
Abstract
Introduction
Traditionally peritoneal dialysis (PD) is initiated >3 weeks post-placement for tract maturation. The pandemic spurred a need for earlier initiation. We hypothesized that there is no significant difference between outcomes of early start (<2 weeks) vs standard (>2 weeks).
Methods
A retrospective review was conducted between 2020 to 2022 at a safety-net hospital and included patients who received a PD catheter (“PDC”). Demographics, technique, dialysate volume, and outcomes were analyzed.
Results
83 patients met criteria. 47/83 (56.6%) were male, the average age was 49.9 [41-60] years, and average BMI was 30.7 [26-34.6]. Average dialysate volume was 2.13 L (±1.31). There were no significant differences in readmissions, reoperations, or catheter issues between the two groups. Patients with higher BMI and catheter-related issues were more likely to be readmitted (P = 0.0003) and undergo reoperation (P = 0.0021).
Conclusions
Early initiation of PD was not associated with significant differences in complications compared to standard start. Our study demonstrates the feasibility and safety of early PD initiation.
Background
Nearly 1 million people in the United States suffer from end-stage renal disease, currently defined as an estimated glomerular filtration rate of 20-30 mL/min/1.73 m2. More than a half a million of these patients require some form of dialysis with half of these patients undergoing kidney transplant. 1 Unfortunately, many patients do not or will not meet criteria for kidney transplant and thus receive dialysis in the form of hemodialysis (HD) or peritoneal dialysis (PD) with many patients requiring HD or PD as they wait for a donor match. 2 Peritoneal dialysis is typically initiated 2-4 weeks after placement of the catheter to minimize complications associated with catheter dysfunction and infection. However, there is decreased use of earlier initiation of PD given anecdotal concerns about infection and leaking around the catheter site while it matures. The timing of urgent peritoneal dialysis initiation varies in the literature, with some defining it as two weeks while others defining it as less than 72 hours.3,4 Recent studies suggest that PD can be started earlier with comparable risks to standard initiation.5-8 In fact, some studies have found there are lower complication rates in urgent-start PD catheters when compared to urgent-start HD catheters.9,10
During the COVID pandemic, capacity restrictions in our hospital/outpatient settings led to consideration of starting patients on PD earlier than 2 weeks to continue to meet patient needs. In this retrospective review, we hypothesized that earlier initiation of peritoneal dialysis after catheter placement is not associated with increased complications. Our secondary outcome was to evaluate the impact of technique (pexy of the omentum, lysis of adhesions, and pexy of the catheter or none).
Methods
We performed a retrospective chart review at our tertiary, safety-net hospital between January 2020 and January 2022 and included all patients who underwent peritoneal dialysis catheter placement. Patients who underwent replacement of peritoneal dialysis catheters, underwent PDC at an external facility, and those whom we could not verify PD initiation were excluded (Figure 1). This study was approved by the University of Texas Southwestern Medical Center and Parkland Health and Hospital System Institutional Review Boards and adheres to the principles and procedures in accordance with the ethical standards of our IRB and with the Helsinki Declaration of 1975. Informed consent was waived due to the retrospective nature of this de-identified study. Inclusion Criteria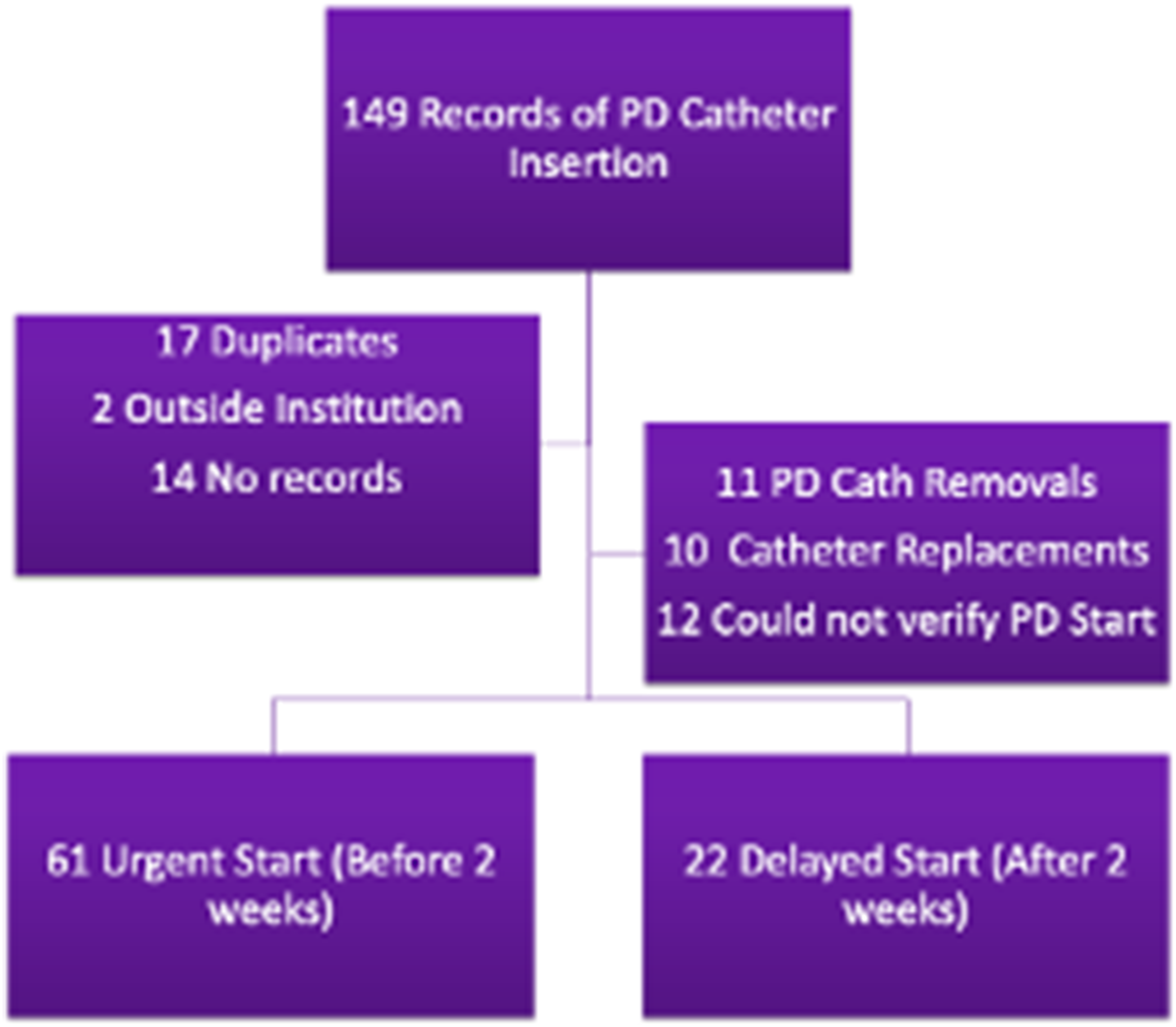
Technique
Peritoneal dialysis catheters were placed laparoscopically in the OR with general anesthesia and preoperative antibiotics, typically renally dosed cefazolin barring a penicillin allergy in which case clindamycin is typically administered. Peritoneal dialysis catheter insertion typically involved Veress placement and insufflation in the LUQ or peri-umbilical space, followed by a supraumbilical incision and the placement of the catheter via Seldinger technique and dilation. Lysis of adhesions, omentectomy, omentopexy, or fixation of the catheter with a dissolvable suture in the lower midline were performed at the discretion of the surgeon. The catheter was then tunneled from midline to either the right or left of the umbilicus. Administration of a heparin-lock through the catheter was also performed at the discretion of the surgeon and used sparingly. After the postoperative period, the patient would receive follow-up from an outpatient dialysis facility that would provide additional home training for peritoneal dialysis. Dialysate volume was measured in liters and recorded by the dialysis nurse; these amounts were recorded in and extracted from the patient’s progress notes. The first recorded dialysate volume was captured for each patient.
Demographics and Outcomes
We collected demographic data including age, sex, comorbidities, ASA score, and BMI. Variables related specifically to the catheter included date of operation, type of technique used during the operation, and whether PD initiation was early vs standard.
We defined PD dialysis initiation less than 2 weeks from surgery as “early” in line with prior studies. The primary outcome was catheter complications including kinking, clogging, and infection. Secondary outcomes included readmissions and need for reoperation. Categorical variables (eg, sex and comorbidities) were analyzed with chi-square tests. Continuous variables (eg, age) were analyzed using Mann-Whitney U tests. All data were analyzed with a P-value of < 0.05.
Results
Demographics
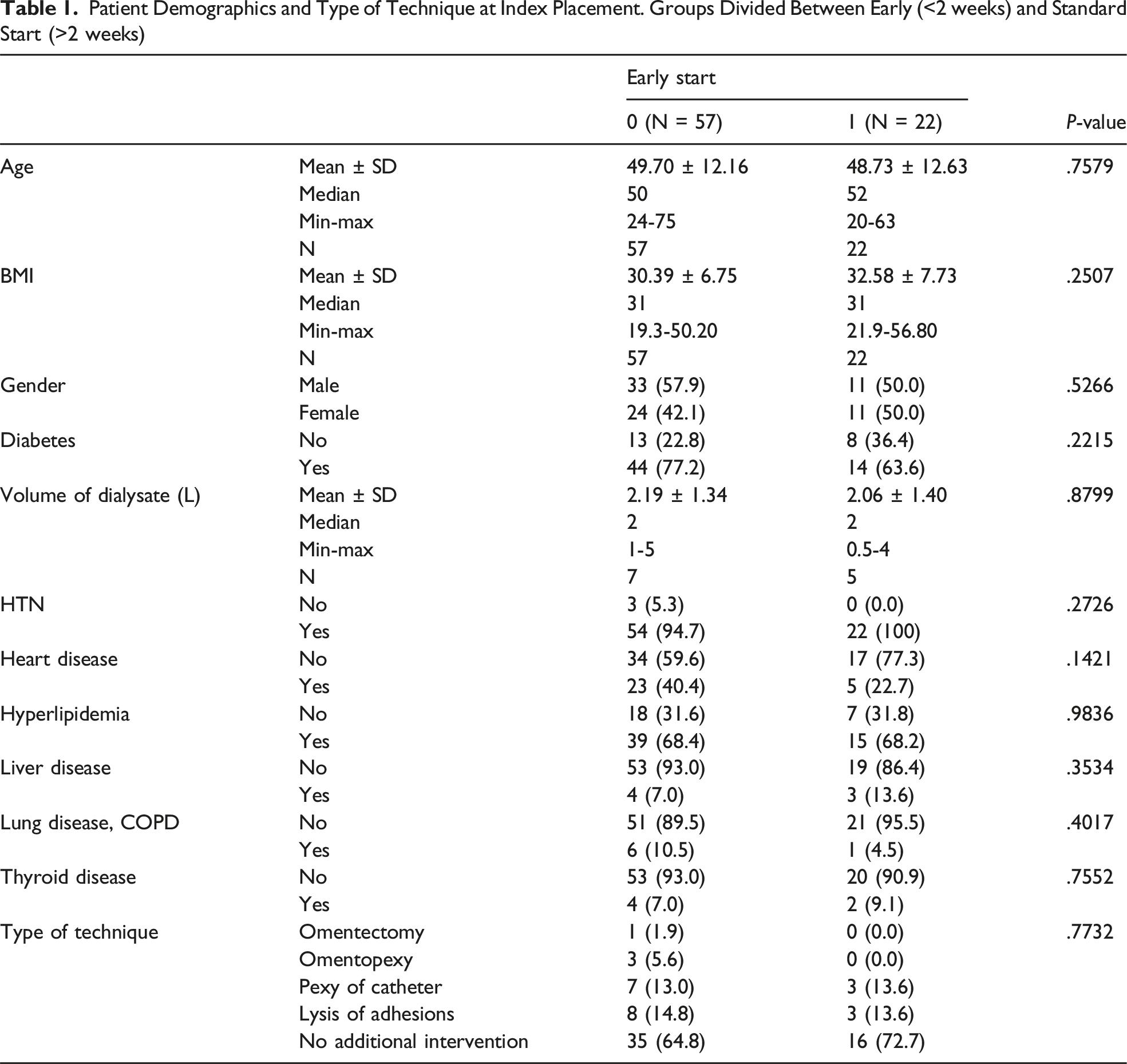
Patient Demographics and Type of Technique at Index Placement. Groups Divided Between Early (<2 weeks) and Standard Start (>2 weeks)
Readmission and Reoperation
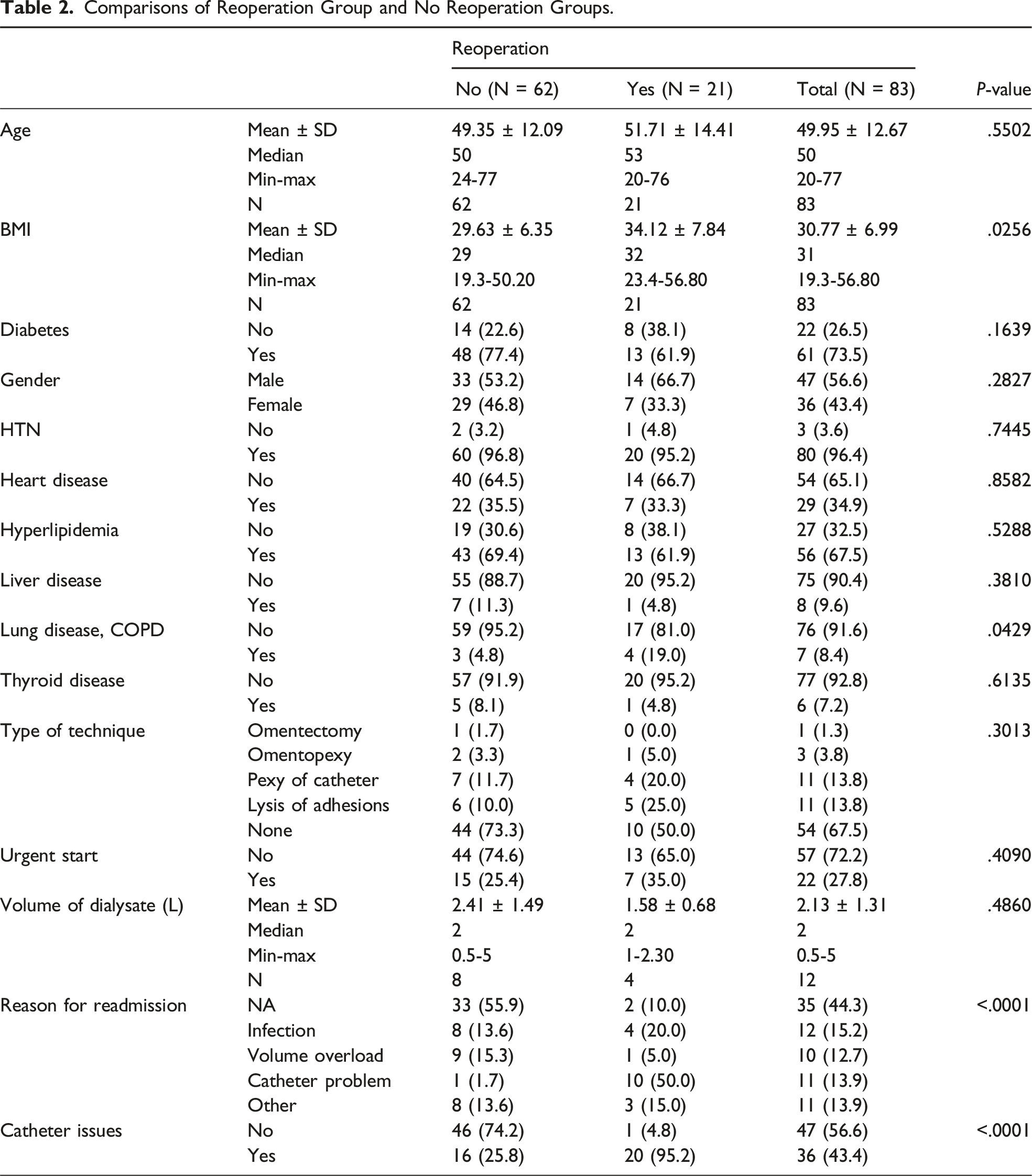
Comparisons of Reoperation Group and No Reoperation Groups.
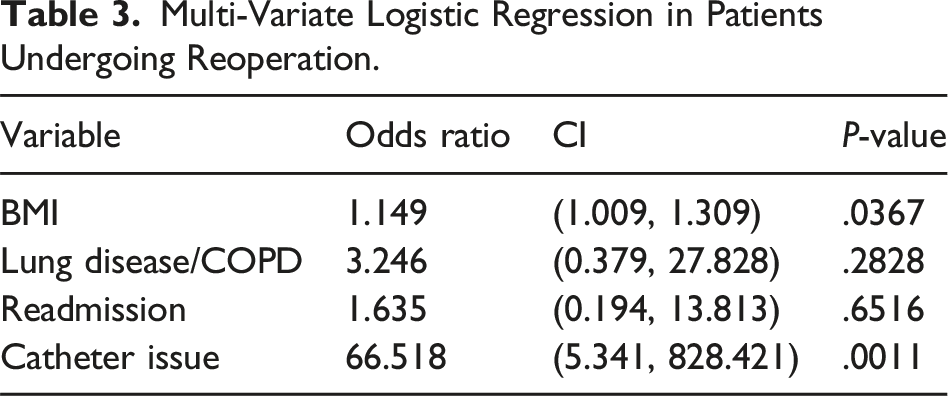
Multi-Variate Logistic Regression in Patients Undergoing Reoperation.
Impact of Technique or Dialysate Volume
No associations were found between techniques or volume of first dialysate. Though if a prophylactic technique was done, most surgeons performed lysis of adhesions or catheter-pexy. The mean volume of first dialysis session via PD catheter in the early start group was 2.06 L and 2.19 L in the standard start group (Table 1). There were no significant differences in the primary outcome (catheter issues) or secondary outcomes (reoperations (P = .4090) and readmissions (P = .8183)) (Tables 2 and 3).
Discussion
In this single-center retrospective review, we explored the outcomes of patients undergoing peritoneal dialysis catheter placement peri-pandemic and its associated challenges with constrained resources. While many studies have shown benefits of urgent initiation of dialysis, many institutions (our own included) at the time did not have a standardized protocol in place for early-start peritoneal dialysis given a historical standard start at 4-8 weeks post-placement to allow for tract maturation.
Hemodialysis and PD have been found to have comparable short-term and long-term outcomes; however, there remain barriers to PD initiation and implementation. Patients can often struggle with PD dialysis since there is a large burden of responsibility on the patient/caregiver requiring education and equipment/supplies setup. 11 Additionally, hospitals may lack the proper protocol for early-start PD catheters, since most emergent protocols for dialysis are centered around hemodialysis. Some hospitals have attempted to develop protocols for urgent or early PD, but many programs are still early in development with findings similar to ours in successful early PD initiation.12-14
The results of this small single-center study demonstrate the efficacy of early-start peritoneal dialysis during the pandemic with no increased risk of catheter-related issues. While a higher percentage of individuals who initiated earlier did have issues with their catheters (55.45% vs 42.59%), this was not found to be statistically significant (P = .2459), which is consistent with the available literature.
There were some differences with regards to the type of catheter complications experienced between our groups and what was seen in other studies.3,15 The most common PDC complication in our study was mechanical dysfunction (kinking, clogging, leaking, etc.) regardless of initiation timing. In our cohort, catheter dysfunction was not the most common complication in our cohort, occurring in only 22.73% of patients. The most common complication was infection (27.73%) with the majority consisting of superficial infections that required antibiotic therapy without surgical intervention. This difference could be attributed to a small sample size or our patient population.
Notably, mechanical dysfunction is more common in unplanned PD initiation.3,15,16 Several studies have stated that these mechanical issues can result in the need for further operative management 17 which was consistent with our experience. Worse outcomes in patients undergoing PDC and PD, whether urgent or standard start, have been associated with comorbid conditions with the most common being diabetes.17,18 However, the opposite was true in the case of our study where patients with diabetes had a negative relationship with catheter issues. We suspect this is likely related to small sample size.
Limitations
This study was not without limitations. It is a retrospective single-centered study with a limited sample population. Given that it is a retrospective study, there is poor control over covariates and potential confounding factors, and it is more likely to be affected by bias than prospective studies. Additionally, other important factors like socioeconomic status, access to care, and education/comfort with peritoneal dialysis were not considered for this study. While surgical placement of the PD catheter is a necessary step, there are many other factors in beginning home PD dialysis, including equipment/supplies set up and patient education that this study did not address. Furthermore, patient education can be impacted by language barriers within our population. Given that a significant percentage of our patient population speaks Spanish, the additional obstacle to educating on peritoneal dialysis (which is heavily patient-dependent) should also be further investigated. Thus, multidisciplinary support is crucial for developing and implementing urgent start PD dialysis protocols.
Finally, one other limitation of the study was that many participants had their dialysis done at outside facility rather than part of our health system so while dialysis start dates were recorded—at the time—a standardized process for time from catheter insertion to nurse teaching to first dialysis was not yet implemented. Additionally, because some facilities did not use the same electronic medical record, the volume for the first dialysis session was not always available for each patient.
Conclusion
Patients with ESRD should be evaluated for the possibility of dialysis and transplant in order to adequately create a “life plan” for how they want to pursue treatment.2,19 However, this is not a possibility for patients with rapid decline in kidney function or patients presenting acutely with severe ESRD. While HD catheters are traditionally used in the urgent setting, the lifestyle advantages and lower complication rates associated with PD catheters make it an attractive option for patients in the short-term and long-term setting. Our study has demonstrated that PD catheters can be safely placed and accessed in less than 2 weeks with similar complication rates to standard dialysis start times. We hope this will aid hospitals in developing urgent start PD protocols and increase access to PD dialysis for appropriate patients.
Footnotes
Author Note
This work was presented at the 2023 Annual Clinical Congress of the American College of Surgeons.
Author Contributions
Literature review: Caleb Graham, Kelsey Melinosky, Jalen Harvey and Caroline Park. Study design: Susan Hambrick and Caroline Park. Data extraction and analysis: Caleb Graham, Kelsey Melinosky, Lauren Lym, Jessica McConahey, Heba Zakaria, Bing Chun Wan, and Caroline Park. Writing and critical revisions: Caleb Graham, Kelsey Melinosky, Thomas Shoultz, Stephen Luk, Jalen Harvey and Caroline Park.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.