
Abstract
Background
Antibiotic misuse extends beyond clinical outcomes, imposing significant financial, operational, and environmental burdens on health care systems. Despite guidelines advising against antibiotic prophylaxis for elective low-risk laparoscopic operations, clean head and neck, and soft tissue procedures, many surgeons continue to use them. We performed a cost and environmental waste analysis at our institution resulting from nonadherence to guidelines.
Methods
A retrospective chart review was performed at a single institution between January 2022 and March 2023. All patients undergoing elective diagnostic laparoscopy, soft tissue excisions for presumed benign disease, thyroid, and parathyroidectomy operations were included. Antibiotic costs were obtained from the hospital charge pharmacy. Waste was estimated by weighing the bottles and syringes used to administer the antibiotics.
Results
From January 2022 to March 2023, 137 patients who underwent the defined operations were identified. 38% (n = 52) underwent lipoma excisions, 33% (n = 46) thyroidectomy, 11% (n = 15) parathyroidectomy, 9% (n = 12) diagnostic laparoscopy, and 9% (n = 12) other soft tissue excision. 94% (n = 129) of cases were classified as clean and 6% (n = 8) were classified as clean-contaminated in the operative report. Prophylactic antibiotics were administered to 92% (n = 126) of patients, with 6% (n = 8) receiving an additional intraoperative dose. Cefazolin was used in 90% (n = 119) of cases, followed by Cefoxitin 1% (n = 1) and Clindamycin 1% (n = 1). Adherence to guidelines could have saved US$3279 and prevented £23 of waste.
Discussion
A significant number of clean cases received prophylactic antibiotics, reflecting poor adherence to clinical practice guidelines. Improving antibiotic stewardship can reduce costs and environmental waste.
• Administration of unnecessary perioperative antibiotics outside established guidelines is common and confers financial and environmental waste impact. • Adherence to evidence-based antibiotic use guidelines can reduce health care costs, minimize waste production, and promote sustainable health care practices.Key Takeaways
Introduction
Much research has been performed evaluating the compliance to perioperative antibiotics and the prevention of surgical site infections; however, there are very few studies looking at compliance with antibiotic guidelines on the reverse aspect—cases where antibiotics are not recommended but still given. These situations represent an understudied area in terms of adverse environmental impact and unnecessary cost. The pharmaceutical industry is estimated to generate more greenhouse gas emissions than the automotive industry, and the production of antibiotic drugs is resource- and energy-intensive. 1 The majority of pharmaceutical waste, including antibiotics, are incinerated, leading to additional greenhouse gas emissions. 2 Antibiotic overuse can therefore exacerbate the environmental impact of the health care sector, which is estimated to be responsible for 8.5% of all US greenhouse gas emissions. 3
Joint guidelines from the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Surgical infection Society, and the Society for Healthcare Epidemiology of America state that antibiotic prophylaxis is not required for clean surgical procedures of the head and neck, such as thyroid or parathyroid operations, or for elective, low-risk laparoscopic cases. 4 While these guidelines don’t address elective, clean soft-tissue excisions, it is generally accepted that antibiotics are not indicated for these cases as well. 5 While surgeons may continue to give antibiotic prophylaxis in these cases with the perception that they may circumvent surgical site infections (SSIs), the reality is that contemporary evidence demonstrates that antibiotic prophylaxis in clean cases has no effect on whether or not an SSI develops. 6 As such, it becomes essential to consider the broader consequences of continued nonadherence to current guidelines including the environmental toll of unnecessary pharmaceutical waste and the associated economic costs.
We hypothesized that perioperative antibiotics were being utilized frequently and in opposition to current guidelines for clean surgical procedures at our institution. The purpose of this study was to quantify the environmental and financial impact correlated with this unnecessary antibiotic use.
Methods
Study Design
A retrospective chart review was conducted under IRB approval on adult patients who underwent ambulatory clean operations between January 2022 and March 2023 at Harbor-UCLA, a 570-bed tertiary-care safety-net hospital. Patients included in the study underwent diagnostic laparoscopy, thyroidectomy, parathyroidectomy, as well as clean-soft tissue excisional biopsies. Demographic information including race/ethnicity, gender, and comorbidities was collected. Wound classification was extracted from operative notes using the Centers for Disease Control and Prevention (CDC) classification system. 7 Operations which met criteria for being clean but reclassified as clean-contaminated postoperatively by the surgeon were included in the study. Prophylactic antibiotic use was obtained from anesthesia records. Information regarding the 30-day postoperative infection, emergency department visits, and readmissions due to infection was gathered. General 30-day emergency department visits and admissions not related to infections were not included to maintain focus on outcomes relevant to antibiotic use. Antibiotic costs were obtained from the institutional pharmacy. Cefazolin had a cost of US$12 per gram, Cefoxitin had a cost of US$9 per gram, and Clindamycin had a cost of US$6 per gram. Waste was quantified by weighing syringes and antibiotic bottles used for administration. Bottles had a weight of £0.05 each and syringes £0.02 each.
Results
Patient Demographics, Comorbidities, and Outcomes Overview
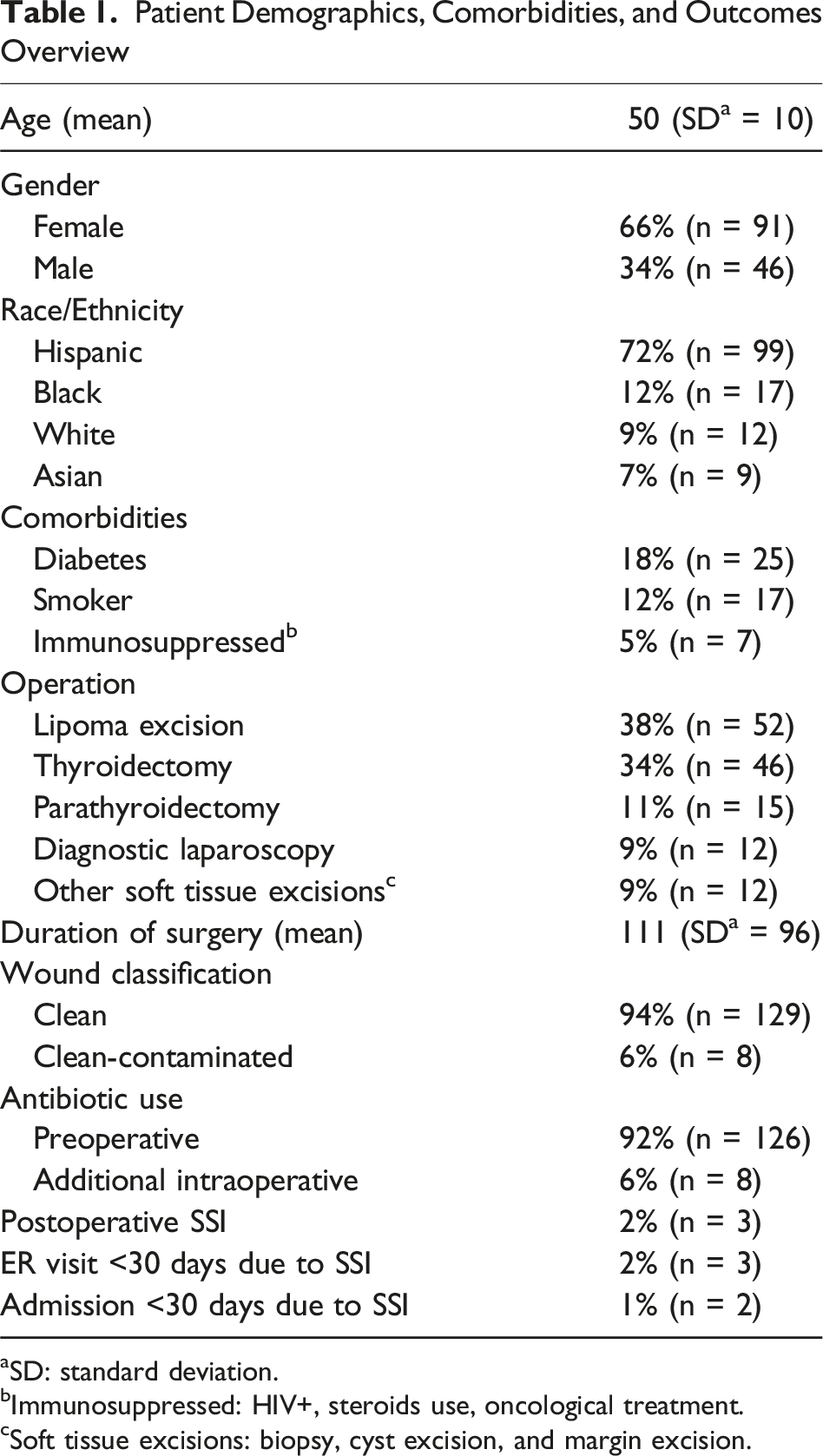
aSD: standard deviation.
bImmunosuppressed: HIV+, steroids use, oncological treatment.
cSoft tissue excisions: biopsy, cyst excision, and margin excision.
Among the operations performed, excisional biopsy of a lipoma was the most common procedure accounting for 38% (n = 52) of cases, followed by thyroidectomy at 34% (n = 46), parathyroidectomy at 11% (n = 15), diagnostic laparoscopy at 9% (n = 12), and other soft tissue excisions (including cyst excision, biopsy, and margin excision) at 9% (n = 12) (Table 1). The mean duration of the operations was 112 min (SD ± 96). The majority of operations were classified as clean 94% (n = 129). The remaining 6% (n = 8) were classified as clean-contaminated at the end of the case. Upon reviewing the operative text, it was not clear why these 8 cases were re-classified as clean-contaminated. Preoperative prophylactic antibiotics were administered to 92% (n = 126) of patients, while 6% (n = 8) received an additional intraoperative antibiotic dose. Cefazolin was the most commonly used antibiotic in 91% (n = 124) of cases, followed by Cefoxitin and Clindamycin, which were each used in 1% (n = 1) of cases. Postoperative infections were observed in 2% (n = 3) of the study population, consisting of 1 seroma with Enterobacter spp. growth and 2 surgical site infections involving Enterobacter spp. and Staphylococcus aureus, respectively. All infections were superficial and occurred in patients whose operations were classified as clean and had received prophylactic antibiotics. All three patients presented through the emergency department within 30 days postoperatively for evaluation of infection. Of these 3 patients, 1% (n = 2) required hospital admission.
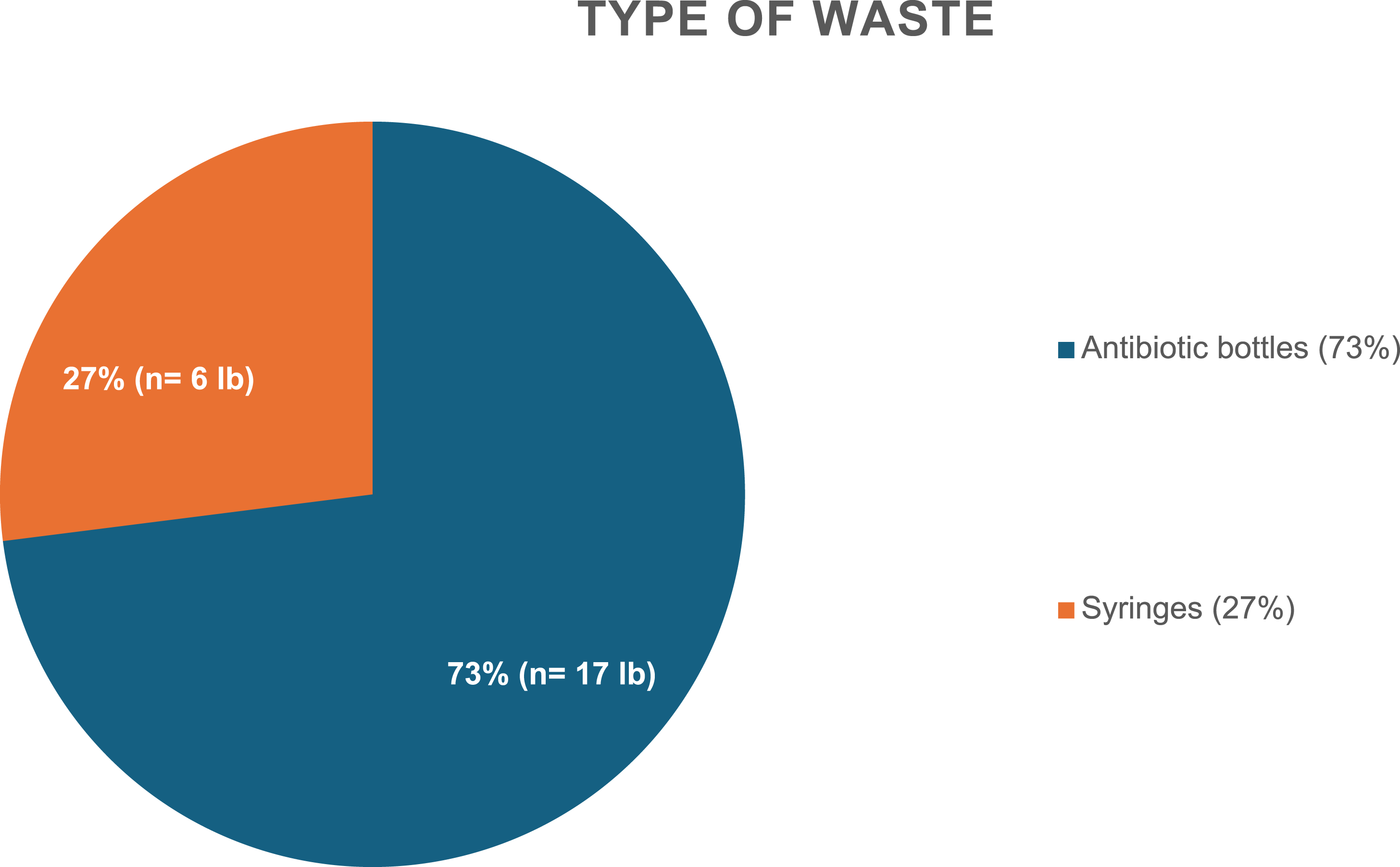
During the study period, antibiotic use amounted to 272 g of Cefazolin, 2 g of Cefoxitin, and 600 mg of Clindamycin, costing US$3279 (Figure 1). The waste generated from nonadherence to guidelines amounted to £23, with 73% (n = 17) attributed to antibiotic bottle waste and 27% (n = 6) to syringe waste; Cefoxitin and clindamycin were packaged in small plastic bags for which the weight was negligible and not included in the final weights (Figure 2). Cost of Antibiotic Usage Waste of Antibiotic Use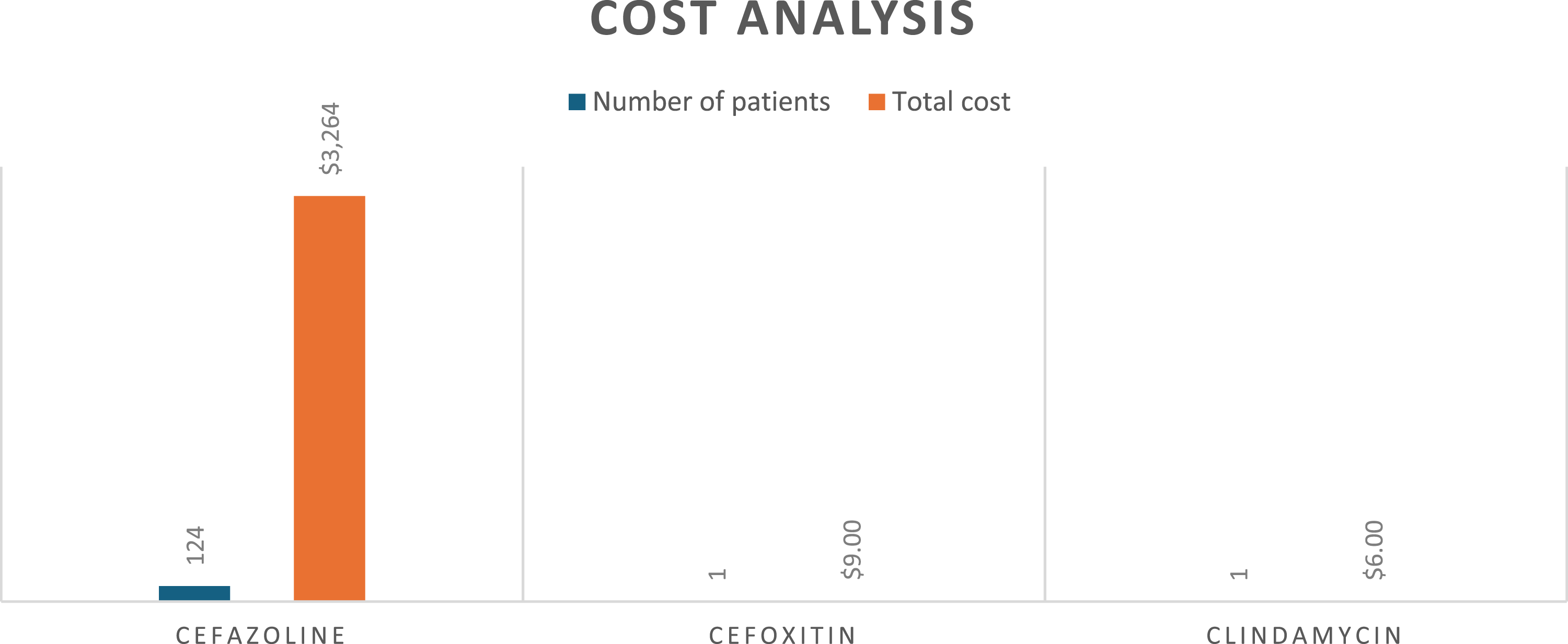
Discussion
Despite guideline recommendations against antibiotic prophylaxis for clean cases, many surgeons continue to give antibiotics unnecessarily. At our institution, we found that over 90% of elective, low-risk, clean operations received preoperative antibiotics inappropriately with some patients also receiving an additional intraoperative dose. Among the 126 patients who received prophylaxis, only 7 had a relative justification based on a history of receiving immunosuppressive medications. 4 The inappropriate use of antibiotics is a multifaceted problem, impacting institutions by increasing costs, the environment through production, waste, and disposal, and patient care by contributing to multidrug resistance. 8
We show in our study that adherence to guidelines could result in an institutional savings of US$3279 and avoid £23 of waste in the form of plastic syringes, pouches, and glass bottles in a little over a year. While these numbers are modest, when applied across large health care systems the cumulative effect adds up. Operating rooms are one of the largest contributors to hospital waste, accounting for 20% to 30% of the total waste produced. 2 The effect of producing and disposing of plastic waste in this modern era cannot be minimized: it is estimated that 2000 garbage trucks worth of plastic are dumped into the world’s oceans, rivers, and lakes every day. 9 This mass production of plastic has significant human health implications; as an example, microplastics found in carotid artery plaques have been implicated as a risk factor for myocardial infarction, stroke, and death. 10
Aside from the problem of waste volume, we were unable to calculate the greenhouse gas emissions that would result from the disposal of this waste, but we know that this is not insignificant. Unlike general waste, pharmaceutical waste must undergo specific disposal processes which has a high environmental impact. 11 At our facility, pharmaceutical waste is collected and transported in a diesel truck to a waste processing center nearly 500 miles away for incineration. This impact of disposal of pharmaceutical waste is in addition to the more than 48.55 billion kg of carbon dioxide already produced during pharmaceutical manufacturing. 1 Additionally, the cost of hazardous waste disposal can range from US$2 to US$20 per pound, depending on the type of waste and the method of disposal, adding to the total costs. 2
The future challenge is convincing surgeons to avoid using unnecessary prophylactic antibiotics. One major factor contributing to antibiotic misuse is the misperception that prophylaxis is low risk yet effective in preventing SSIs.6,12 Education that prophylaxis does not impact SSI rates in certain cases may help improve adherence to guidelines. 13 In our study, for example, all patients who developed SSI had received prophylaxis. Another contributing factor may be the discretion granted to clinicians in current guidelines, which often leave the decision to administer antibiotics open to individual judgment. 4 While this flexibility aims to account for unforeseen intraoperative circumstances, it can lead to the inappropriate administration of antibiotics in cases that do not warrant prophylaxis. In our study, several cases that were ostensibly clean were later reclassified, seemingly indiscriminately, as clean-contaminated at the conclusion of the surgery, a determination that should not retroactively justify prophylaxis administration. Interventions such as decision-support tools or automated prompts in electronic health records (EHRs), along with anti-microbial stewardship programs and ongoing education on the harms of indiscriminate antibiotic use, may help close the gap between guidelines and clinical practice. Studies have demonstrated the benefits of EHR alerts in areas such as medication allergies and test result follow-up. 14 Similar strategies may be viable options to improve adherence to antibiotic prophylaxis guidelines.
While our study provides a very small insight into the cost and waste implications of antibiotic misuse, our larger aim is to raise awareness and offer a broader perspective on its importance. Aside from antibiotics, unnecessary tests, labs, and imaging studies all have the same global impacts. Efforts should be made nationally to identify more areas for improvement regarding unnecessary health care ordering in order to lead to more cost-effective care and environmental waste reduction.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.