
Abstract
Background
Level-I and level-II trauma centers are required to offer equivalent resources since “The Orange Book.” This study evaluates differences between level-I and level-II management of solid organ injury (SOI) with traumatic brain injury (TBI).
Methods
We conducted a retrospective review of the National Trauma Data Banks from 2013 to 2021 of adult (≥18 years), blunt trauma patients with both TBI and SOI treated at level-I or level-II trauma centers.
Results
48,479 TBI and SOI patients were identified, 32,611 (67.3%) at level-I centers. Unadjusted incidence of laparotomy was higher at level I (14.5% vs 11.7%, P < 0.001), and angiography rates were similar (3.3% vs 3.4%, P 0.717). Sub-group analysis of stable patients (SBP ≥100) showed an increase in nonoperative management at level II (87.3% vs 88.7%, P < 0.001) and decrease in laparotomy (9.9% vs 8.3%, P < 0.001). On logistic regression (LR), severe TBI, high-grade SOI, and level I trauma status were predictors of laparotomy. Logistic regression showed mild/moderate TBI with high-grade SOI and level II were associated with use of angiography. Unadjusted mortality rates were slightly different (14.8% vs 13.4%, P < 0.001), but there was no association with trauma level on LR.
Discussion
Nonoperative management was seen more at level-II centers with laparotomy at level I. Subgroup analysis showed no difference in mortality in trauma levels. Matched patients for level I and II showed no statistical difference in management. Patients were treated similarly at both levels with similar outcomes and mortality.
Introduction
The American College of Surgeons Committee on Trauma (ACSCOT) utilizes the “Resources for Optimal Care of the Injured Patient” to determine required resources at different trauma center levels. Trauma centers are categorized into one of 4 levels. Level I trauma centers, as tertiary care facilities, offer comprehensive resources covering the entire spectrum of care from prevention through rehabilitation for traumatic injuries. These centers also engage in extensive education, including public health initiatives, ongoing education for trauma teams, and research in trauma management. Level II trauma centers in contrast provide the full breadth of clinical care for trauma patients but are not required to engage in the same depth of academic pursuits and community-outreach as level-I centers. 1
Since publication of the version of “Resources for Optimal Care of the Injured Patient” or the “Orange Book,” published by the ACSCOT in 2014, and continued in the more recent guidelines the “Gray Book,” resource availability, treatment standards, and outcomes at level-I and level-II trauma centers are required to be equivalent.2,3 In particular, hemorrhage control strategies of both angiography and laparotomy should be equally available and utilized in managing hemorrhagic shock. This is of especial interest in treating poly-trauma patients, such as those with combined traumatic brain injury (TBI) and solid organ injury (SOI). After a severe initial insult, cerebral blood flow autoregulation can be disrupted leading to a cycle of progressive edema, inflammation, and ischemia. 4 One of the mainstays of treatment for TBI is attenuating this potential secondary brain injury (SBI). 5 Hypotension is well-established in the literature to worsen SBI and increase mortality.6-10 In poly-trauma patients with TBI and concomitant injuries, therefore, even the potential for hemorrhagic shock should be aggressively treated.5,11,12 Studies comparing management and outcomes between level I and II trauma centers demonstrate mixed results for different trauma populations.13-21
To our knowledge, no study yet has compared level-I and level-II surgical management (laparoscopy and angiography), resultant outcomes, and mortality in patients with combined TBI and SOI. Other sources of hemorrhage such as open book pelvic fractures or long bone fractures are also important to evaluate alongside TBI. However, management strategies are different. We are specifically interested in evaluating management differences of SOI in the presence of TBI between different trauma levels. This study seeks to evaluate differences between level-I and level-II trauma centers in hemorrhage treatment strategies utilized in patients with TBI and SOI and resultant outcomes. We predict that after the Orange Book, level-I and level-II trauma centers should have similar management strategies in combined TBI and SOI, using angiography or laparoscopy, with laparoscopy being performed more at level I trauma centers. If management strategies are equivalent in level-I and level-II trauma centers, then hospital complications and mortality outcomes should be equivalent as well.
Methods
A retrospective review was conducted of the National Trauma Data Bank (NTDB) from 2013 to 2021. Inclusion criteria included adult patients (age ≥18 years old) treated at either a level-I or level-II trauma center following blunt trauma with diagnosis of both TBI and SOI, specifically any liver, kidney, or spleen injury. Exclusion criteria included interfacility transfers and unidentified trauma level. Patient selection is detailed in Figure 1. Demographic variables such as gender, age, trauma mechanism, Injury Severity Score (ISS), and comorbidities were compared between trauma levels. Patient selection algorithm.
The primary outcome of interest was choice of hemorrhage management strategy: nonoperative vs laparotomy vs angiography. Patients that underwent both laparotomy and angiography were included in the laparotomy group for analysis as these patients made up less than one percent of the study population. The primary outcome also guided the timeframe selected for the study, as variables for angiography and laparotomy as choices for hemorrhage control were introduced in the NTDB in 2013. Secondary outcomes evaluated included mortality, hospital lengths of stay, and hospital events. Sub-group analysis was also conducted for hemodynamically stable patients (ED SBP ≥100) and different grades of TBI and SOI. TBI was separated into mild/moderate TBI defined as Abbreviated Injury Score (AIS) ≤ 3 and Glasgow Coma Score (GCS) ≥ 9 and severe TBI (AIS ≥2 and GCS ≤8). Solid organ injury was separated into low-grade (AIS ≤2), moderate (AIS = 3), and high-grade (AIS ≥4).
Univariate analysis was performed using Pearson’s chi-squared test for categorical variables and independent t-tests for continuous variables. P-values <.05 were considered statistically significant. Multivariate logistic regression analysis was also conducted analyzing influence of trauma verification status and other factors on treatment strategy and mortality. Statistical analysis was conducted using SPSS (version 27.0).
Results
Differences in Combined TBI/SOI Patients Between Trauma Levels.
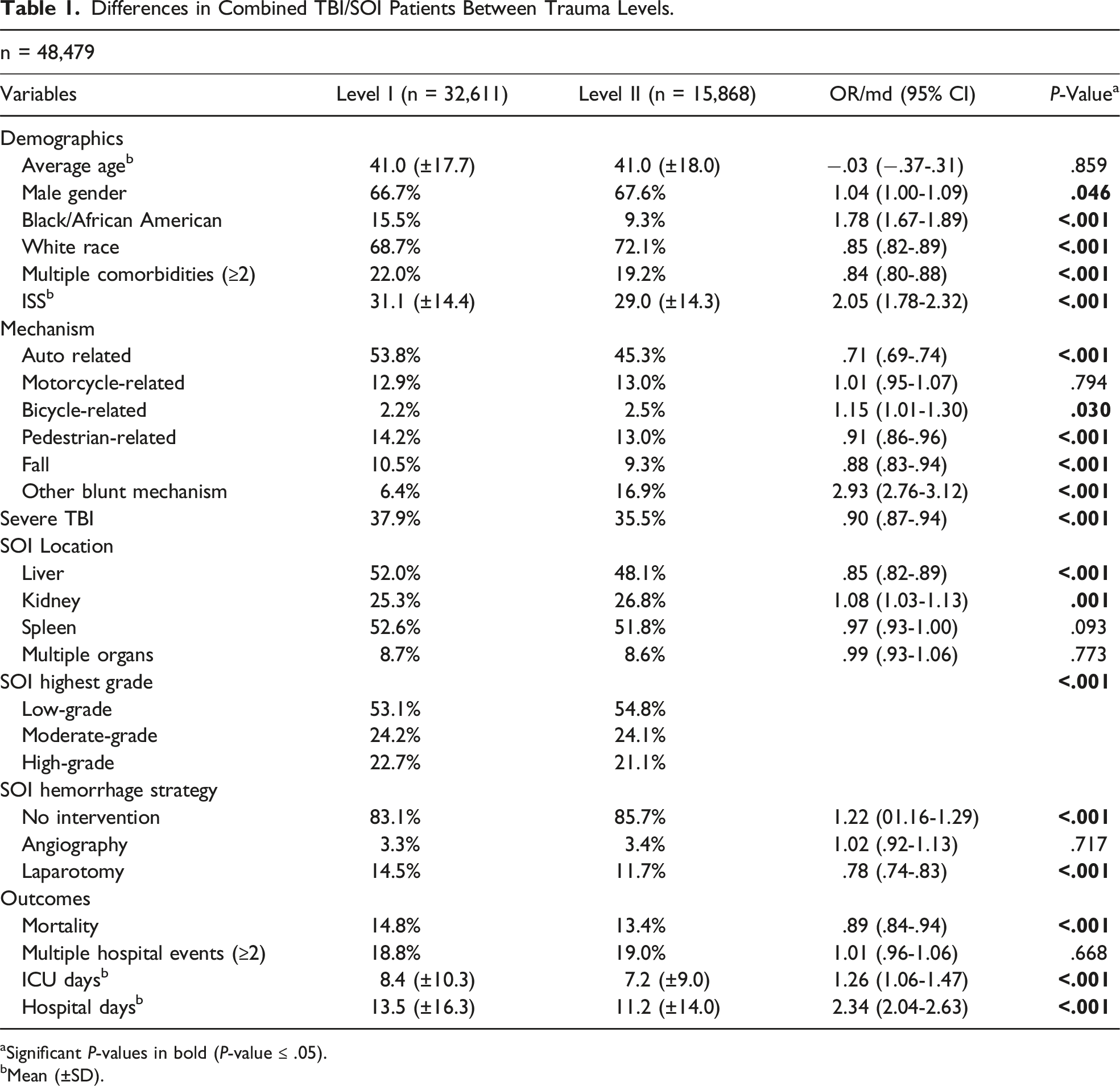
aSignificant P-values in bold (P-value ≤ .05).
bMean (±SD).
Nonoperative management was slightly more frequent at level-II centers (83.1% at level I vs 85.7% at level II, P < .001). Angiography was performed at similar rates (3.3% vs 3.4%, P = .717). Unadjusted incidence of laparotomy, however, was higher at level-I centers (14.5% vs 11.7%, P < .001). Transfusion rates at 4 hours were similar including packed red blood cells (mean volume 319.3 mL ± 3,7772.5 mL at level I vs 315.0 mL ± 1169.6 mL at level II, P = .893), plasma (mean volume 245.8 mL ± 1528.9 mL vs 222.7 mL ± 821.1 mL, P = .138), and platelets (mean volume 43.2 mL ± 622.3 mL vs 43.0 mL ± 190.9 mL, P = .971).
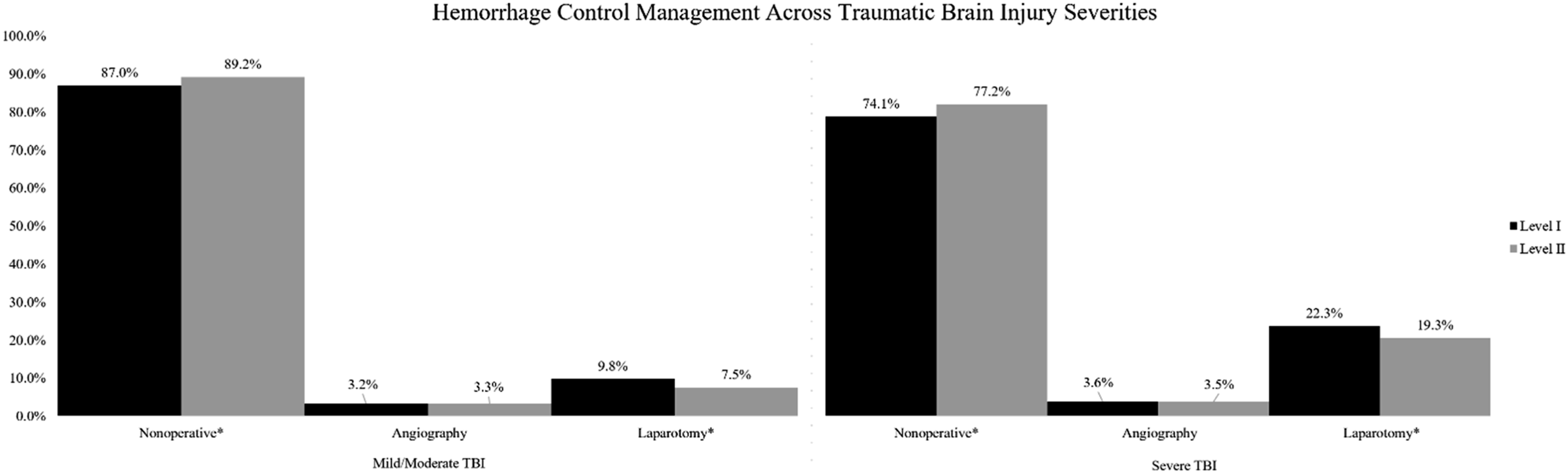
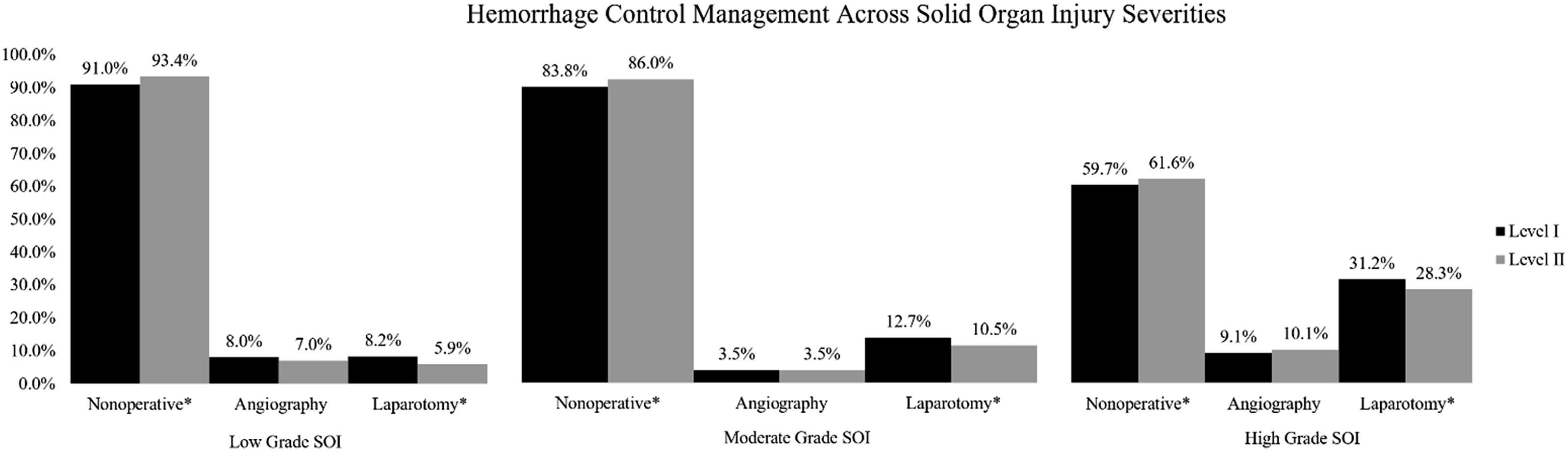
Sub-group analysis of stable patients (systolic blood pressure ≥100) revealed a slight increase in nonoperative management (87.3% at level I vs 88.7% at level II, P < .001) and decrease in use of laparotomy (9.9% at level I vs 8.3% at level II, P < .001) at level-II centers (Graph 1). In patients of different TBI severity, nonoperative management was again more common at level-II centers and laparotomy rates higher at level-I centers (Graph 2). This pattern was also seen on sub-group analysis of different SOI grades (Graph 3). Subgroup analysis: Hemodynamically stable patients. Subgroup analysis: Traumatic brain injury severity. Subgroup analysis: Solid organ injury severity.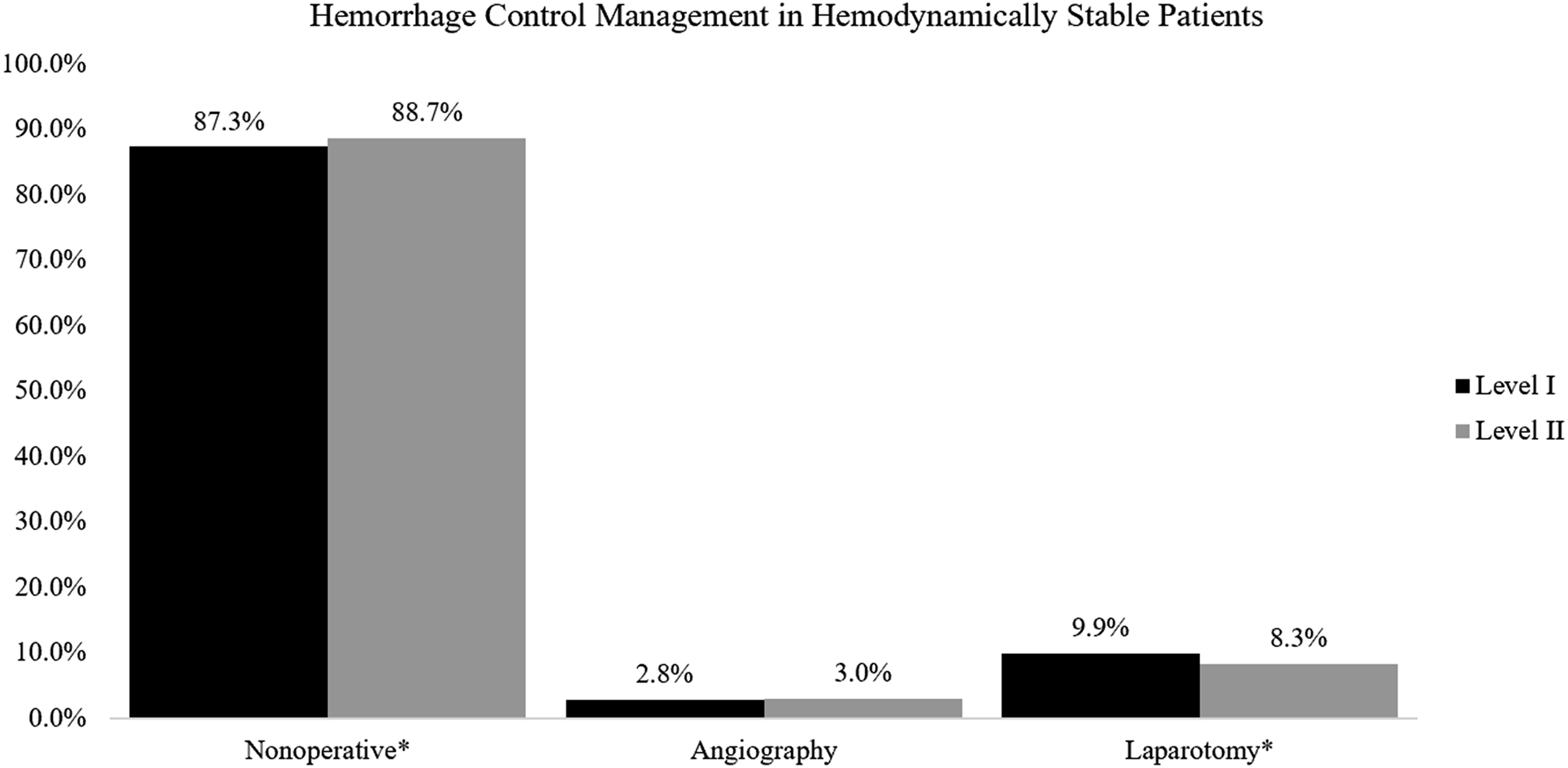
Select Variables in Intervention Logistic Regression.
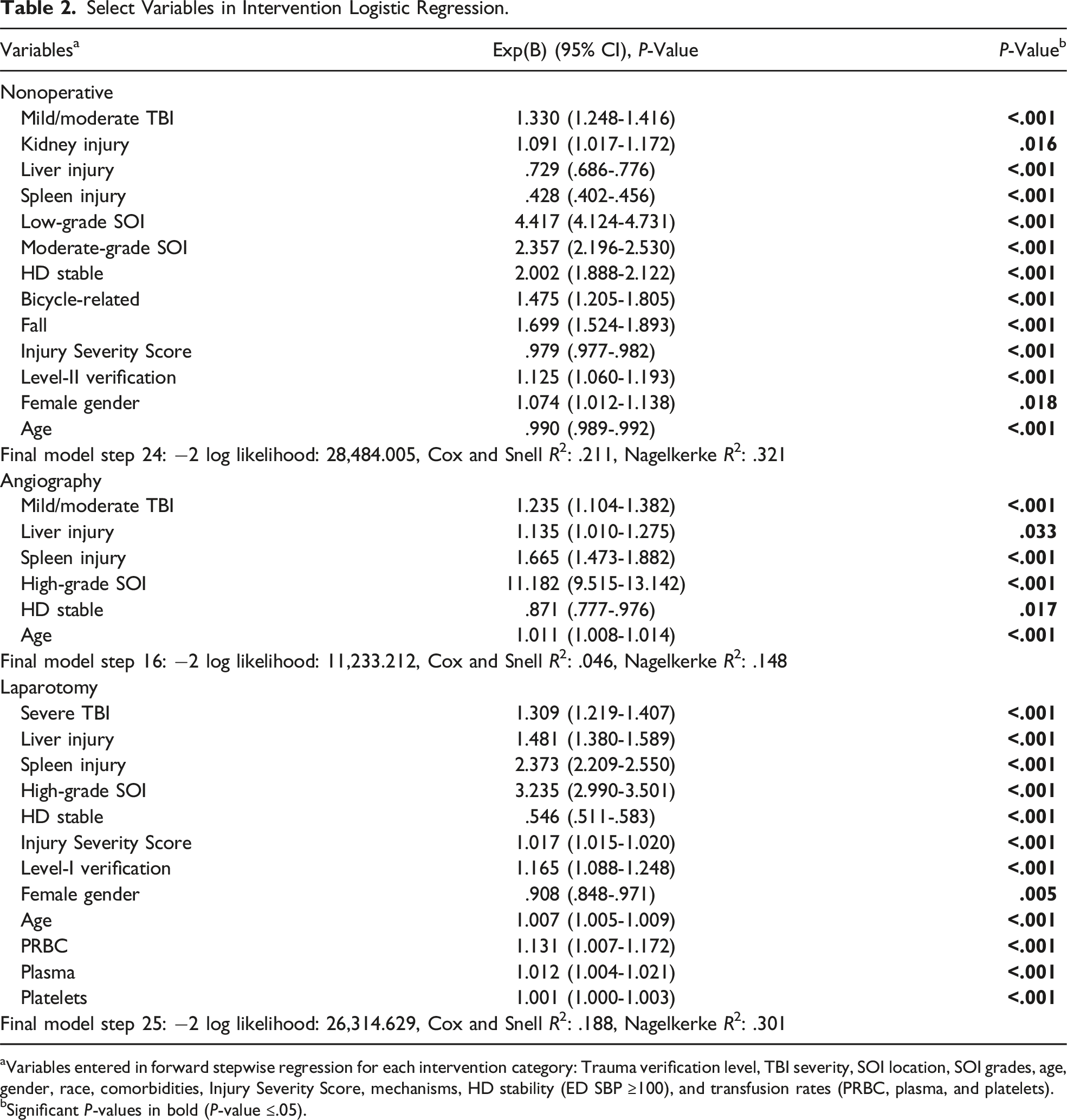
aVariables entered in forward stepwise regression for each intervention category: Trauma verification level, TBI severity, SOI location, SOI grades, age, gender, race, comorbidities, Injury Severity Score, mechanisms, HD stability (ED SBP ≥100), and transfusion rates (PRBC, plasma, and platelets).
bSignificant P-values in bold (P-value ≤.05).
Unadjusted mortality rates were slightly higher at level-I centers (14.8% vs 13.4%, P < .001). On logistic regression, however, mortality was not affected by trauma verification status. Severe TBI, pedestrian-related trauma, falls, increasing age, hemodynamic instability, increasing ISS, and use of laparotomy were all associated with increased mortality. Average ICU and hospital lengths of stay (LOS) were longer at level-I centers on both univariate analysis and linear regression (ICU adjusted estimate .68, P < .001; hospital adjusted estimate 1.69, P < .001). Complications such as sepsis (.9% vs .6%, P .001), acute kidney injury (2.7% vs 2.3%, P .008), pulmonary embolism (1.8% vs .9%, P < .001), and pneumonia (4.7% vs 3.6%, P < .001) were all mildly increased at level-I centers on univariate analysis but were not affected by verification status on logistic regression.
Discussion
This study supports the notion that level-I and level-II trauma centers perform equivalently. While we did note minor variations in treatment strategies between verification level, on further analysis this did not appear to be independently associated with trauma level but rather related to patient-specific characteristics. Despite these minor differences, we found no significant difference in either mortality or hospital complications between patients with concomitant TBI and SOI managed at either level-I or level-II trauma centers. One study in 2009, prior to the Orange Book changes, focused on transport from scene to level-I hospitals and analyzed survival and functional outcomes based on discharge status. 13 The study’s results showed that patients taken directly to level-I trauma centers from the scene of injury have improved survival and better functional outcomes. Significant results were noted in patients with head injuries or pelvic fractures. 13 Level-I centers were more likely to discharge home, rehabilitation, or SNF than patients taken directly to level-II trauma centers. 13 Because the study was performed prior to the changes in the Orange Book, it’s expected that a level-I trauma center would indeed have better outcomes and survival. The reasons of better outcome and survival benefit trace back to level-I centers have more resources, higher volume, higher acuity, and a training institution. 13
Our study adds to the growing body of literature showing similar outcomes between level-I and level-II trauma centers. Unadjusted mortality was slightly higher at level-I centers, which can be explained by the sicker (more patients with multiple comorbidities) and more severely injured (higher ISS) patients that presented to level-I centers. However, there was no association with trauma-level designation with mortality on logistic regression. Interestingly, lengths of hospital and ICU stays as well as unadjusted rates of certain hospital complications were also noted to be increased at level-I centers, again possibly explained by the higher acuity of trauma patients at level-I centers. A systematic literature study performed in Denmark compared mortality or nonfatal outcomes in level-I trauma level to non-level I with populations that had general trauma or major trauma using six electronic databases up to December 2019. Though the study adjusted for comorbidity and interhospital transfer “less frequently,” 21 it still found that level-I centers reported survival benefit and were associated with lower mortality than non-level-I trauma centers. This study cited similar reasons as the 2009 study discussed above for survival benefit and lower mortality due to higher volume of patients resulting in more experience managing these patients and/or more resources available at level-I centers especially because “level-I centers serve as the regional resource center and training institution in their area.”13,21
Some differences were noted in management choices when comparing level-I and level-II centers. Nonoperative management was more commonly pursued at level-II centers and laparotomy occurred more frequently at level-I centers. This trend was continued on sub-group analysis of both hemodynamically stable patients and across different severities of both TBI and SOI. The association of level-II status with nonoperative management and level-I status with laparotomy was also found on logistic regression analysis. When looking at past studies analyzing verification centers and management strategies, it is important to note the limited studies available after the revised Orange Book. A study looked at data of trauma patients from January 2011 to December 2016 extracted from the Michigan Trauma Quality Improvement Program (MTQIP) database, which has 29 ACS-COT-verified level-I and level-II trauma centers in that state. 22 The study showed that differences do exist in outcomes between level-I and level-II trauma centers for severe liver injury. Level-II centers were more likely to use angiography in higher grade liver injuries and more likely to use operative management with “concomitant hollow viscus, splenic, bladder, or abdominal vascular injuries” with no significant difference seen in patients. 22 Comparing the study’s results to past studies, the improved outcomes found at level-I centers still exist for severe liver injuries, head injuries, and major injuries ISS >15 despite the expectation of level-I and level-II trauma centers to have clinically equivalent resources and outcomes based on the Orange Book. 22 In addition to level-I centers having a higher volume, possible factors that may contribute to varying outcomes between level-I and level-II centers include the center having a surgical residency program, medical school association, trauma research, surgical critical care services, and more experienced personnel. 22
Management Following Matching.
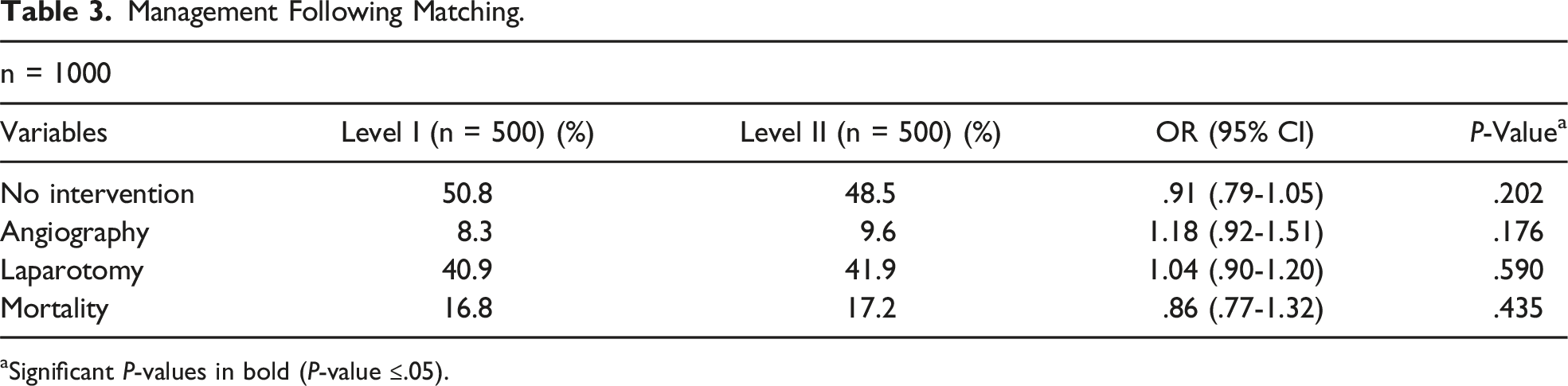
aSignificant P-values in bold (P-value ≤.05).
This study has limitations, mainly that of being a retrospective review. Given the large sample size, statistical significance does not necessarily equate to clinical significance. We defined TBI severity using a combination of AIS and GCS, attempting to differentiate TBI severity in a clinically relevant manner. However, we are unable to account for loss of consciousness or other nuances of TBI. Categorization of SOI grade is more conventional. 23 The database of use (NTDB) also inherently carries certain limitations including the inability to differentiate between patients with multiple traumatic encounters included in the data set due to de-identification, detail of more specific TBI-related morbidity, and capture of long-term outcomes beyond the hospital stay.
Although our study shows equivalent mortality outcomes and hospital complications in level-I and level-II trauma centers, further studies are needed to establish the equality care of this patient population more definitively between both levels of trauma verification. This study may not be generalizable due to varying definitions and categorization of SOI grade, definition, and grading of TBI severity, whether outpatient/inpatient management of comorbidities preinjury affected resulting outcomes, and type of patient population presenting to level-I vs level-II trauma centers.
Supplemental Material
Supplemental Material - Impact of Trauma Verification Level on Management and Outcomes of Combined Traumatic Brain and Solid Organ Injuries: An NTDB Retrospective Review
Supplemental Material for Impact of Trauma Verification Level on Management and Outcomes of Combined Traumatic Brain and Solid Organ Injuries: An NTDB Retrospective Review by Ayesha Tariq, Bhani Kondal, MD, Elliott Smith, MD, Emily Dubina, MD, Nicholas Sheets, MD, and David Plurad in The American Surgeon.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.