
Abstract
Background
Open fractures have been associated with a higher risk of infection if antibiotics are not administered within 1 h of presentation in adult trauma patients. Time to antibiotic administration for open fractures is frequently used as a quality metric for trauma centers, but there have been no large studies evaluating this topic for pediatric patients.
Methods
The 2019 Trauma Quality Improvement Program dataset was queried for patients ≤ 16 years old with isolated open femur or tibia fractures undergoing operative intervention after blunt trauma. Patients transferred from another hospital were excluded. Pediatric patients receiving early antibiotics (EA) within 1 h were compared to patients receiving delayed antibiotics (DA) greater than or equal to 1 h from arrival. Multivariate logistic regression was used to evaluate risk of surgical site infection (SSI).
Results
There were 150 patients with open lower extremity fractures: 98 (64.9%) EA vs 52 (34.4%) DA. There was no difference in the rate of SSI between the 2 groups (EA: 1.0% vs DA: 1.9%, P = 0.65). There remained similar associated risk of infection after adjusting for lower extremity abbreviated injury scale >3, blood transfusion requirement, and vital signs on arrival (OR 0.62, 95% CI 0.04-10.24, P = 0.74).
Conclusions
Most pediatric trauma patients with open lower extremity fracture received antibiotics within 1 h of presentation. However, SSI was rare and the risk of SSI was not associated with antibiotic administration within 1 h. Therefore, timing of antibiotic administration for pediatric open lower extremity fractures should be re-evaluated as a quality metric.
Introduction
Open fractures among the pediatric population are rare, accounting for only 2% to 9% of all pediatric fractures.1-4 Among open fractures in children, one of the most common sites of injury reported is the tibia. 5 Infection rates following open fractures have been reported to increase with higher grades of open fracture, particularly Gustilo type III open fractures (eg, extensive soft tissue injury or any open fracture associated with vascular injury that requires repair) in adults.6,7 Open fractures in children differ in several ways as compared to adults. Anatomically, young children have a thicker and more vascular periosteum, and thus experience more rapid and reliable fracture healing as compared to adults.1,8 Additionally, infection rates in open fractures occurring in children have been reported to be much lower than rates in adults with Patzakis et al reporting overall infection rates of 1.8% in children vs 7.2% in adults.4,9,10
Despite the lower incidence of infection with pediatric open fractures, prompt administration of antibiotics has been demonstrated to be the variable most closely associated with reduction of infection rates in open fractures, including surgical site infections (SSI) in both adults and children.10-12 In the adult population, studies have demonstrated that open fractures are associated with a higher risk of infection if antibiotics are not administered within 1 h of presentation. 13 As such, the American College of Surgeons (ACS) Trauma Quality Improvement Program (TQIP) guidelines released in November 2015 recommend administration of intravenous antibiotics within 1 h of presentation. 14 However, there have been no large studies evaluating this practice for pediatric patients.
Therefore, this study sought to evaluate if antibiotic administration less than 1 h from arrival leads to a decreased rate of SSI for operative open lower extremity fractures, hypothesizing that pediatric trauma patients with open femur or tibia fractures undergoing operative intervention would have a decreased risk of SSI if antibiotics were administered within 1 h of presentation.
Methods
This study was deemed exempt by our local Institutional Review Board and a waiver of consent granted for use of a deidentified national database. A retrospective analysis was performed using the 2019 Trauma Quality Improvement Program (TQIP) database, which includes national data. In 2019, the TQIP added a new variable in the dataset indicating which patients with open fractures were started on intravenous antibiotic therapy and the timing of antibiotic initiation.
The 2019 TQIP database was queried for patients
Two groups were compared: patients receiving early antibiotics (EA) within 1 h of hospital presentation and patients receiving delayed antibiotics (DA) greater than or equal to 1 h from arrival. The primary outcome was any surgical site infection (SSI) including osteomyelitis, deep surgical site infection, and superficial surgical site infection. Secondary outcomes included other infectious complications including blood stream infection, urinary tract infection (UTI), and pneumonia.
Additional information collected included age, sex, body mass index (BMI), injury severity score (ISS), vital signs on arrival, vascular injuries to the leg (femoral vein/artery, popliteal vein/artery, anterior tibial artery, posterior tibial artery, and peroneal artery), and comorbidities that are more likely to be prevalent within a pediatric trauma population including attention deficit hyperactivity disorder (ADHD), diabetes, smoking, and substance abuse. Other outcomes measured include total hospital length of stay (LOS), intensive care unit (ICU) LOS, acute respiratory distress syndrome (ARDS), acute kidney injury (AKI), and compartment syndrome. Frequency statistics were performed for all variables of interest. A chi-square test and Mann-Whitney U test were used to compare categorical and continuous variables, respectively. Categorical data were reported as percentages, and continuous data was reported as medians with interquartile range or as means with standard deviation.
A multivariable logistic regression analysis was performed evaluating risk of SSI. These variables were carefully chosen after a review of the literature and discussion among coauthors.15-17 Covariates with statistical significance (P < 0.20) were then included in a hierarchical multivariable logistic regression model and the adjusted risk for SSI was reported with an odds ratio (OR) and 95% confidence intervals (CIs). All P-values were two-sided, with a statistical significance level of <0.05. All analyses were performed with IBM SPSS Statistics for Windows (version 24, IBM Corp., Armonk, NY).
Results
Demographics and Comorbidities of Pediatric Trauma Patients With Open Lower Extremity Fractures Stratified by Timing of Antibiotic Administration.
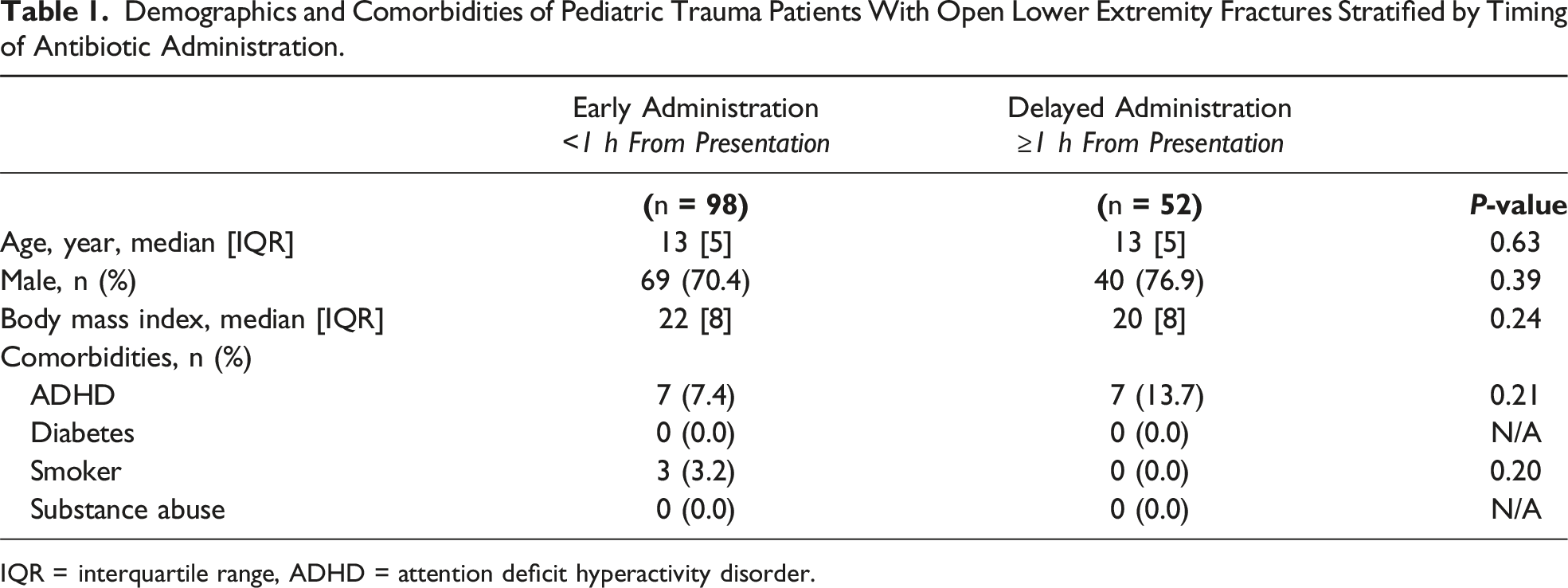
IQR = interquartile range, ADHD = attention deficit hyperactivity disorder.
Injury Profile and Vital Signs for Pediatric Trauma Patients With Open Lower Extremity Fractures Stratified by Timing of Antibiotic Administration.
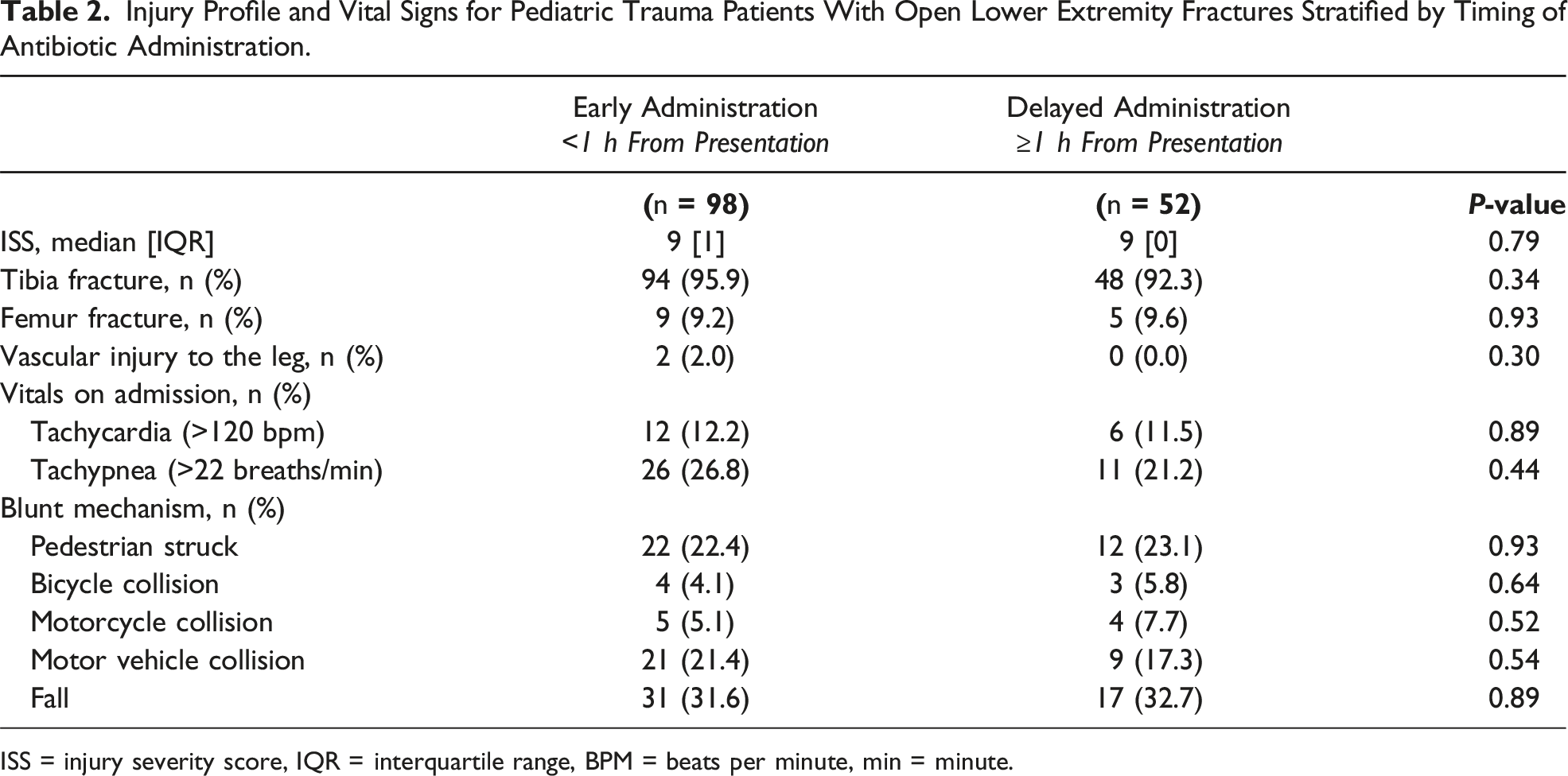
ISS = injury severity score, IQR = interquartile range, BPM = beats per minute, min = minute.
Clinical Outcomes of Pediatric Trauma Patients With Open Lower Extremity Fractures Stratified by Timing of Antibiotic Administration.
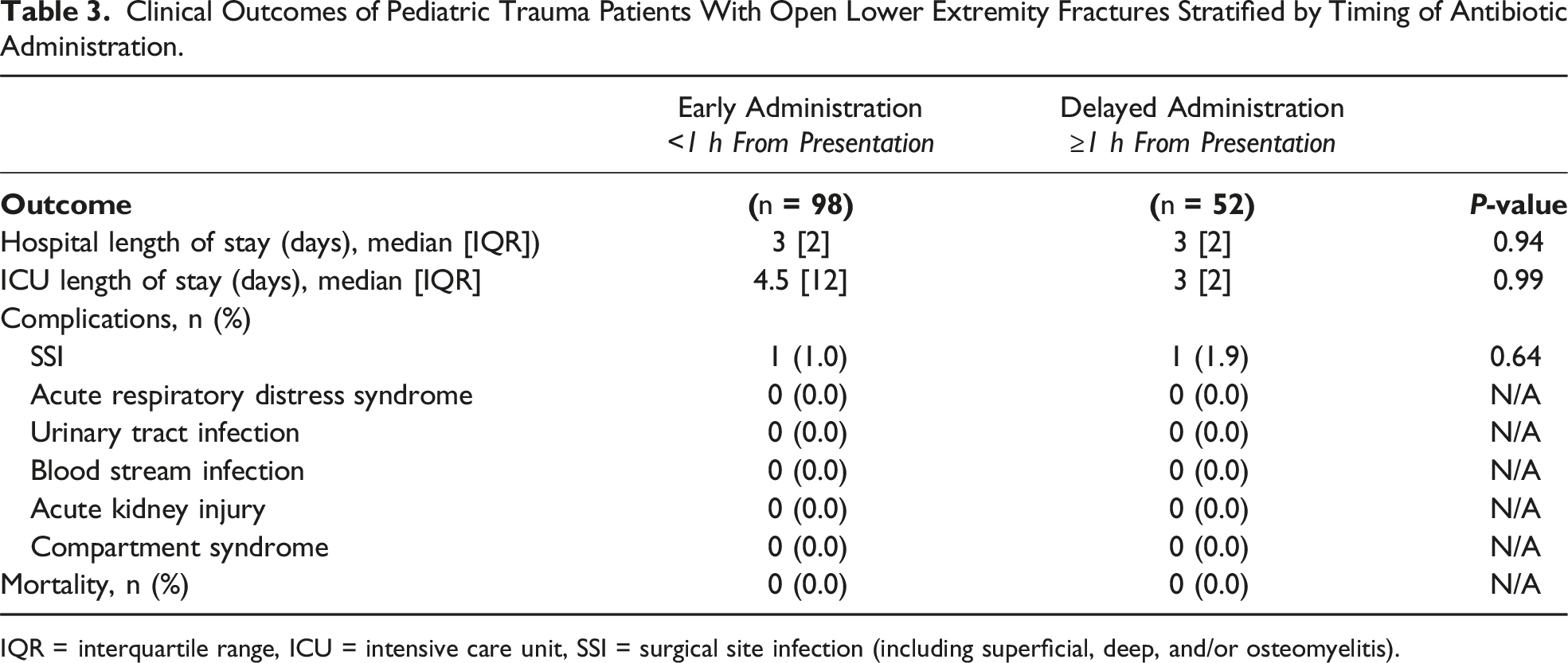
IQR = interquartile range, ICU = intensive care unit, SSI = surgical site infection (including superficial, deep, and/or osteomyelitis).
After controlling for vitals on admission, the severity of the extremity injury (using AIS), and blood product transfusion, there was no difference in the associated risk of SSI between those receiving EA and DA (OR 0.62, CI 0.04-10.24, P = 0.74).
Discussion
Antibiotics remain a mainstay of treatment of open fractures, with the goal of reducing risk of infection. Based on predominantly adult data, there has been a push to utilize administration of antibiotics within 1 h as a quality metric for pediatric open lower extremity fractures. However, contrary to the hypothesis, this national analysis found there was a similar rate and associated risk of SSI in the cohort receiving antibiotics within 1 h vs greater than 1 h from arrival.
Open fractures are by definition contaminated wounds, however the bacterial load and degree of contamination can vary greatly, both within a given Gustilo type of open fracture as well as with increasing severity of open fracture. Infection rates range from 0 to 9% for Gustilo type I fractures, 1% to 12% for Gustilo type II fractures, and 9% to 55% for Gustilo type III fractures in adult studies.6,10,18-24 Infection rates in children with open long bone fractures have been shown to be significantly lower than that of adults with similar fractures, with Chen et al reporting an overall SSI rate of 13.5% in children vs 21.3% in adults and Patzakis et al reporting overall infection rates of 1.8% in children vs 7.2% in adults.9,10 This contemporary analysis has demonstrated SSI rates to be similar for both EA and DA cohorts with each having an incidence of SSI less than 2%. This may partially be related to decreased comorbidities in the pediatric population as medical conditions such as diabetes and obesity have been demonstrated to be associated with increased risk of SSI in children.25-28 In addition, there is recently increased attention toward immediate local wound care/hygiene,29-31 use of bedside and/or operative washout,3,32,33 and timely administration of antibiotics.
With respect to the significance of early administration of antibiotics and the rate and risk of SSI, an adult population study by Lack et al reported that time from injury to antibiotics independently predicted infection for Gustilo type III open tibia fractures. 13 Their study of 137 adult patients with Gustilo type III open tibia fractures found that with increasing time to antibiotic administration there was an associated rise in infection rate: 6.8% for antibiotic prophylaxis within 1 h of injury vs 27.9% for antibiotic prophylaxis beyond 90-min (P = 0.01). 13 In contrast, our study has shown a similar rate and associated risk of SSI between EA and DA groups in a pediatric patient population. One potential explanation for the difference is the study by Lack et al only included patients with Gustilo type III fractures. Open fractures with higher Gustilo classifications (eg, type III) are associated with increased risk for infection despite the use of broad-spectrum antibiotics and aggressive surgical debridement.10,20,34 Thus, the use of early antibiotics may have a more significant impact with higher grade fractures, which represent a minority of pediatric open fractures. That said, the authors wish to assert that while administration within 1 h may not be an ideal overall quality metric, administration of antibiotics as early as possible still should be attempted as it may have a role in higher grade open fracture injuries.
There are several limitations to this study. First, the retrospective database design of this study means that there are potential limitations including misclassification and/or missing data. However, the TQIP database utilizes registrars with standardized training for data abstraction, ensuring that there is consistency and standardization among clinically abstracted data. 35 Moreover, TQIP includes numerous mechanisms that assure consistent, high-quality data collection such as training and continuing education for trauma registrars, data logic checks, assessment of outlier values, and internal as well as external data validation on site visits where necessary. 35
Additionally, despite using a large national database, the overall sample size was still relatively small, as was the incidence of SSI. Due to the low sample size in this study, we were not adequately powered to confidently demonstrate equivalence in this scenario. The number of patients we would need to show a difference in risk reduction with timely administration of antibiotics would be substantial if the baseline incidence of SSI is truly 2%. However, this highlights how difficult it would be to obtain Level I quality of evidence (eg, a systematic review of multiple randomized control trials). Also, this database lacks information on the specific antibiotic agent used and duration, variables which have been shown to affect SSI in prior studies.10,36,37 Moreover, we did not include other risk factors for infection, such as the time to surgical fixation, method of fixation, and operative details such as intraoperative blood loss and body temperature. Finally, an important limitation is the lack of data regarding the Gustilo classification within TQIP, which as previously mentioned is a significant risk factor for SSI.18,20,24 However, we did use the AIS grade as a marker of injury severity (including soft tissue damage) to at least partially control for injury severity.
Conclusions
This national analysis demonstrated that antibiotic administration within 1 h for pediatric trauma patients with open femur/tibia fractures occurred commonly, however, was not associated with decreased rate or associated risk of SSI. Further data with increased power is necessary to definitively evaluate if there is a benefit with early administration of antibiotics for pediatric trauma patients with an open fracture, and thereby if this should remain to be a quality metric.
Footnotes
Author Note
Presented at the Pediatric Trauma Society 8th Annual Meeting on 11/03/2022.
Author Contributions
All authors contributed to the study conception and design. Data collection was performed by Areg Grigorian. Statistical analysis was performed by Areg Grigorian. Critical review of the data was performed by all authors. The first draft of the manuscript was written by Marlene Jacobo and Jeffry Nahmias and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
This study was approved by each participating site’s Institutional Review Board and deemed exempt from need for consent.
Data Availability Statement
Data can be made available upon request.