatient providers for patients without immediate surgical needs, particularly for those with complex preexisting conditions or palliative care needs.24-27 Identifying the right transition points to co-management with nonsurgical provider teams and to a trauma team serving in a consulting role during the patient’s hospital course within an institution is crucial for optimizing resource allocation and redesigning care workflows effectively. Critically, our findings do not advocate for complete disengagement from patient care by the trauma team. Rather, we advocate for trauma teams taking a more peripheral or consulting role once all care teams agree that further surgical intervention is unlikely. Our study is the first, to our knowledge, to demonstrate such a transition point. Numerous studies of select nonoperative trauma or isolated injury patients have demonstrated efficacy in management by a non-trauma dedicated service. Crucially, such studies advocate for allocation to non-trauma services after a thorough initial evaluation by a trauma team or in close consultation with a surgical team.28-33
Considering the continued trauma surgeon workforce shortage and increasing proportion of nonoperative trauma patients admitted under the care of a trauma surgeon, attention must turn to minimizing undue inappropriate clinical burden on trauma surgeons who are already susceptible to burnout despite reporting higher rates of perceived patient ownership and a willingness to participate in multidisciplinary care.18,34-39 We believe that our findings show that for every trauma admission, there is a point during admission when the likelihood of requiring surgeon-directed care decreases significantly and plateaus. At this time point, it is reasonable to consider a care transition to a nonsurgical specialist such as a trauma-trained hospitalist, geriatrician, or even supervised advanced practice providers (APPs). Advanced practice provider utilization remains highly variable across different trauma centers. Still, it represents an opportunity for cost-effective care and resource optimization, as APP care has been associated with improved patient outcomes, care continuity, and team cohesion in trauma centers.40-42 For example, one study found that integration of APPs into surgical teams was associated with decreased costs and length of stay for inpatients. 43 Some may argue that taking this approach would weaken the sense of responsibility and patient ownership among trauma surgeons. However, we would counter this by stating that the responsibility of excellent patient care should be shared amongst all health care providers, including APPs and non-surgeons. Moreover, an over-reliance on perceived patient ownership may be associated with burnout and stress among surgeon workforces.18,44
This study has several strengths. We conducted a novel time-to-intervention analysis to identify the optimal timing for transitioning care from surgical to nonsurgical physician or APP leadership. This approach uncovers an opportunity to reevaluate care practices and institutional resource allocation for multidisciplinary trauma patients. Moreover, we examined a diverse patient population representing a range of blunt and penetrating trauma. Penetrating trauma accounted for 7.2% of our patient cohort, which aligns with nationwide rates reported in the literature. 45 Considering the challenges of prolonged hospital stays for trauma patients, the surgeon workforce, high care costs, and the opportunity cost of surgeons attending to patients with non-immediate surgical needs, there is a significant opportunity to redesign trauma care structures to minimize costs while optimizing the delivery of appropriate care to hospitalized patients.
Like all studies, ours has limitations. This study is a single-center retrospective analysis of billable procedures for previously admitted trauma patients. Our conclusions about care transition time points may not match level 1 trauma centers with differing types of trauma populations. However, using clinical time-series analyses to make operational workflow allocation decisions can be replicated at any institution. Another limitation of our study arises from the binary classification of procedures as surgeon-directed or non-surgeon-directed. This classification may simplify complex patient care, and surgeon vs nonsurgical physicians may have differing practice patterns regionally. To mitigate this, procedures were reviewed by a senior general surgery resident and senior surgical faculty member. This analysis can be repeated on an institutional level with procedures recharacterized based on institutional practices or workforce availability.
We also acknowledge several nuances to our findings. Our findings do not support the complete transfer of trauma care, nonoperative or otherwise, to non-trauma services. Trauma surgeons remain the best caregivers for trauma patients in the acute post-trauma period. 46 Our findings, though provocative, should not be generalized to trauma patients admitted to intensive care units, and these patients should remain under the purview of trauma surgeons until it is safe to discharge them to a lower level of care, regardless of length of stay. That said, our findings support a growing trend of multidisciplinary collaboration for trauma patients with increasingly complex comorbidities. One example is geriatric rib fracture and femur fracture patients, who have been shown to benefit from co-management from geriatricians and trauma surgeons. 47 Other nuances exist, such as pancreatic injuries that may require complex pancreaticobiliary repair/reconstruction, altered gastrointestinal anatomy, or complex hepatobiliary trauma. In these cases where patients may require unique multidisciplinary postoperative care, a blanket recommendation to transfer to a medicine service may not be advised.
Conclusion
Using an adjusted model to account for heterogeneity in age, trauma activation level, ISS, GCS, and patient stability, this novel study identifies hospital day 5 as a potential inflection point during a trauma admission at which a nonsurgical physician can drive care, allowing the surgical team to be better utilized elsewhere. While we do not expect time points to be reproducible across all trauma centers in the United States, we highlight that our methodology can help individual centers use local data to tailor local workforce and resource allocation. We do not advocate for entirely shifting the burden of nonoperative trauma care to nonsurgical physicians. Instead, we hope to spur continued efforts to optimize resource allocations in our trauma centers and reinforce multidisciplinary collaboration among surgeons, hospitalists, and APPs. By streamlining trauma care, trauma surgeons can focus on the operative management of injured patients. Our findings continue to emphasize the importance of active engagement with nonsurgical colleagues, case management, and after-hospital care to ensure the most appropriate care for trauma patients in a burdened trauma care system.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: UA receives consulting fees from Siemens Healthineers. AC receives funding from National Institutes of Health Grants #5T32GM008450-25. All JTACS Disclosure forms have been supplied and are provided as supplemental digital content. We acknowledge the editorial assistance of the NC Translational and Clinical Sciences (NC TraCS) Institute, supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Number UM1TR004406.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Appendix
Daily Cox Multivariable Hazard Ratios for Undergoing a Surgeon-Directed Procedure During Admission for Trauma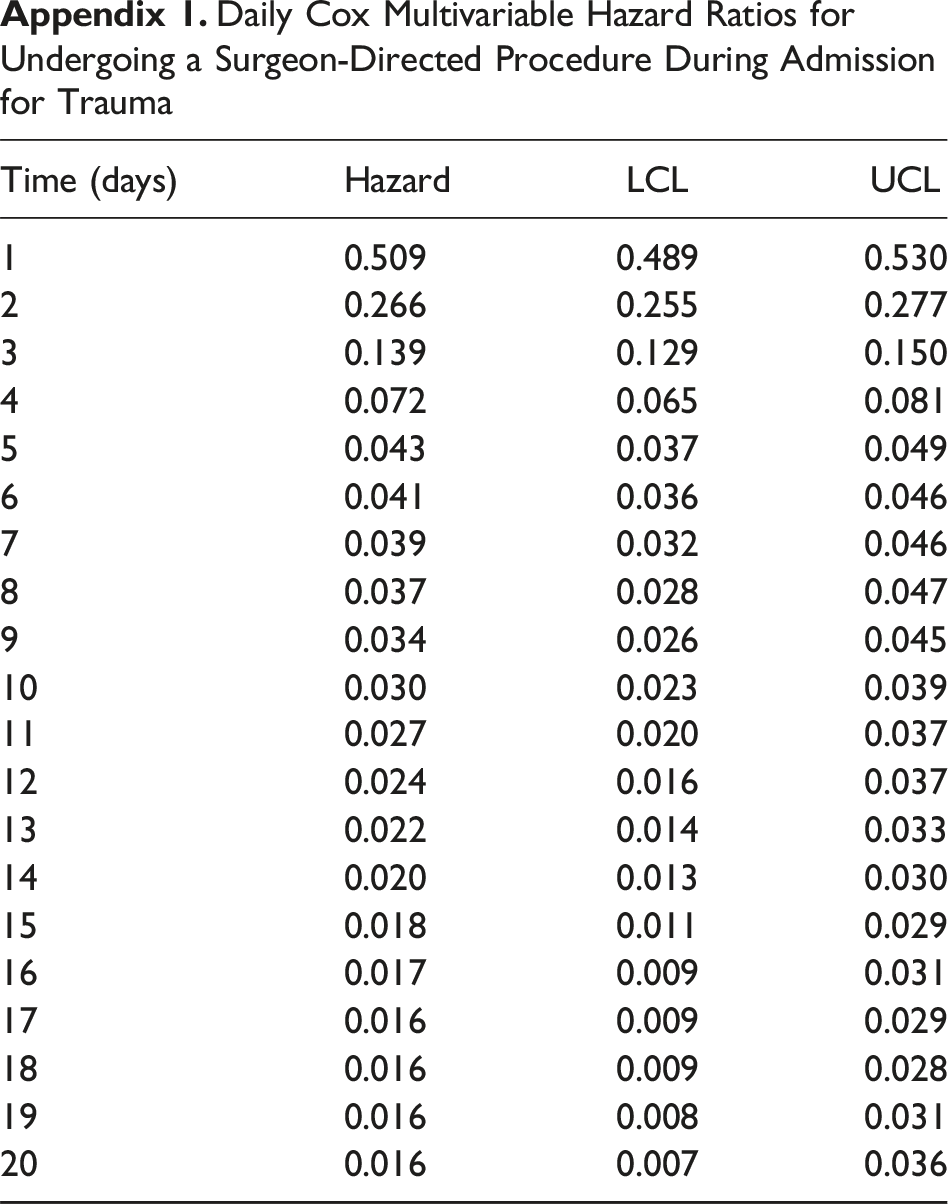
Time (days)
Hazard
LCL
UCL
1
0.509
0.489
0.530
2
0.266
0.255
0.277
3
0.139
0.129
0.150
4
0.072
0.065
0.081
5
0.043
0.037
0.049
6
0.041
0.036
0.046
7
0.039
0.032
0.046
8
0.037
0.028
0.047
9
0.034
0.026
0.045
10
0.030
0.023
0.039
11
0.027
0.020
0.037
12
0.024
0.016
0.037
13
0.022
0.014
0.033
14
0.020
0.013
0.030
15
0.018
0.011
0.029
16
0.017
0.009
0.031
17
0.016
0.009
0.029
18
0.016
0.009
0.028
19
0.016
0.008
0.031
20
0.016
0.007
0.036