
Abstract
Background
Subtotal cholecystectomy (STC) is a viable alternative for challenging cases of severely acute or chronic inflammation of the gallbladder. However, despite its advantages, patients undergoing STC still face the risk of developing symptomatic gallstones in the remnant gallbladder. In such cases, redo resection of the gallbladder remnant is required, posing some technical challenges. In this report, we share our experience in diagnosing and surgical management of remnant gallbladder cholecystitis.
Methods
A retrospective study of all patients admitted to a tertiary care hospital with symptoms directly linked to gallbladder remnant stones from 2018 to 2023 was performed.
Results
Six patients were admitted with symptoms directly linked to gallbladder remnant stones. The median age at presentation was 50 years (IQR 25-75), with median interval between the index surgery and the current presentation of 9.5 months (IQR 3-90). The presentation varied and included stump cholecystitis, cholangitis, Mirizzi syndrome, and liver abscess. All 6 patients underwent laparoscopic redo cholecystectomy, with 1 conversion to open surgery and without major complications. Symptoms resolved in all patients.
Conclusions
Symptomatic gallstone disease in remnant gallbladder is rare and requires redo cholecystectomy. According to our limited series, laparoscopic redo cholecystectomy may be feasible and safe.
Introduction
Laparoscopic cholecystectomy is one of the most frequently performed surgical procedures, due to the many advantages of minimally invasive technique.1,2 The implementation of the “critical view of safety” technique, pioneered by Strasberg et al in 1995, 3 has further improved patient’s safety by reducing the risk of bile duct injury during the procedure. Although bile duct injury is a rare complication, its potential severity and long-term consequences have prompted surgeons to explore safer alternatives in “bail-out” situations.4,5 In cases where achieving the critical view of safety is not feasible, due to severe inflammation, fibrosis, etc, a subtotal cholecystectomy (STC) may be performed to prevent bile duct injuries.6-8 However, concerns have been raised regarding the persistence of symptoms related to the remnant gallbladder after STC, often necessitating a redo cholecystectomy in symptomatic patients. 9
In this series, we report our recent experience redo remnant cholecystectomy performed at a tertiary center.
Methods
A retrospective review of medical records at our institution was performed including the period from 2018 to 2023. The objective was to identify patients who had experienced “stump cholecystitis” or “remnant cholecystitis” and underwent redo cholecystectomy.
The information sought included patients’ demographics, surgical and medical history, details of the index surgery, clinical presentation, imaging findings, operative and postoperative data and outcome. Complications were classified according to the Clavien-Dindo Classification System. 10 Symptoms resolution was retrieved from postoperative office visits notes. To ensure ethical compliance, this study received approval from the institutional review board.
Results
Patients’ Demographics and Medical Background.
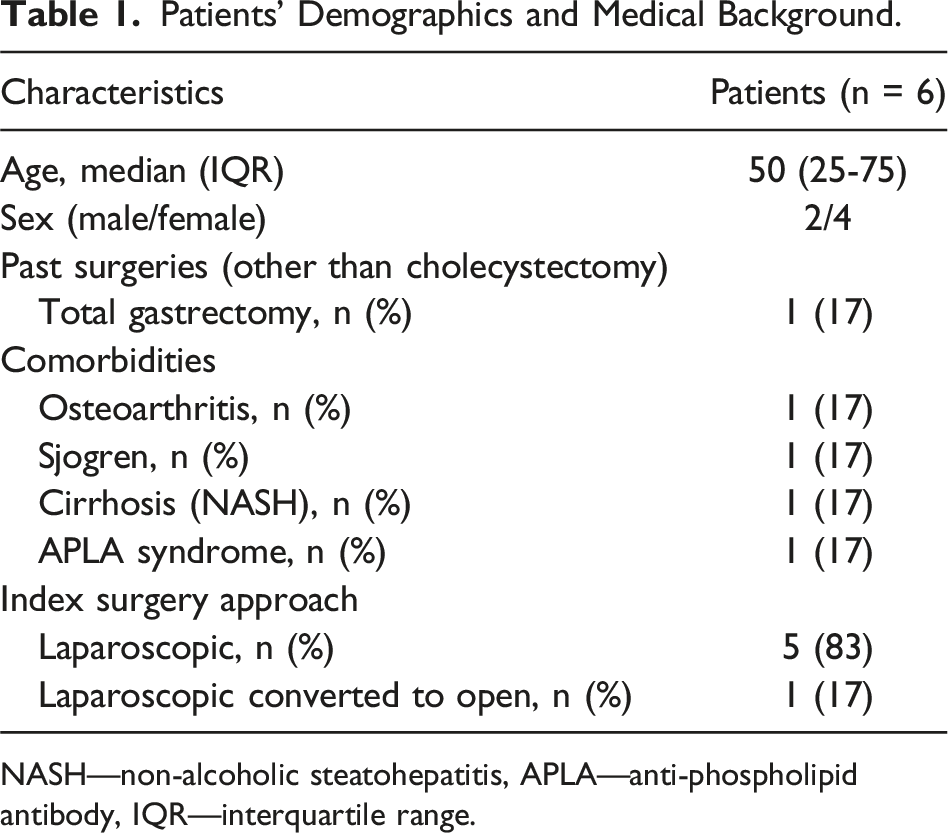
NASH—non-alcoholic steatohepatitis, APLA—anti-phospholipid antibody, IQR—interquartile range.
Presentation, Workup, Surgical Details, and Outcomes.
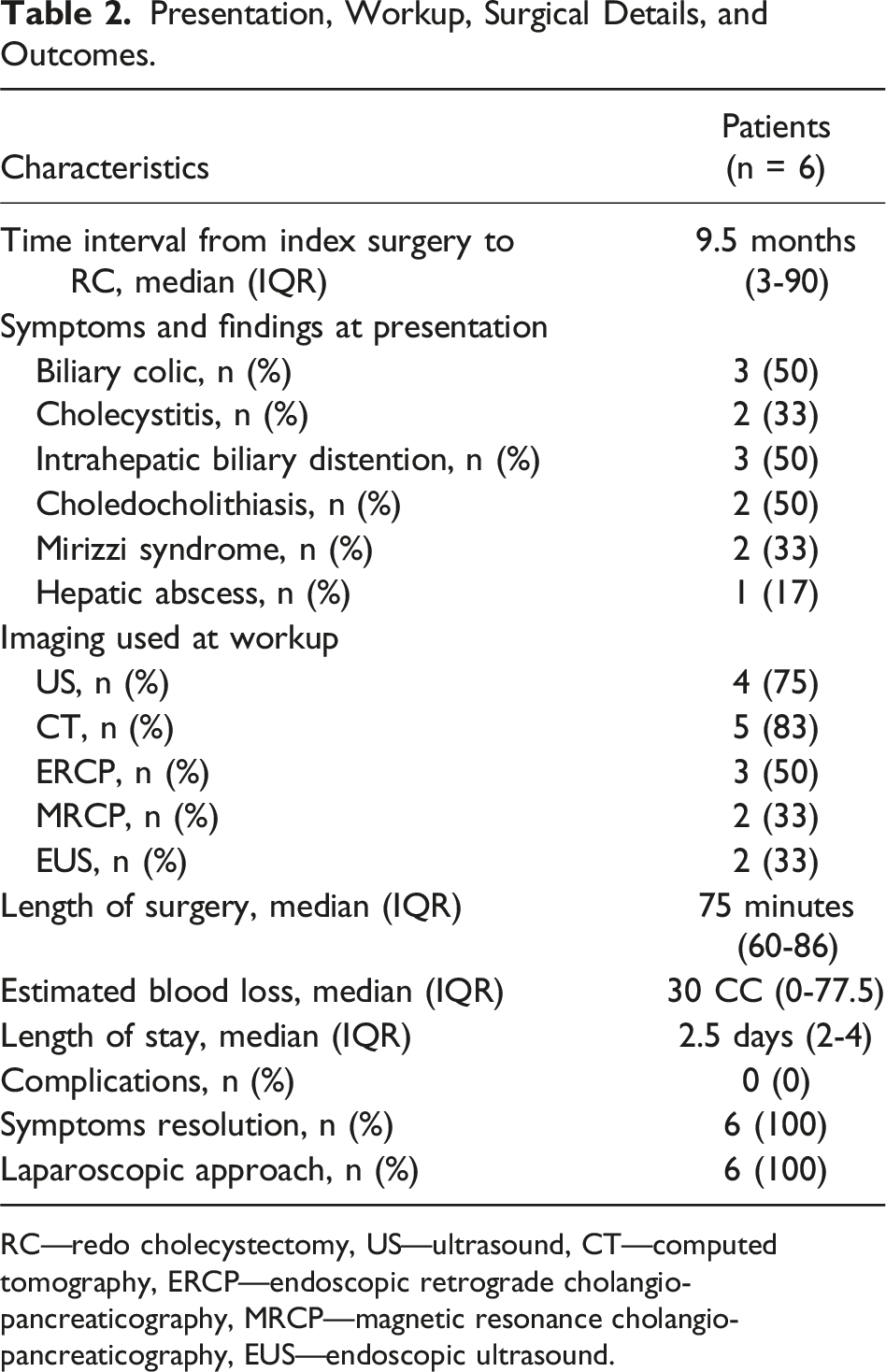
RC—redo cholecystectomy, US—ultrasound, CT—computed tomography, ERCP—endoscopic retrograde cholangio-pancreaticography, MRCP—magnetic resonance cholangio-pancreaticography, EUS—endoscopic ultrasound.
Of note, the median length of operation was only 75 minutes (IQR 60-86) despite the challenges arising in “redo surgeries.” No short- or long-term complications were recorded, and all patients reported resolution of their symptoms.
Discussion
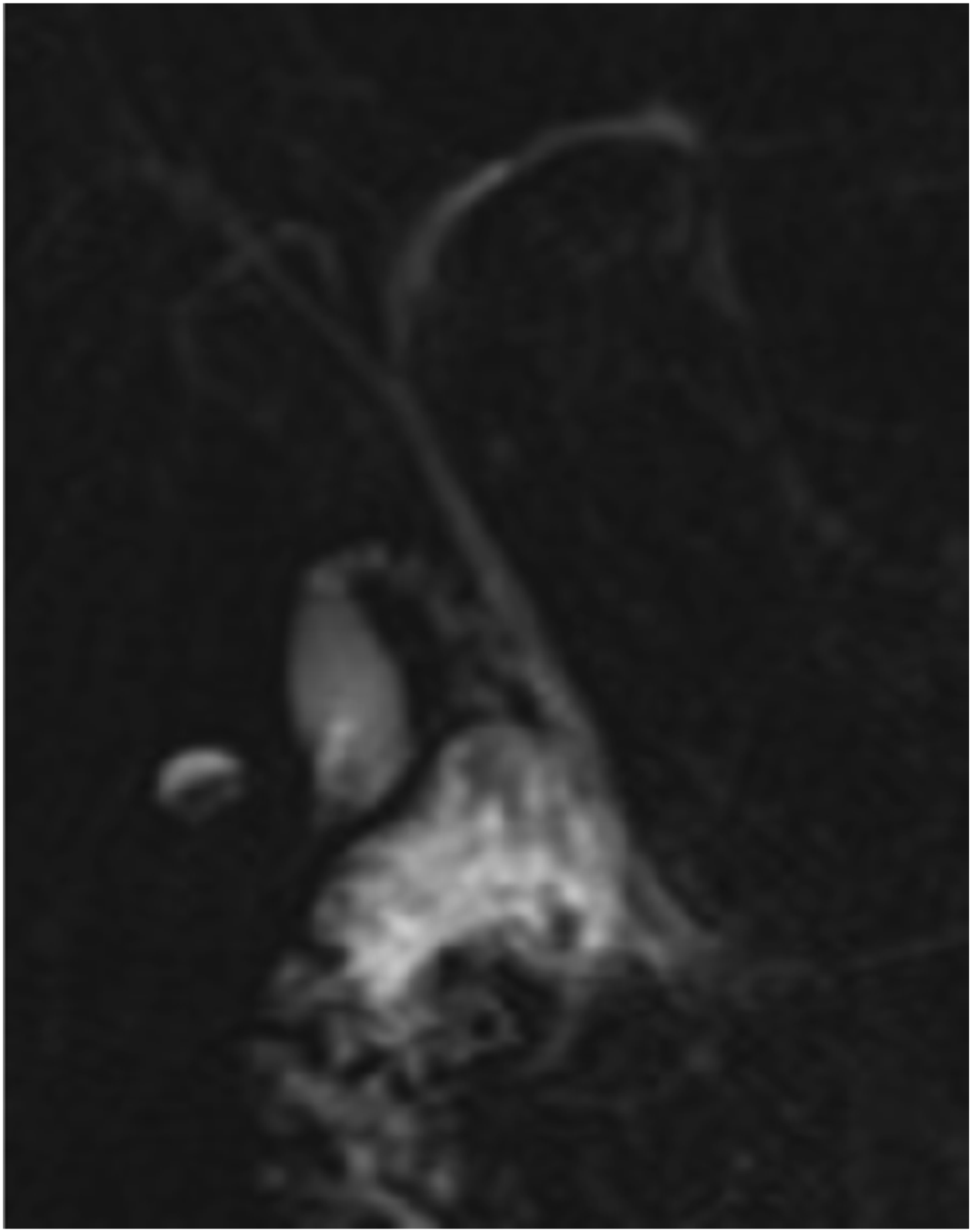
Subtotal cholecystectomy (STC) is an important surgical alternative as a bailout in complex cases, in order to avoid the risk of bile duct injury. 11 However, as highlighted in this report, this procedure carries the potential risk of symptomatic gallstone formation in the remnant gallbladder.9,12 Interestingly in the current series, similar to previous reports,13,14 we observed that in 66% of patients, the initial operating report did not document that STC was performed; this may be related to the fact that a remnant gallbladder may unintentionally be left behind if the cystic duct-gallbladder junction cannot be correctly identified.3,13 The incidence of unintentional incomplete removal of the gallbladder is unknown, and the incidence of stones in the remnant gallbladder varies widely, ranging from 0% to 15%.15,16 The incidence of symptomatic biliary disease after STC also remains uncertain, because of unawareness by the surgical team.13,14 The diagnosis of symptoms related to remnant gallbladder may be challenging, as the patients are labeled as having had their gallbladder already resected. As shown in Table 2, we found that the most common presentation of patients with remnant gallbladder symptoms is recurrent biliary colic. Therefore, a history of recurrent biliary colic similar to the pain experienced before the initial cholecystectomy should raise suspicion of a remnant gallbladder. Reviewing the operative records of the initial cholecystectomy may be helpful to determine the level of difficulty and findings at the initial operation. Consistent with previous reports, the incidence of more complex biliary pathologies, such as Mirizzi syndrome and choledocholithiasis, which may be missed by an abdominal ultrasound warrants the use of more advanced imaging modalities such as CT, MRCP, EUS, or ERCP (Figures 1 and 2). 17
Obviously, the treatment of choice for symptomatic remnant gallbladder cholecystitis is completion cholecystectomy of the remnant. While there are a few case reports on managing remnant stones with ERCP or extracorporeal shockwave lithotripsy, we believe, as others, that the surgical removal of the remnant gallbladder is the treatment of choice. This procedure can be technically demanding due to expected adhesions and distorted anatomy. Concors et al 13 reported that although redo cholecystectomy was initially attempted laparoscopically in few cases, it ultimately required an open approach in all cases. Rozsos et al 18 considered laparoscopic surgery to be risky and recommended that completion cholecystectomy should be performed through minilaparotomy. However, recent studies, similar to our series, have reported successful laparoscopic removal of a remnant gallbladder in institutions with advanced laparoscopic experience, with a near 0% conversion rate.19,20 The uniform resolution of symptoms in all of our patients following laparoscopic redo cholecystectomy is encouraging, along with a lack of major complications.
Obviously, it is difficult to draw conclusions based on such a small cohort, but due to the rarity of this condition, we doubt that large series will ever be available.
Nonetheless, this report contributes more information to the existing literature13,16,21,22 and underscores the importance of vigilance and clinical suspicion in the post-STC patient population.
In conclusion, post cholecystectomy, clinical history of recurrent biliary symptoms should raise the suspicion of a remnant gallbladder. Imaging studies are useful for establishing the diagnosis and providing a road map for redo surgery. Completion cholecystectomy for symptomatic remnant gallbladder can be safely performed laparoscopically with expected relief of symptoms. ERCP with remnant gallbladder and stones. ERCP—endoscopic retrograde cholangio-pancreaticography. MRCP showing remnant gallbladder filled with stones. MRCP—magnetic resonance cholangio-pancreaticography.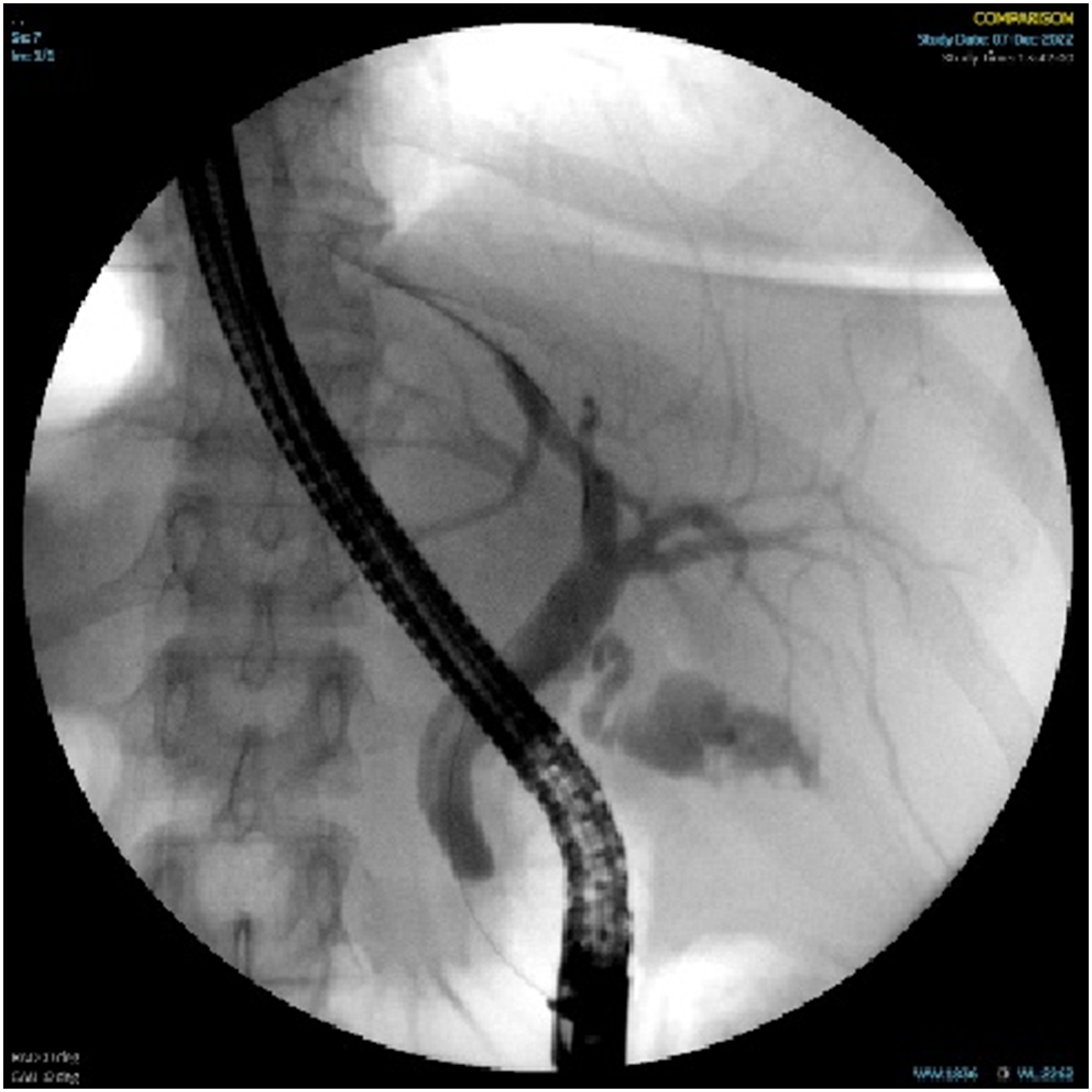
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.