
Abstract
Background
One of the most commonly performed operations in the US, colectomy remains associated with a substantial incidence of postoperative complications. While there is increasing recognition that hospital for-profit financial structure may be linked with variation in morbidity, the impact of care at for-profit (FP) hospitals on outcomes following colectomy remains to be elucidated.
Methods
All adults undergoing elective/emergent colectomy for diverticular disease, inflammatory bowel disease, benign colonic neoplasms, or colon cancer, ≤2days of admission, were tabulated from the Nationwide Readmissions Database. Patients were stratified by care at FP centers into the FP and Non-FP cohorts. Following entropy balancing, multivariable models were developed to consider the independent association of FP status with key outcomes.
Results
Of ∼1,130,803 admissions for colectomy, 862 495 (76.3%) were elective. Among electively admitted patients, 74 933 (8.7%) were grouped as FP. After risk adjustment, care at FP institutions was associated with greater odds of major morbidity (AOR 1.27, CI 1.22-1.32), non-home discharge (AOR 1.20, CI 1.13-1.27), and non-elective readmission (AOR 1.26, CI 1.12-1.32), but lower per-patient expenditures (β-$2430/patient, CI -2,860, -2010). Considering the 268 308 emergent cases, 38 568 (14.4%) were managed at FP hospitals. Following multivariable adjustment, treatment at FP hospitals remained associated with increased morbidity (AOR 1.16, CI 1.11-1.21) and decreased costs (β-$5,630, CI -6,210, −5,050).
Discussion
Undergoing colectomy at FP hospitals was associated with greater complications and readmissions, but reduced per-patient expenditures. Future research should consider the factors contributing to inferior clinical outcomes at these centers. Best practices should be shared across institutions, irrespective of financial structure.
Keywords
Key Takeaways
• Approximately 16% of centers performing colectomy were for-profit institutions. • Across both elective and emergent colectomy, hospital for-profit status was linked with greater morbidity and readmissions. • For-profit hospitals demonstrated similar duration of hospitalization, but reduced per-patient expenditures.
Introduction
With more than 275 000 cases performed each year, colectomy remains one of the most common operations in the US. 1 In both the elective and emergent settings, however, colon resections have been associated with a substantial incidence of complications, ranging from ∼10-30%.2,3 As a high-volume procedure with relatively substantial morbidity, colectomy has received growing focus as an area for surgical quality improvement efforts. Indeed, outcomes have been described to vary significantly by both patient and hospital-level factors.1,4,5
Importantly, there is increasing recognition that hospital for-profit financial structure may be linked with variation in perioperative outcomes. For-profit institutions (FP) reportedly optimize profit margins by selecting younger, less complex patient populations, focusing on highly reimbursed procedures, and reducing overhead costs. 6 Across clinical contexts, the impact of such efforts on clinical outcomes has been mixed, with some detailing no association between FP status and morbidity,7,8 and others reporting greater complications 9 and readmissions. 10 However, the influence of care at FP hospitals on outcomes following colectomy has yet to be elucidated. With colectomy performed across a wide range of hospitals and in both elective and emergent settings, a comprehensive understanding of how FP structure shapes outcomes could guide institutional and systems level quality improvement efforts.
In the present work, we examined the association between care at FP hospitals and clinical and financial outcomes following colectomy. We hypothesized management at FP centers to be linked with greater morbidity, but decreased per-patient expenditures, compared to treatment at non-FP hospitals.
Methods
We queried the 2016-2022 Nationwide Readmissions Database (NRD) to tabulate all adult (≥18 years) hospitalizations entailing elective or emergent colectomy for diverticular disease, inflammatory bowel disease, benign colonic neoplasms, or colon cancer, within 2 days of admission, using previously published International Classification of Diseases, Tenth Revision (ICD-10) procedure codes. 4 The NRD represents the largest national in-hospital registry detailing readmission outcomes and uses survey-weighting methodology to accurately estimate ∼60% of all US hospitalizations, each year.
We excluded records missing key data related to age, sex, in-hospital mortality, or elective case status (<1%). Subsequently, records demonstrating care at a for-profit hospital were classified as the FP cohort. Patients treated at government-owned or not-profit institutions, were categorized as the Non-FP (Figure 1). Study CONSORT Diagram of Survey-Weighted Estimates Of 1,130,803 patients undergoing elective or emergent colectomy within 48 hours of admission, 113 501 (10.0%) were treated at For Profit (FP) hospitals, while 1,017,302 (90.0%) were managed at Non-FP centers. All estimates represent survey-weighted methodology.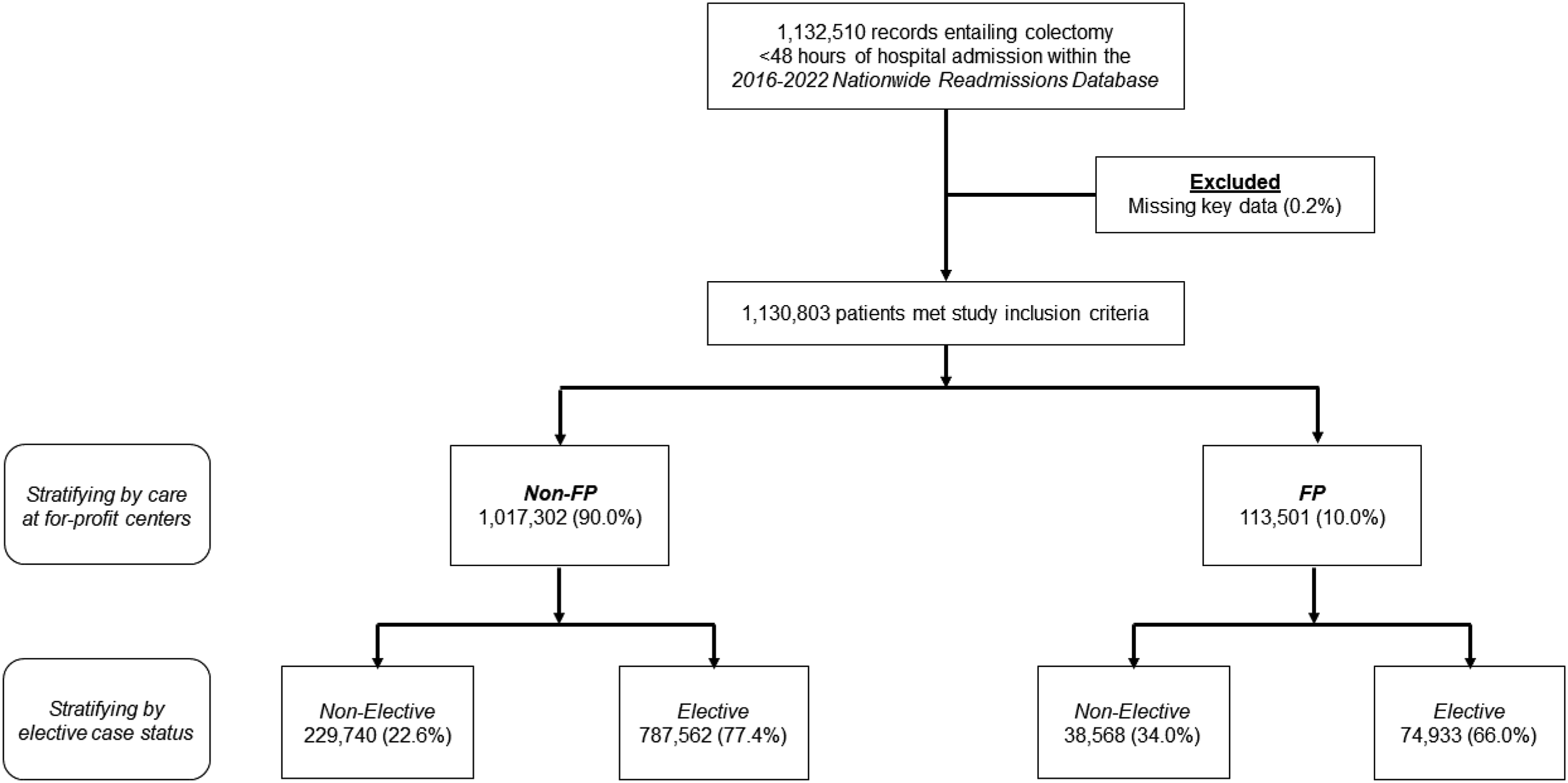
Relevant patient, disease, and hospital factors were delineated using the Healthcare Cost and Utilization Project Data Dictionary. The van Walraven modification of the Elixhauser Comorbidity Index was used to quantify patient comorbidity burden. 11 Surgical approach was stratified as open or minimally invasive, including laparoscopic or robotic operations. Comorbidities and perioperative complications were ascertained using ICD-10 diagnosis codes. Complications were further categorized as cardiac, infectious, respiratory, renal, thrombotic, and stroke. Per-patient hospitalization costs were computed using hospital-specific cost-to-charge ratios, which were inflation-adjusted using the 2022 Personal Healthcare Price Index.
We performed distinct analyses considering elective and non-elective cases. The primary study endpoint was in-hospital mortality. We secondarily considered the incidence of perioperative complications, length of stay (LOS), hospitalization expenditures, and discharge to extended care nursing facilities.
Continuous data are reported as medians with interquartile range (IQR) or means with standard deviation (SD). Categorical variables are shown as group proportions (%). The significance of intergroup comparison was evaluated using the Mann-Whitney U, student’s t-test, and Pearson’s χ2 test, as appropriate. Multivariable regression models were developed to assess the independent association of treatment at FP centers with key study outcomes. To minimize model bias and enhance out-of-sample validity, all covariates were automatically selected via elastic net regularization, and included patient age, sex, comorbidity burden, income, insurance coverage, indication for colectomy, extent of resection, operative approach, and admission year, as well as hospital teaching status and annual case volume. Logistic and linear regression outputs are detailed as adjusted odds ratio (AOR) or beta-coefficients (β), both with 95% confidence intervals (CI).
All statistical analyses were conducted using Stata 18.0 (StataCorp, College Station, TX). The threshold for statistical significance was set at α = 0.05. As the NRD is fully deidentified, this study was exempted from full review by the University of California, Los Angeles, Institutional Review Board.
Results
Demographic, Clinical, and Hospital Characteristics, Stratified by Elective Case Status and Care at For-Profit Hospitals.
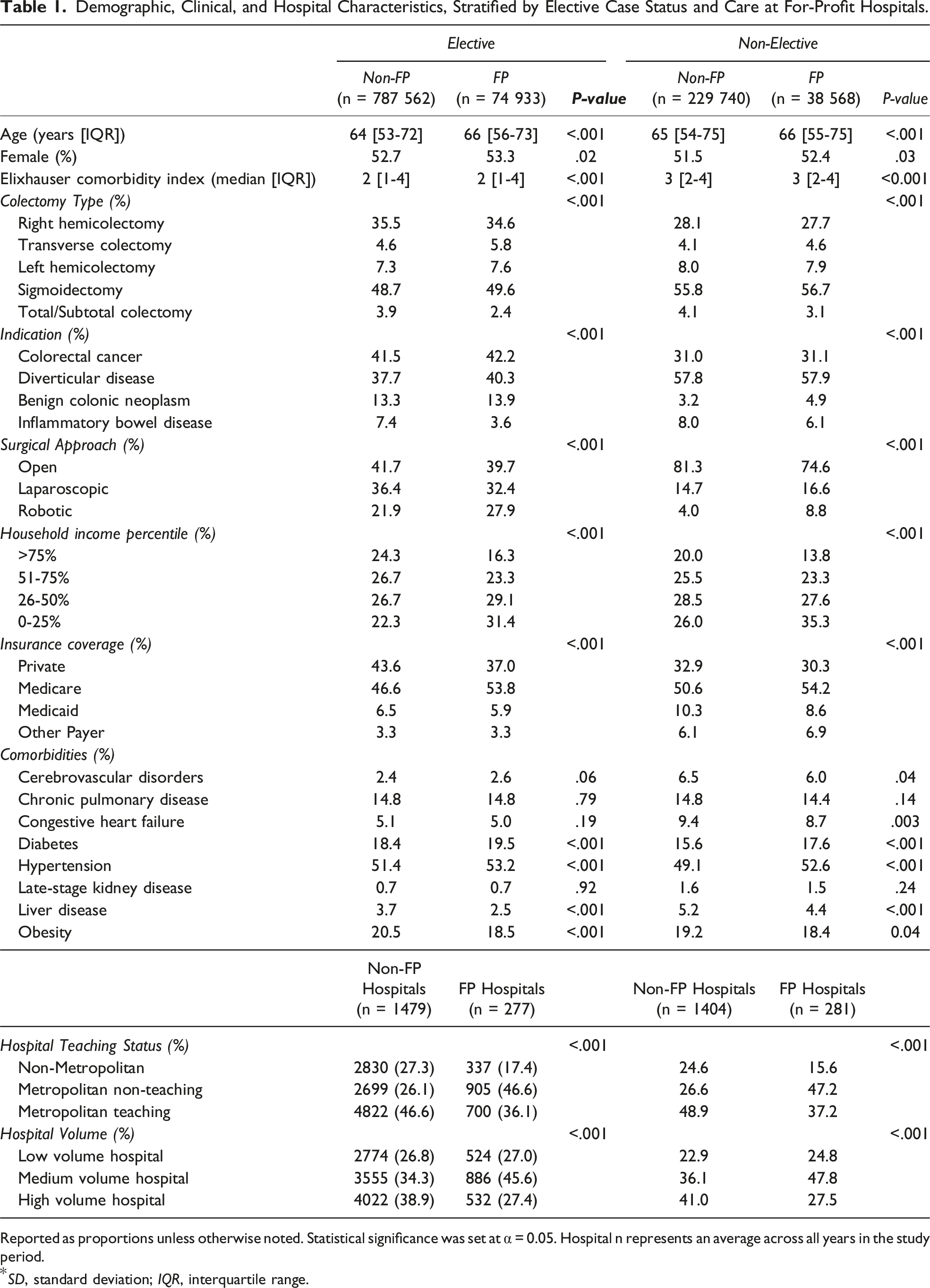
Reported as proportions unless otherwise noted. Statistical significance was set at α = 0.05. Hospital n represents an average across all years in the study period.
*SD, standard deviation; IQR, interquartile range.
Unadjusted and Adjusted Outcomes Stratified by Elective Case Status and Care at For-Profit (FP) Hospitals.
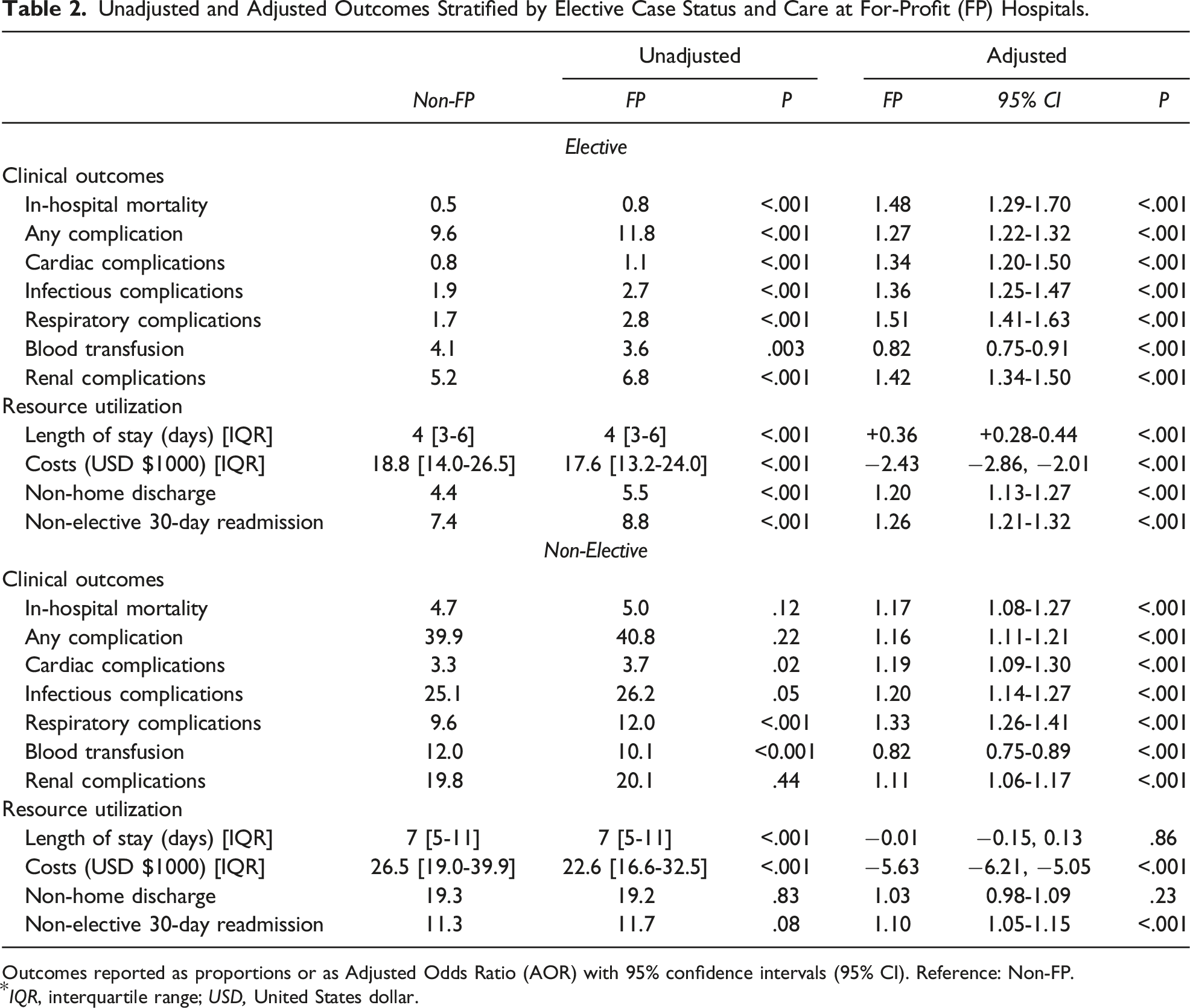
Outcomes reported as proportions or as Adjusted Odds Ratio (AOR) with 95% confidence intervals (95% CI). Reference: Non-FP.
*IQR, interquartile range; USD, United States dollar.
Elective Cases
Among 862 495 elective colectomy cases, 74 933 (8.7%) were performed at FP hospitals. The proportion of elective cases performed at FP hospitals declined over the study period, from 9.2% in 2016 to 8.3% in 2022 (P for trend<0.001) (Figure 2). Trends in Treatment at For Profit Hospitals. Across the study period, the proportion of patients undergoing elective colectomy at For Profit (FP) hospitals decreased, from 9.2% in 2016 to 8.3% in 2022 (P for trend<.001). A similar trend was noted among patients undergoing non-elective colectomy, such that the proportion decreased from 15.4% in 2016 to 12.9% in 2022 (P for trend<0.001). *indicates statistical significance, P < .001.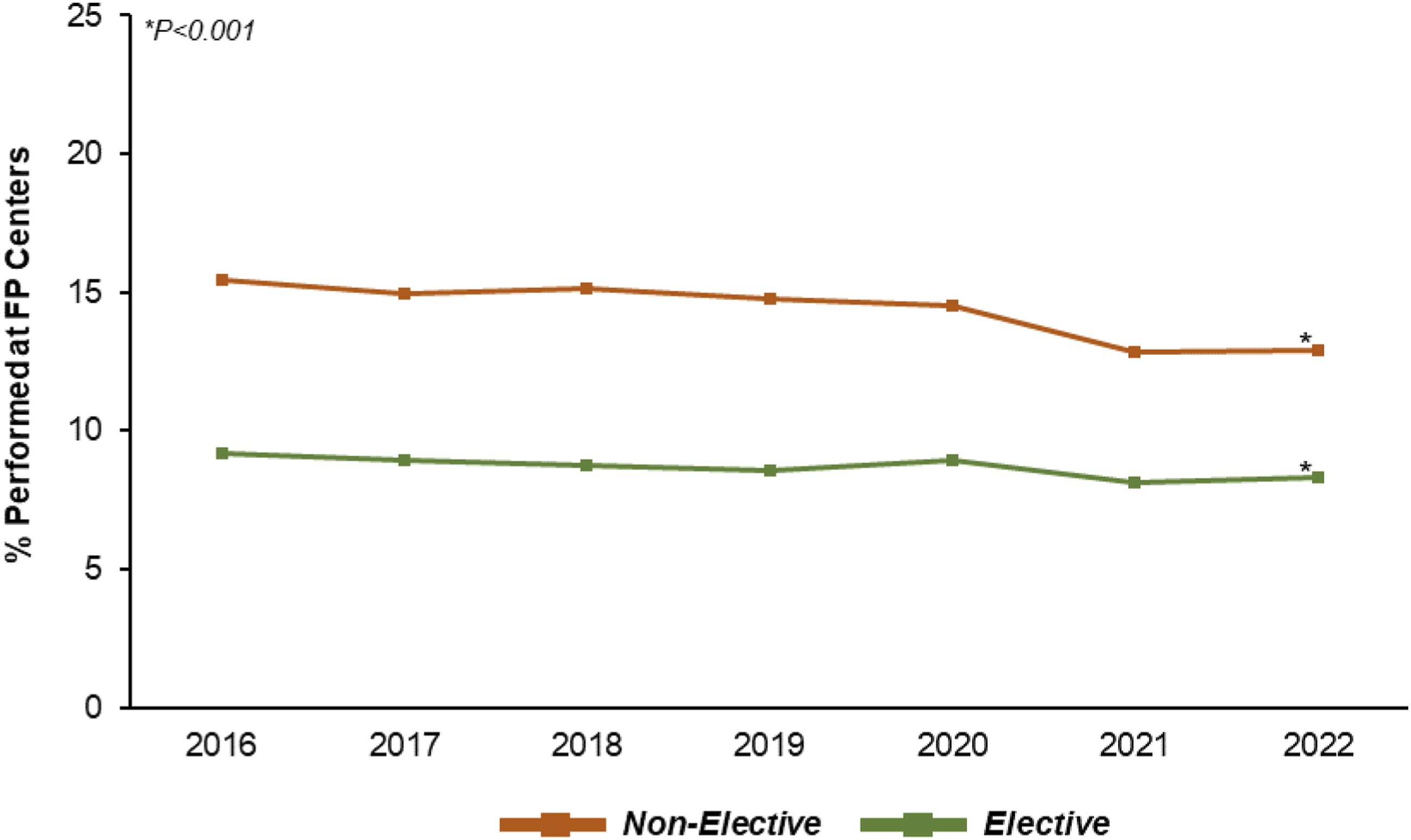
On average, the FP cohort was older (66 [56-73] vs 64 years [53-72], P < 0.001) but of comparable sex and comorbidity burden. FP patients were more commonly of lowest median household income quartile (31.4 vs 22.3%, P < .001) and less often privately insured (53.8 vs 46.6%, P < .001). Indication for colectomy and extent of surgical resection were clinically similar between groups. However, FP more frequently underwent robotic-assisted resection (27.9 vs 21.9%, P < .001), relative to others.
Moreover, FP centers were more frequently metropolitan non-teaching hospitals (46.6 vs 26.1%, P < .001) and less often high-volume institutions (27.4 vs 38.9%, P < .001).
On bivariate comparison, FP demonstrated an incrementally higher, but not clinically significant, rate of in-hospital mortality (0.8 vs 0.5%, P < .001). Further, FP more often experienced any complication (11.8 vs 9.6%, P < .001). Length of stay was clinically comparable between groups, but FP experienced lower per-patient expenditures ($17,600 [13 200-24,000] vs 18 800 [14 000-26,500], P < .001).
Following multivariable risk adjustment, care at FP hospitals remained associated with higher odds of in-hospital mortality (AOR 1.48, CI 1.29-1.70) and major morbidity (AOR 1.27, CI 1.22-1.32). Specifically, treatment at FP hospitals was linked with greater likelihood of perioperative infection (AOR 1.36, CI 1.25-1.47), acute kidney injury (AOR 1.42, CI 1.34-1.50), and respiratory complications (AOR 1.51, CI 1.41-1.63; Figure 3A). Considering resource utilization, management at FP institutions was associated with a +0.36 day increase in LOS (β + 0.36 days, CI 0.28-0.44), but a $2430 decrement in expenditures (β -$2430/patient, CI -2,860, −2010). Finally, FP demonstrated greater odds of both non-home discharge (AOR 1.20, CI 1.13-1.27) and non-elective readmission within 30 days (AOR 1.26, CI 1.21-1.32; Figure 3B). Morbidity and Readmission Following Elective Colectomy (A) Adjusted risk of major morbidity and (B) Cumulative hazard of readmission, stratified by care at For Profit (FP) centers. Following multivariable risk adjustment, care at FP hospitals remained associated with incrementally increased rates of renal, infectious, and respiratory complications, as well as composite major morbidity. Similarly, undergoing colectomy at FP hospitals was linked with a 26% increase in the relative risk of non-elective readmission within 30 days of index discharge. *indicates statistical significance, P < .001.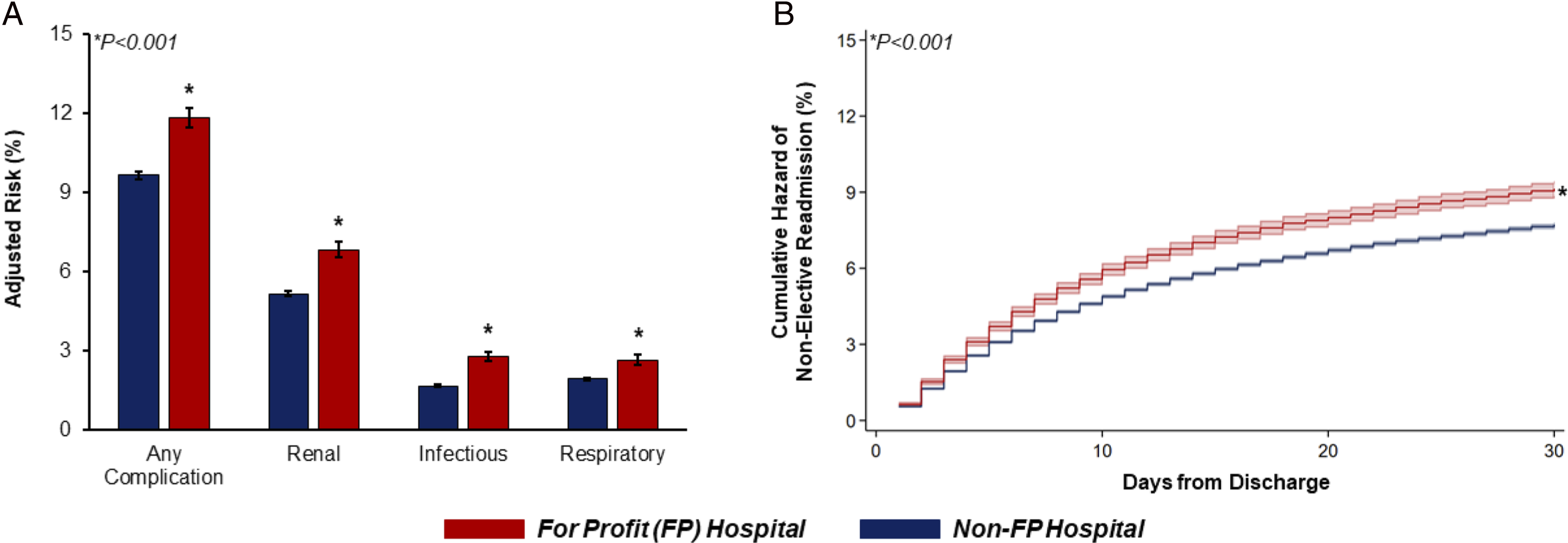
Non-Elective Cases
Evaluating the 268 308 cases entailing non-elective colectomy, 38 568 (14.4%) were managed at FP hospitals and 229 740 (85.6%) at Non-FP hospitals. The proportion of non-elective cases performed at FP hospitals also decreased, from 15.4% in 2016 to 12.9% in 2022 (P for trend<.001).
The FP cohort was of incrementally lower age (65 [54-74] vs 66 years [55-75], P < .001), but of similar sex and comorbidities. FP was more frequently of lowest income (35.3 vs 26.0%, P < .001) and Medicare insurance coverage (54.2 vs 50.6%, P < 0.001).
On unadjusted analysis, FP faced similar rates of in-hospital mortality (5.0 vs 4.7%, P = 0.12) and any major complication (40.8 vs 39.9%, P = 0.22).
After multivariable risk adjustment, care at FP centers remained associated with greater likelihood of in-hospital mortality (AOR 1.17, CI 1.08-1.27) and major morbidity (AOR 1.16, CI 1.11-1.21), including infectious (AOR 1.20, CI 1.14-1.27), respiratory (AOR 1.33, CI 1.26-1.41), and renal complications (AOR 1.11, CI 1.06-1.17; Figure 4). While LOS was similar between groups, treatment at FP hospitals was linked with decreased per-patient expenditures (β-$5630/patient, CI -$6210, -$5050). Coefficient Plot of Outcomes Following Non-Elective Colectomy Following risk adjustment, care at a For Profit (FP) hospital was associated with greater odds of in-hospital mortality, many complications, and non-elective readmission, following emergent colectomy. Reference: Care at Non-FP hospitals. Error bars represent 95% confidence intervals. *indicates statistical significance, P < .001.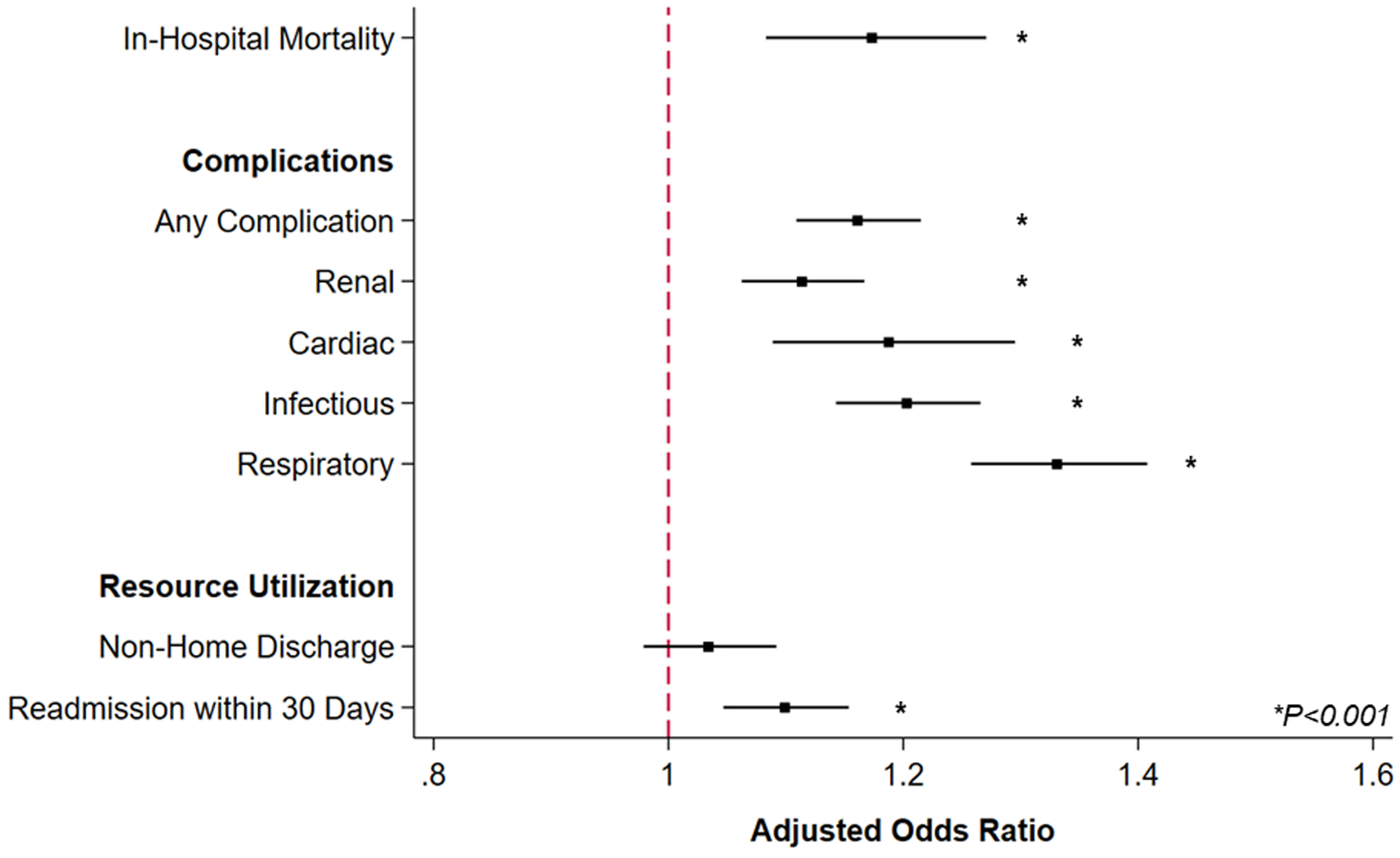
Discussion
We examined the association of care at FP hospitals with clinical and financial endpoints following colectomy across the US and made several important observations. First, ∼16% of hospitals performing colon resections were FP institutions. Care at FP hospitals was associated with an incremental increase in the adjusted risk of complications after both elective and urgent/emergent procedures, but lower per-patient charges. Furthermore, treatment at FP centers was linked with greater non-elective readmission. With implications towards interhospital quality efforts and broader health system policy, these findings warrant further discussion.
In our study, patient populations did not significantly differ by age or comorbidity burden between FP and non-FP hospitals, as has been previously reported. However, FP patients were more frequently insured by Medicare, which may reveal underlying trends in case-mix selection. Indeed, prior work has reported FP institutions to contribute to higher Medicare spending12,13 and engage in so-called “cream skimming,” in which such institutions are intentionally located in areas serving more profitable patient populations. 14 Yet, in the present work, FP institutions were also noted to serve greater proportions of lower income patients. Therefore, the extent of patient selection practices exhibited by these centers remains unclear and requires further investigation.
We identified care at FP hospitals to be associated with greater major perioperative morbidity following both elective and emergent operations. Our work accords with a growing body of literature linking care at such institutions with inferior clinical outcomes across a myriad of clinical contexts. 15 While the contributors to inferior outcomes remain to be wholly elucidated, these events may be inherently related to FP hospital structure. In contrast to non-for-profit institutions, the profits of clinical care in a FP institution are redirected to the hospital’s share-holders. Unfortunately, this approach may disincentivize FP hospitals from investing in quality-improving technologies, focusing instead on cost-saving measures. For example, FP institutions have been reported to reduce nurse-to-patient ratios, with mixed effects on patient outcomes. 16 Given the clinical similarities between patient cohorts, these hospital-level differences may contribute to the higher incidence of infectious, respiratory, and renal complications observed in our study. Although the absolute risk increase is small, our findings suggest disparities in the quality of care between FP and non-FP institutions, which could influence patients’ long-term health trajectories. Notably, prospective payment systems—such as those implemented in Medicare—have also been criticized for incentivizing FP hospitals to prioritize cost-saving strategies over quality improvement investments. This shift has enabled FP hospitals to become more competitive and gain market share compared to non-FP hospitals. 16
Of note, we found FP centers to more frequently utilize robotic-assisted approaches in both the elective and emergent setting. This finding contradicts a previous study by Barbash et al, 17 who reported FP hospitals to be less likely to acquire a surgical robot, from 2005 to 2009. Ultimately, we suggest our finding may stem from the dramatic shifts in the landscape of surgical care in the two decades since their assessment. While still requiring upfront investment, robotic surgical systems are a strong attractant for new patients 18 and may be particularly important in the contemporary competitive surgical care market. 19 These factors may indirectly contribute to the profit margins even if they are not directly reflected in the charges submitted for reimbursement. Indeed, others have more recently found a positive association between robotic surgical systems and hospital profit margins due to market competition and patient capture. 20
Finally, among patients undergoing elective colectomy, care at FP hospitals was linked with a ∼26% increase in the relative risk of non-elective readmission within 30 days of discharge. It is certainly possible this difference in readmission risk also stems from hospital-level factors, and in particular efforts to reduce LOS. Yet, this greater incidence of readmission is especially significant, given that many FP institutions have branded themselves as promoting a more cost-efficient approach to healthcare. While we noted reduced per-patient expenditures at FP hospitals, those charges only reflect the index hospitalization. The increased likelihood of discharge to extended care facilities, or non-elective readmission, faced by FP patients, may therefore suggest the potential for additional financial burden on the overall health system. Ultimately, future research should consider this question and track cost savings longitudinally, to accurately answer whether FP institutions truly reduce the cost and improve the value of care.
The present work has several important limitations. Radiographic and laboratory data is not documented within the NRD. We could not ascertain symptom burden, severity of disease, or history of gastrointestinal pathology or intervention. Similarly, granular hospital data, such as nurse-to-patient ratios, surgeon experience, the availability of enhanced recovery after surgery pathways, or other intrahospital care algorithms, was unavailable for analysis. Finally, FP hospitals have been reported to up-code diagnosis-related groups, in an effort to optimize billing practices and enhance profitability. These differences in billing strategies between FP and non-FP institutions may, at least in part, underlie the noted variation in complication rates in our administrative registry-based study. 13 Despite these limitations, we applied robust statistical methods and analyzed a large national cohort, to comprehensively report the impact of care at FP hospitals on outcomes following colectomy.
In conclusion, we found care at FP hospitals to be linked with greater morbidity and readmission, but reduced per-patient expenditures following colectomy, with the greatest impact among emergent cases. These differences persisted even after adjusting for the greater proportion of minimally invasive cases performed at FP centers. Our findings call for the sharing of best practices and perioperative care pathways between institutions, to improve outcomes at both FP and non-FP hospitals. Furthermore, future research should investigate the factors contributing to reduced per-patient expenditures at FP hospitals and ascertain whether these cost-containment strategies could be more broadly disseminated, to increase the value of care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.