
Abstract
Background
While greater institutional experience with high-risk rectal cancer operations has previously been associated with improved clinical outcomes, the impact on costs remains unclear. The present work aimed to characterize the relationship between hospital proctectomy volume and hospitalization costs.
Methods
The 2016-2021 Nationwide Readmissions Database was queried to identify all adults undergoing elective rectal cancer resection. Multivariable linear regression was used to model hospitalization costs, with inclusion of hospital volume as restricted cubic splines. The volume corresponding to the inflection point (60 cases) was used to categorize hospitals as high-volume (HVH) or low-volume (LVH). Association of HVH status with adverse events, resource use, and readmission was assessed.
Results
An estimated 123,231 patients underwent rectal cancer resection, with median cost of $24,700. Although only 22.1% of hospitals were defined as HVH, 65.3% of patients were treated at these centers. Compared to LVH, patients at HVH were more commonly privately insured and had neoadjuvant chemoradiation and robotic operations. After adjustment, HVH was associated with lower odds of complications (AOR 0.91, P = 0.001) and non-home discharge (AOR 0.86, P < 0.001), while mortality and 30-day readmission were comparable. Furthermore, HVH was associated with a -$1800 decrement in costs (P < 0.001) and a −0.6-day decrease in length of stay (P < 0.001). Of note, the disparity in costs between HVH and LVH persisted over time.
Discussion
Increasing institutional volume of rectal cancer resection was associated with reduced hospitalization costs. Further cost mitigation strategies to streamline care pathways at low-volume centers are warranted to improve the value of rectal surgical care.
• Using the 2016 to 2021 Nationwide Readmissions Database, increasing hospital volume of rectal cancer resection was associated with reduced hospitalization costs. • Hospitals with high volume of rectal cancer resection were associated with a -$1800 decrease in costs, −0.6-day decrease in length of stay, and 9% lower odds of complications compared to low-volume hospitals.Key Takeaways
Introduction
Colorectal cancer is the second leading cause of cancer-related deaths globally, with rectal cancer accounting for 30% of diagnoses and 46,000 new cases in the United States each year. 1 Surgical resection, in combination with chemoradiation, remains the gold standard treatment for rectal cancer. 2 However, rectal operations can be technically challenging due to the narrow anatomy of the pelvis and difficulty to achieve adequate resection margins. Growing literature suggests that greater surgeon and hospital volume may be associated with improved outcomes following complex oncologic surgery. 3 Moreover, efforts to centralize rectal cancer care to high-volume centers of excellence have demonstrated improved recurrence-free and overall postoperative survival. 4
Although regionalization of rectal surgical care may have clinical benefits, the financial implications have not been well-studied. High-volume centers may accrue lower hospitalization costs due to greater surgeon experience, efficient care pathways, and avoidance of costly complications. 5 On the other hand, major referral centers may require significant travel distance and increased resource utilization in order to deliver higher quality care. 6 Nevertheless, a recent multi-center study suggested that rectal cancer surgery performed at a high-volume regional center rather than the closest hospital available was both less expensive and contributed to greater long-term quality-adjusted life years. 7 Yet the cost-volume relationship in rectal surgery at the national level has not been explored. Understanding the financial outcomes of care at high-volume hospitals across various regional referral patterns may inform value-based surgical care.
The present study used a nationally representative cohort to characterize the relationship between hospital volume of elective rectal cancer resection and inpatient costs. In addition, we examined the association of volume status with patient factors and clinical outcomes. We hypothesized that increasing hospital volume would be associated with reduced costs, and high-volume centers would exhibit lower mortality, complications, length of stay, and 30-day readmission.
Methods
Data Source and Study Population
This was a retrospective cohort study using the 2016-2021 Nationwide Readmissions Database (NRD). Maintained by the Healthcare Cost and Utilization Project, the NRD is the largest all-payer readmissions database in the United States. 8 Using validated survey-weighting methodology, the NRD provides accurate estimates for over 33 million discharges and approximately 60% of all US hospitalizations. Unique linkage numbers are used to track hospital readmissions within each state and calendar year. Due to the de-identified nature of the NRD, this study was deemed exempt from full review by the Institutional Review Board at the University of California, Los Angeles. All adults (≥18 years) undergoing elective resection for rectal cancer were identified using International Classification of Diseases, 10th Revision (ICD-10) procedure codes (Supplemental Table 1). Records with missing data for age, sex, mortality, or admission type were excluded.
Study Variables and Outcomes
Patient and hospital characteristics including age, sex, income quartile, primary payer, and hospital teaching status were defined in accordance with the NRD Data Dictionary. 8 Comorbidities such as diabetes, hypertension, obesity, coronary artery disease, chronic lung, liver, and kidney disease, as well as history of chemoradiation therapy were identified using ICD-10 diagnosis codes (Supplemental Table 1). The Elixhauser Comorbidity Index, a validated composite of 30 comorbidities, was used to quantify the overall burden of chronic conditions. 9 Treatment characteristics, including operative approach (open, laparoscopic, and robotic), type of resection (low anterior resection (LAR), abdominoperineal resection (APR), and stoma creation were defined using ICD-10 procedure codes (Supplemental Table 1). Similarly, complications including renal (acute kidney injury), infectious (sepsis and wound infection), respiratory (pneumonia, mechanical ventilation, and respiratory failure), cardiac (cardiac arrest and tamponade), thromboembolic (deep vein thrombosis and pulmonary embolism), cerebrovascular (stroke), and hemorrhagic complications as well as ileus were identified (Supplemental Table 1). Annual hospital volume was calculated as the total number of rectal cancer resections performed at each institution in a given year.
Multivariable linear regression was used to model hospitalization costs. Patient factors were selected for inclusion as covariates by applying autonomous variable selection methods as detailed below. Hospital volume was treated as a continuous variable and incorporated into the model using restricted cubic splines. Using the postrcspline package in Stata, restricted cubic splines allow for nonlinear estimation of the functional relationship between volume and costs. 10 The inflection point of the spline between hospital volume and costs was then defined as the global maximum of the second derivative. 10 Hospitals at or above the volume corresponding to the inflection point (60 cases) were considered high-volume (HVH) and others low-volume (LVH).
The primary outcome of interest was hospitalization costs, which were generated by applying center-specific cost-to-charge ratios to overall charges and inflation-adjusted using the 2021 Personal Healthcare Price Index. 11 Mortality, complications, length of stay (LOS), non-home discharge, and 30-day nonelective readmission were secondarily assessed.
Statistical Analysis
Categorical and continuous variables are reported as proportions (%) or medians with interquartile range (IQR) and compared using the Pearson’s chi-square or Mann-Whitney U tests, respectively. Multivariable linear and logistic regressions were developed to evaluate the association between HVH status and outcomes of interest. Variable selection for all models was performed by applying the Least Absolute Shrinkage and Selection Operator (LASSO) regularization algorithm to reduce the risk of model overfitting and enhance out-of-sample generalizability. 12 An interaction term between the admission year and HVH status was used to analyze cost differences over time. Regression results are reported as adjusted odds ratios (AORs) or beta coefficients (β) with 95% confidence intervals (95% CIs). Statistical significance was set at α = 0.05. All statistical analyses were performed using Stata 16.1 (StataCorp, College Station, TX).
Results
Estimating the Cost-Volume Relationship
A nationally representative sample of 123,231 patients underwent elective rectal cancer resection, with a median cost of $24,700 (IQR: 17,800-35,900). Of 508 NRD-participating hospitals, the median annual institutional volume of rectal cancer resection was 17 (IQR: 5-47) cases per year (Figure 1). Histogram of annual hospital caseload of rectal cancer resection.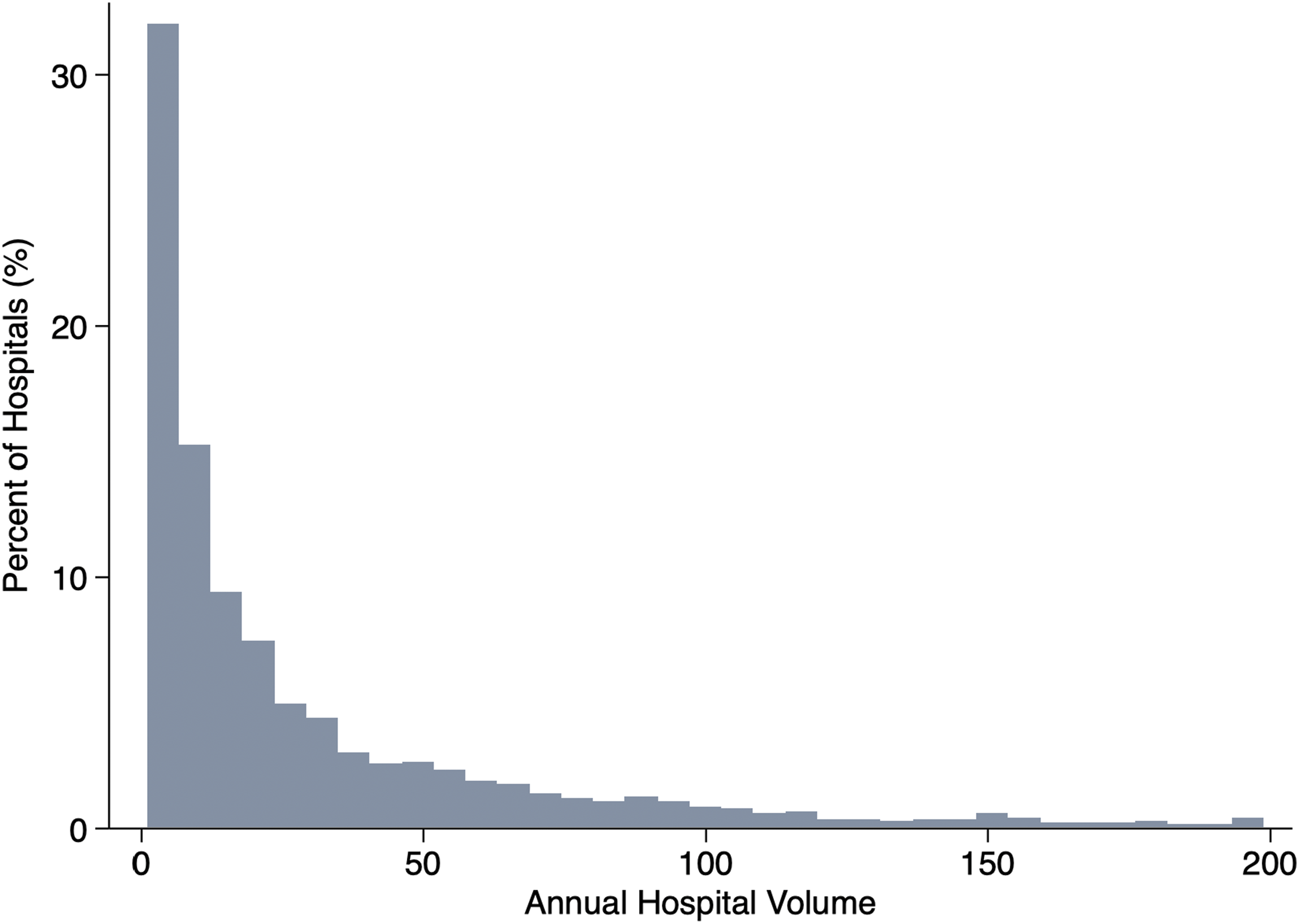
After risk adjustment, several patient characteristics, such as increasing Elixhauser Comorbidity Index, were associated with greater hospitalization costs (Supplemental Table 2). History of chemoradiation therapy was associated a -$600 decrease in expenditure. In addition, robotic operative approach, APR compared to LAR, and stoma creation were all associated with significantly increased costs. Figure 2 displays the volume-cost relationship among all hospitals performing rectal cancer resection. The minimum volume threshold was identified at 60 cases per year, and 22.1% of hospitals were designated as HVH. Functional relationship between annual hospital volume of rectal cancer resection and hospitalization costs using restricted cubic spline analysis.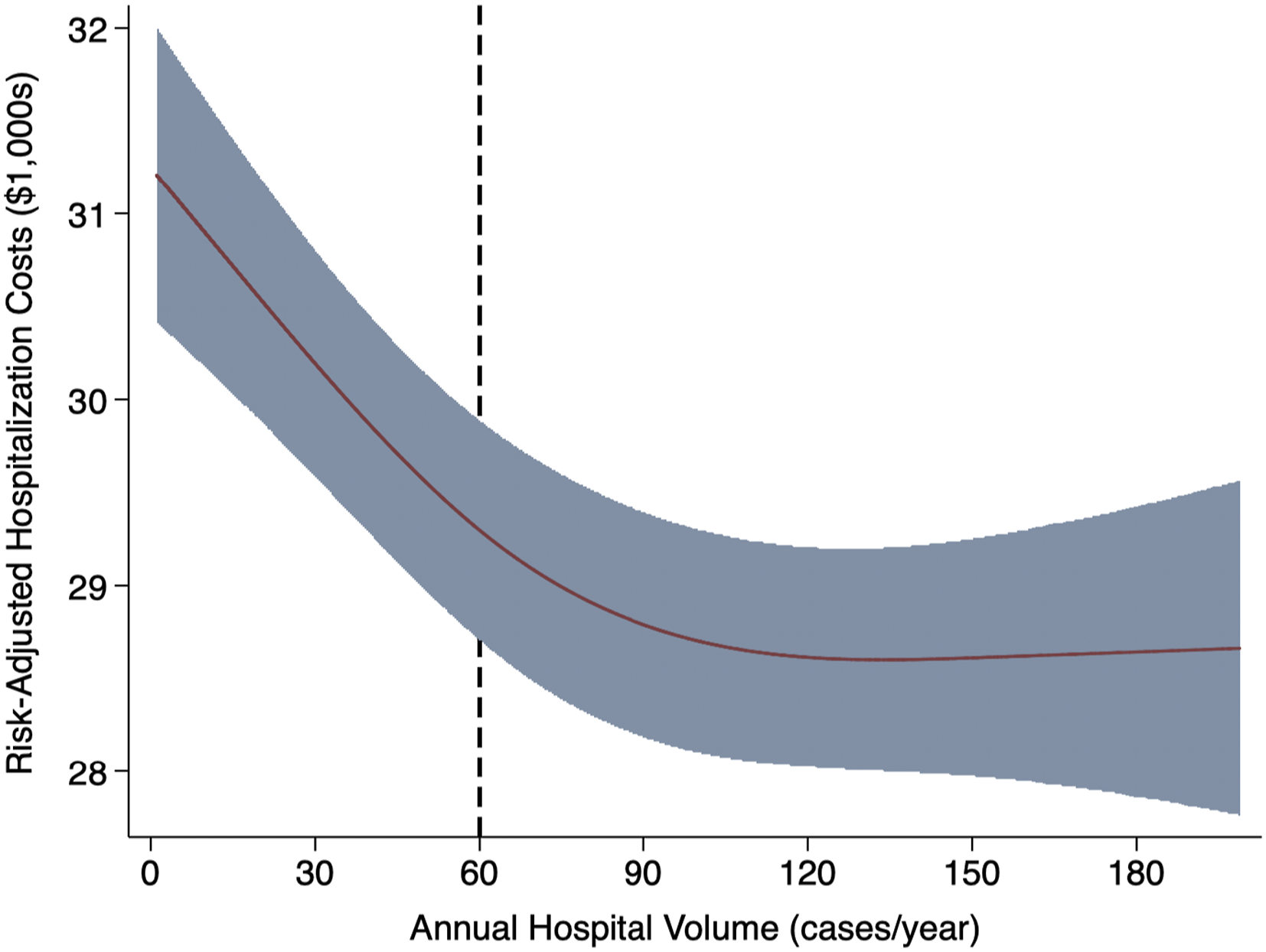
Patient and Hospital Factors at HVH and LVH
Patient, Operative, and Hospital Characteristics Stratified by Hospital Volume Status
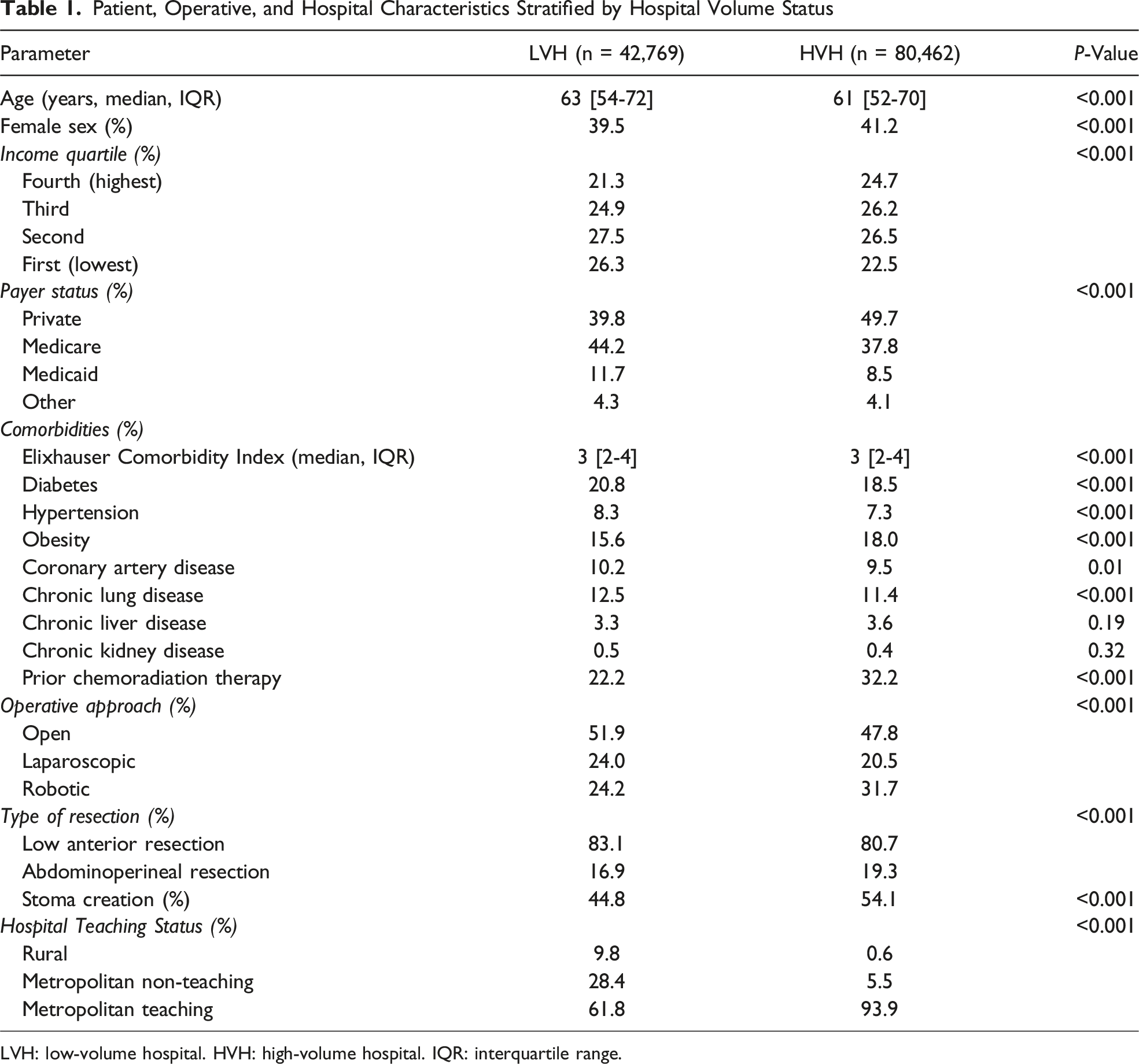
LVH: low-volume hospital. HVH: high-volume hospital. IQR: interquartile range.
Following risk adjustment, HVH remained associated with significantly greater odds of neoadjuvant chemoradiation (AOR 1.36 [95% CI 1.27-1.46]), robotic operations (1.23 [1.11-1.36]), APR (1.13 [1.06-1.20]), and stoma creation (1.22 [1.16-1.28]) relative to LVH (Figure 3, Supplemental Table 3). Furthermore, HVH was associated with decreased odds of Medicare (AOR 0.91 [95% CI 0.86-0.97]) and Medicaid (0.53 [0.48-0.58]) relative to private insurance. Factors associated with treatment at a high-volume hospital (reference: low-volume) among patients undergoing rectal cancer resection. Model C-statistic: 0.71. Ref: Reference.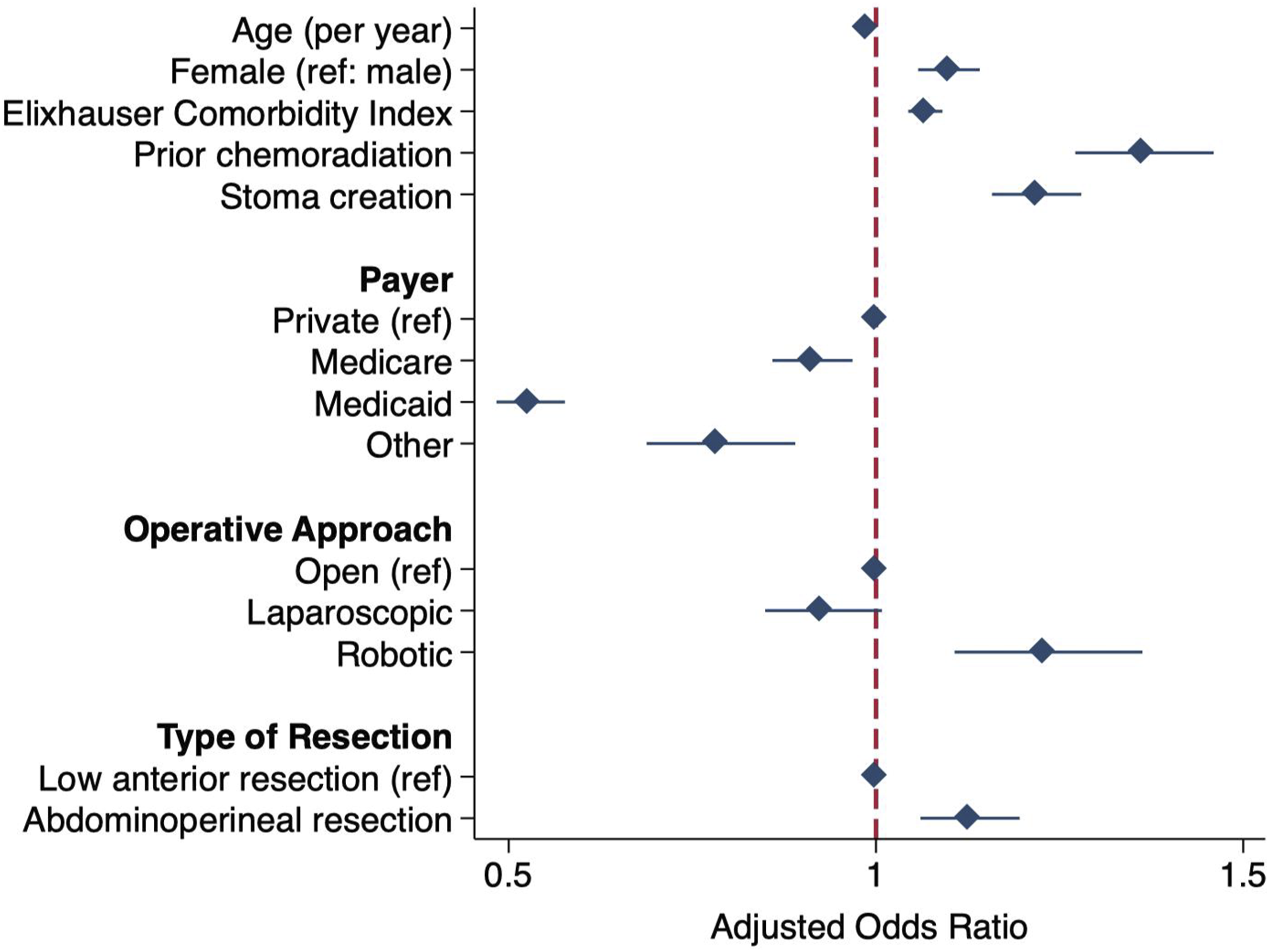
Outcomes at HVH and LVH
Unadjusted Outcomes Among Patients Undergoing Rectal Cancer Resection Stratified by Hospital Volume Status
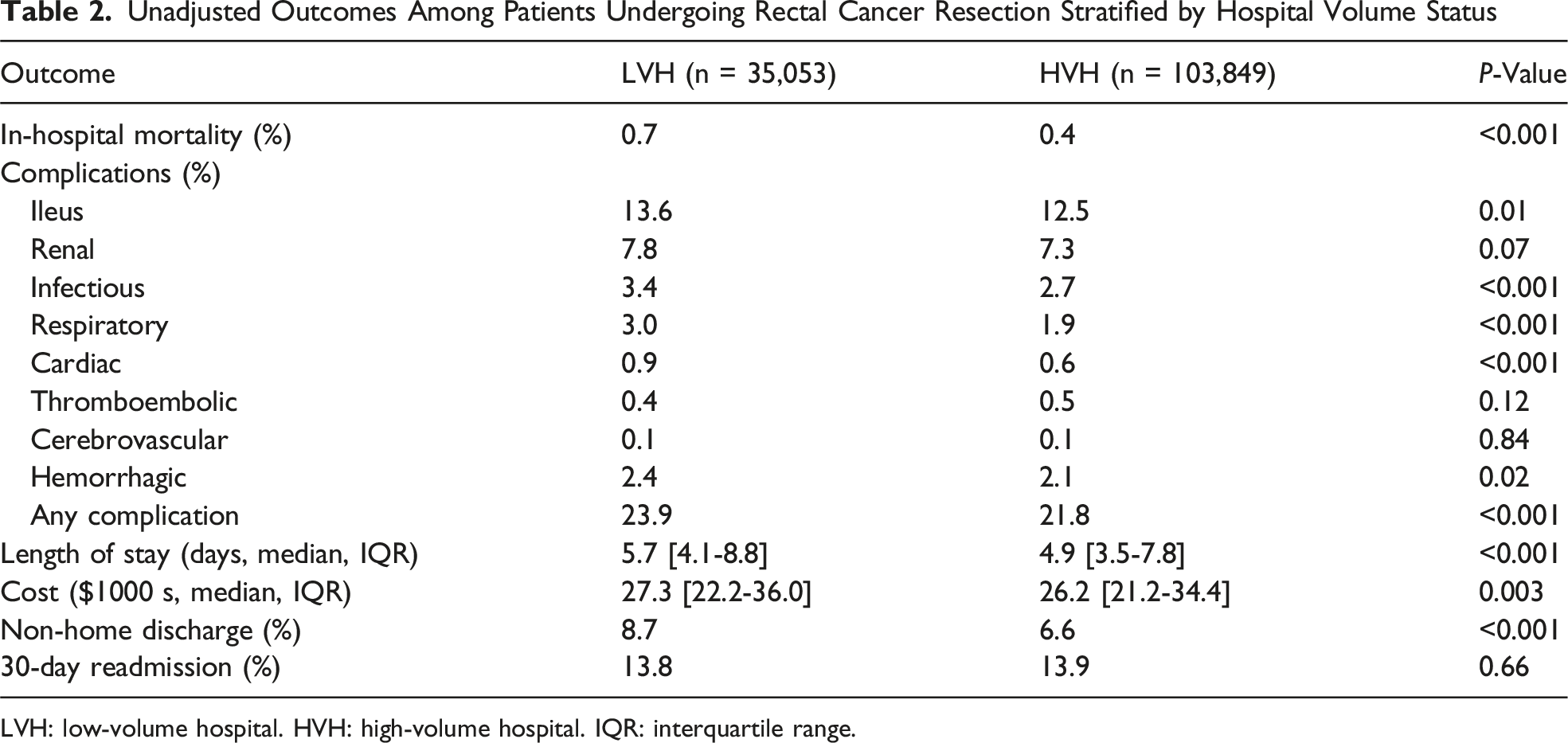
LVH: low-volume hospital. HVH: high-volume hospital. IQR: interquartile range.
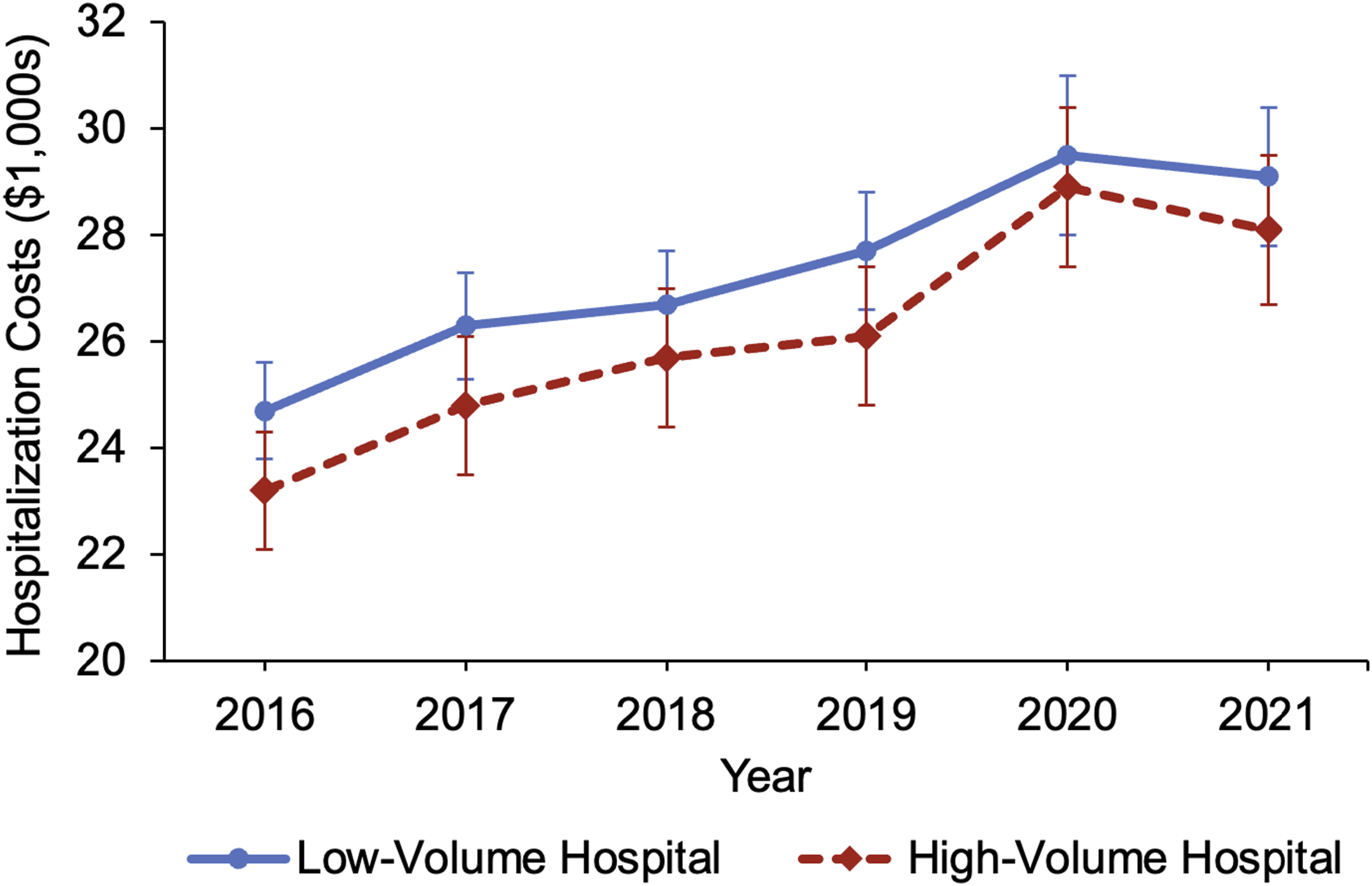
Temporal trends in hospitalization costs stratified by hospital volume status.
Adjusted Outcomes Associated With Treatment at a High-Volume Hospital (Reference: Low-Volume) Among Patients Undergoing Rectal Cancer Resection
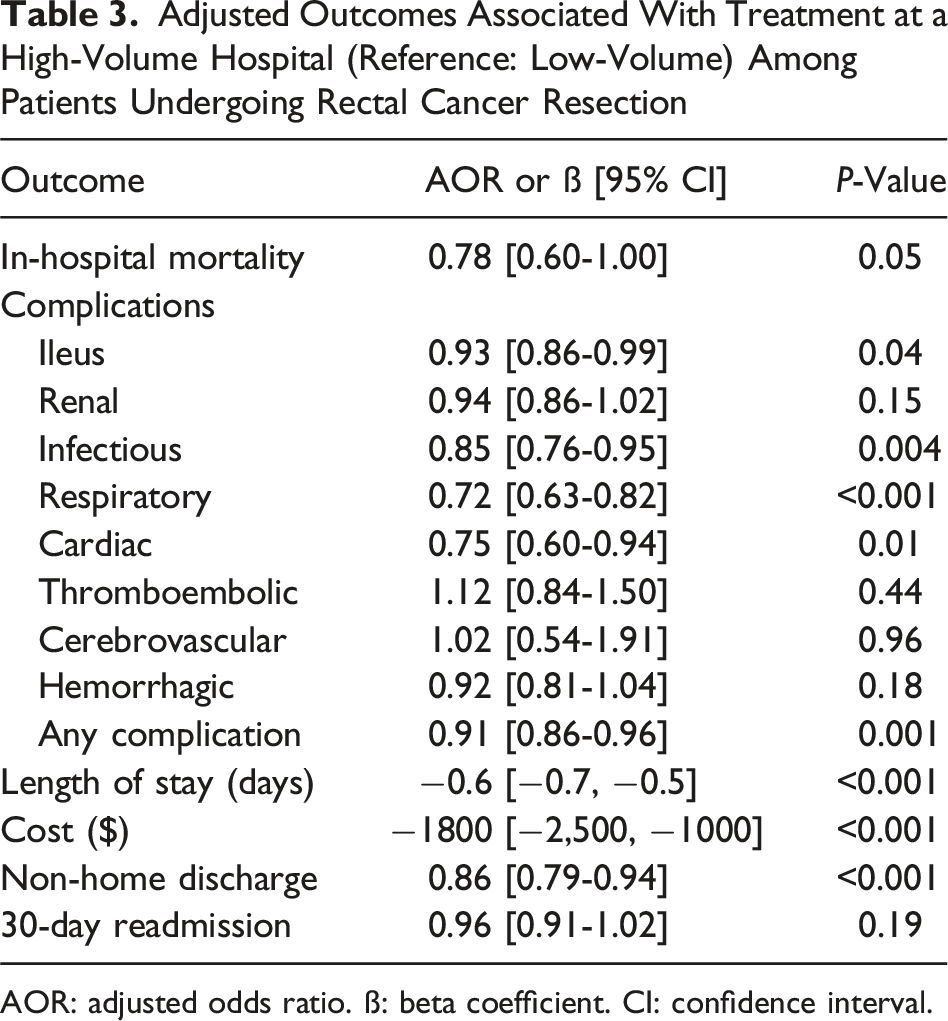
AOR: adjusted odds ratio. ß: beta coefficient. CI: confidence interval.
Discussion
Using a nationally representative cohort of patients undergoing rectal cancer resection, the present study aimed to characterize the relationship between hospital volume and hospitalization costs. We found increasing proctectomy volume to be associated with a nonlinear decrease in costs. After defining a minimum volume cutoff of 60 cases, the proportion of HVH patients was found to increase over time from 65.0% in 2016 to 67.2% in 2021. Patients at HVH more commonly had private insurance, neoadjuvant chemoradiation, and robotic operations, while LVH patients were more commonly treated at rural centers. Notably, HVH was associated with 9% lower odds of postoperative complications and over 15% lower odds of non-home discharge. In addition, HVH demonstrated a −0.6-day decrement in LOS and a -$1800 reduction in costs compared to LVH. The discrepancy in hospitalization costs between HVH and LVH persisted but narrowed over time. Several of our findings merit further discussion.
Prior limited studies have similarly found evidence of reduced expenditure at centers with high volume of colorectal surgery.5,7 One major concern with regionalization of care is the added cost and inconvenience of traveling to a HVH instead of seeking treatment at a local LVH. However, Leeds et al. reported that the total cost burden of undergoing rectal cancer surgery at a farther high-volume regional center would need to exceed $15,000 per patient to achieve economic breakeven, suggesting high cost-effectiveness. 7 Another raised concern is the increased cost associated with delivery of complex, higher quality care, including high nurse-to-bed ratios, staffing for intensive care units, specialist services, and advanced technology. 13 Of note, HVH patients demonstrated greater utilization of robotic surgery, APR, and stoma creation, which were all independently associated with increased costs. Nevertheless, the clinical benefits may outweigh the potential costs, as a 2013 national study of 1428 robotic colorectal cases found a $3000-8000 incremental reduction in costs associated with high-volume hospitals and surgeons. 5 Our findings similarly suggest an inverse cost-volume relationship, although with a more modest -$1800 decrement in costs at HVH. Of note, this study provides the first nationally representative cost analysis of rectal cancer surgery in the contemporary era and may be more generalizable. Interestingly, only 8-13% of hospitals were designated as HVH a decade ago compared to 22.1% of hospitals in the present work.5,14 The increase in proportion of HVH may be contributing to the narrowing cost disparity observed over time, indicating that further centralization of rectal surgical care may be beneficial.
Significantly lower odds of postoperative complications at HVH likely contribute to the reduction in inpatient costs and LOS. Our findings are consistent with prior literature demonstrating improved postoperative and long-term survival following rectal cancer surgery at centers of excellence. 4 Particularly for challenging deep pelvic dissection, greater surgeon and institutional experience lead to efficient, proficient operations and play a vital role in optimizing outcomes. 3 Furthermore, rectal cancer management often requires a multidisciplinary approach that is more accessible at HVH, with careful preoperative staging and extensive discussion with medical and radiation oncologists regarding neoadjuvant/adjuvant chemoradiation. 15 In addition, streamlined perioperative care pathways at HVH have led to more rapid recovery with decreased costs, effectively delivering value-based health care. 16 Efforts to identify and disseminate best practices from HVH are warranted, including multimodal prehabilitation, careful patient selection criteria, and enhanced recovery pathways.15-17
Notably, several patient and hospital-level factors were associated with treatment at HVH vs LVH. While HVH were almost all metropolitan teaching centers, LVH were more likely in rural locations, which has predicted worse overall survival in colon cancer compared to urban areas. 18 Rural patients travel greater distances to access care and experience longer times from cancer diagnosis to surgery. 18 Furthermore, a stark income-based disparity in access to HVH exists, as evident by the greater proportion of privately insured patients with higher socioeconomic status. Our findings suggest that access to HVH allows for a broader range of treatment options for patients, as HVH status was associated with increased likelihood of receiving neoadjuvant chemoradiation, robotic operations, APR, and stoma creation compared to LVH. Of note, the higher rate of stoma creation may be attributed to HVHs performing more APR procedures, which inherently require end colostomy creation, as well as the greater use of neoadjuvant chemoradiation, which often necessitates the placement of a diverting loop ileostomy. Total neoadjuvant therapy is increasing in utilization and has shown to increase the odds of complete pathologic response by 39%. 19 In addition, robotic-assisted surgery for rectal cancer has been associated with significantly lower conversion rates compared to conventional laparoscopic surgery. 20 Barriers in access to these multimodal forms of treatment at LVH need to be addressed in order to improve quality and cost efficacy of rectal cancer care.
This study has several limitations inherent to its retrospective nature and use of an administrative database. The NRD lacks granular clinical data including laboratory values, cancer staging, type and dose of neoadjuvant therapy, and anatomic complexity of each procedure. Outpatient data such as prior colorectal cancer screening and cost of travel were unable to be assessed. In addition, the clinical and financial outcomes analyzed were limited to the duration of each hospitalization within the 1-year surveillance period, and long-term survival was not available. Cumulative institutional and surgeon experience were not captured, as the NRD does not track hospitals across years or provide unique surgeon identifiers. Geographic variations in costs were unable to be assessed due to lack of hospital region data. Furthermore, specific operating room costs are not separately delineated within the total hospital charge data provided by the NRD. ICD coding may also be influenced by provider and hospital practices among participating centers in the NRD. In addition, the transition from ICD-9 to ICD-10 may have introduced variations in coding from prior literature of older data. Nevertheless, we utilized the largest all-payer readmissions database and robust statistical methods to enhance the generalizability of our findings at the national level.
In conclusion, the present study used a nationally representative database to demonstrate that increasing hospital volume of rectal cancer resection was associated with reduced hospitalization costs. Moreover, treatment at HVH was associated with decreased postoperative complications, duration of stay, and non-home discharge. Our findings suggest that streamlined perioperative care pathways at HVH may be improving clinical outcomes and reducing excess expenditure. Increasing access to multimodal neoadjuvant therapy and identifying perioperative best practices may help alleviate financial burden. Given the persistent disparity in expenditure over time, regionalization of care to HVH and cost mitigation strategies particularly at LVH are warranted to improve the value of rectal surgical care.
Supplemental Material
Supplemental Material - Cost-Volume Relationship in Rectal Cancer Resection Across the United States
Supplemental Material for Cost-Volume Relationship in Rectal Cancer Resection Across the United States by Ayesha P. Ng, Giselle Porter, Esteban Aguayo, Lavender Micalo, Troy N. Coaston, Peyman Benharash, and Hanjoo Lee in The American Surgeon™.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.