
Abstract
Historically, surgery has been considered an inherently “masculine” profession. This persistent stereotype has led to gender inequality in currently practicing surgeons, despite gender parity of newly admitted medical students in North America. Since women began practising medicine in the 19th century, these norms began to be challenged in tandem with the suffragette movement. In the United States, United Kingdom and Canada, pioneering female physicians and surgeons worked together to establish spaces where women would be welcomed and mentored the next generation of female surgeons. In this essay, I highlight prominent women physicians and surgeons that have contributed to the presence of women in the operating room through mentorship.
The Surgeon “myth”
The following riddle is used as an example of heuristic bias. A man and his son are in a terrible car accident. Tragically, the father does not survive, and the son is urgently transported to the hospital for surgery. The surgeon at the hospital takes one look at the child and says, “I can’t operate on this patient, he’s my son!” How is this possible? Once it is revealed that the son’s mother is the surgeon, we realize we have fallen trap to a heuristic bias.
Despite the number of female medical students increasing over the last four decades, and now surpassing their male counterparts, women pursuing surgical specialties are a minority. 1 Although there has been a notable growth in women pursuing obstetrics and gynecology, ophthalmology, and otolaryngology, other surgical specialties such as cardiothoracic, orthopedic, and urology remain underrepresented. 2 Many factors may explain this gender parity in surgical specialization, including the subconscious characterization of a stereotypical surgeon. In her novel “Cold, Hard Steel: The Myth of the Modern Surgeon,” Dr Agnes Arnold-Forster provides a well-characterized portrayal of this mythical stereotype. She writes of the modern surgeon as “mostly male, authoritarian, and paternalistic, […]. He cuts first, asks questions later, and is never in doubt.” 3
When women began pursuing surgical careers in the 1800s, surgery was seen as an inherently masculine activity. In 1859, an author for the British Medical Journal ironically poses the following scenario: “Imagine the Semiramis of surgery, a Fergusson in woman’s outward guise, amputating a thigh, or removing a diseased jaw or elbow-joint, […]. Imagine some fair and amiable damsel, […], poring with inquisitive eye over a collection of ulcerated Peyer’s patches or a piece of softened cerebral substance, […]. Call to mind all things that are done in the ordinary course of hospital duties, […] and imagine, good reader, if you can, a British Lady performing them.”
4
The author continues by stating, “Is it compatible with the attributes of woman, that she should arm herself with a medical education and medical diplomas, and put herself forward to practise medicine? Certainly not.” 4 Another piece in Englishwoman’s Domestic Magazine by Maria Susan Rye states that Dr Elizabeth Blackwell, the first American female physician, had a gender incompatible with the brutal nature of surgery. 5 In addition, others concluded women could not mentally move on from these gruesome cases once exposed, which would affect their ability to care for other patients. 6 These norms created barriers for women pursuing surgical careers, as many were forced away from treating their patients surgically because of this perceived gender incongruence. 7
Despite this perception, many women in the Western world have worked to change this ideology. Suffragettes helped promote the equality of women in all aspects of society, while others moved to another country that would allow them to train in surgical specialties. Some would establish women-led institutions and hospitals that would train and hire female surgeons. 8 Regardless of their method, women worked cooperatively to challenge the gender norms of surgical practices. Part of this cooperation included providing mentorship to the next generation of female surgeons. In this essay, I highlight the legacy of prominent female physicians and show mentorship as an effective tool to challenge the entrenched gendered norms of surgical practices.
Dr Elizabeth Blackwell: a Reckoning Force to the Field of Medicine
In 1849, Dr Elizabeth Blackwell became the first woman to earn a medical degree (Figure 1).
9
Her passion for medicine was ignited after the passing of a friend who believed she would have suffered less from her metastatic cancer had a woman treated her.
10
Blackwell initially wished to pursue a career in surgery, as outlined in a letter addressed to her cousin in 1849. She expressed a desire to become an accomplished obstetrician, but could not pursue it further due to permanent vision loss following a severe eye infection.
11
Although saddened by her own circumstances, Blackwell was not deterred from her own ascribed mission statement: to ensure the presence of women in the operating room.
12
Dr Elizabeth Blackwell, photographed in 1888 by W.A. Thomas.
While lecturing at the Marylebone Institute, she advocated for the need for female doctors, and more notably, female surgeons. 4 Through her teachings, she would dissuade her younger colleagues from adopting “masculine” characteristics to be better accepted into surgical environments. Blackwell deliberately contradicted this ideology and would criticize her mentees who would adopt these behaviors in the pursuit of their goals. 13 Moreover, Blackwell’s philosophy to combat gender norms had been prevalent since starting her medical studies, as evidenced by her refusal to study abroad in a more accepting environment compared to the United States. By remaining in the US, Blackwell hoped to challenge the perception of women pursuing medicine in her program. 14
As women integrated themselves into medicine, the development of women-only institutions became prominent. Although these institutions were a critical pillar in allowing and supporting women while they pursued medical training, Blackwell found the quality of these programs to be far worse than those at male institutions. She rectified this discrepancy by developing a high-standard educational program at the New York Infirmary for Women and Children in 1853 (Figure 2).
15
High-quality training for female students was a fundamental step in the training and legitimization of female physicians. Illustration of female medical students attending a lecture at the New York Infirmary. Frank Leslie’s Illustrated Newspaper. April 16, 1870.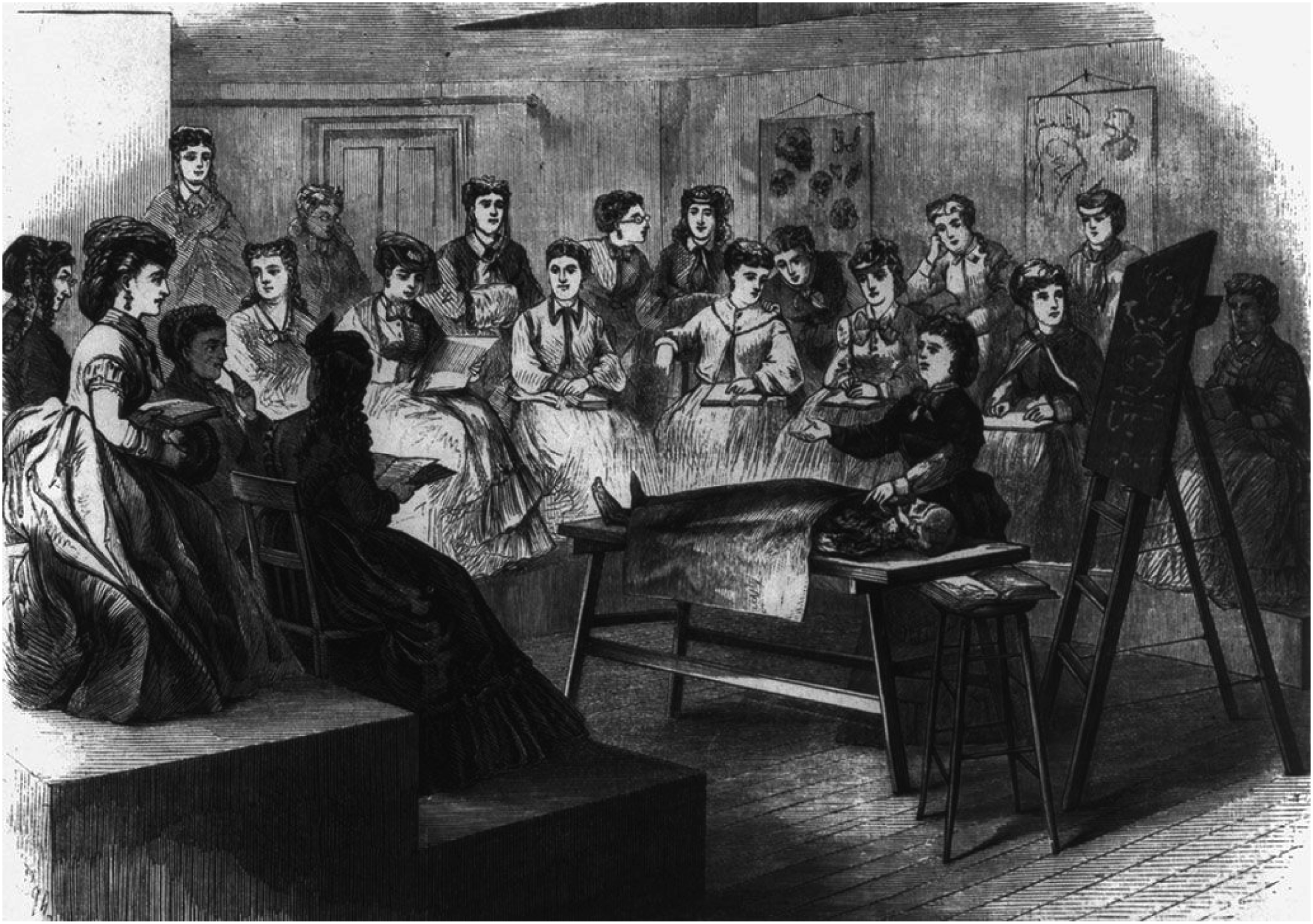
Elizabeth Blackwell’s dedication to promoting female physicians created a path that allowed her sister to thrive. Dr Emily Blackwell was the second female physician in the United States in 1854 and pursued a more surgical practice. 16 Because Elizabeth Blackwell had cultivated a positive environment for women to learn, Emily Blackwell was able to focus on developing her clinical expertise. She was regarded as a compassionate surgeon with highly refined skills in the operating room. 16 Emily Blackwell would ultimately become a professor of obstetrics at the New York Infirmary until her retirement in 1900. In 1910, both Blackwell sisters would pass. 15 By the time of their deaths, 6% of all practicing physicians in the United States were women. 17 This is a testament to Elizabeth Blackwell’s trailblazing legacy, which began with the firm belief that women should, and could, pursue medicine.
The Immediate Influence of Elizabeth Blackwell on the First Generation of Female Surgeons
Dr Elizabeth Garrett Anderson was the first British female physician in 1865. Six years before her accreditation, Anderson attended Elizabeth Blackwell’s lectures at the Marylebone Institute. She would cite these lectures as a fundamental source of inspiration for her pursuit of medicine. 18 Although Anderson was not personally interested in surgery, describing the surgical field in a letter as “not my line,” she recognized the need to support other women who wished to become surgeons. 19 Like Elizabeth Blackwell, Anderson believed women had to maintain and express their femininity to validate its congruence with surgery. During her own time in the operating room, she described to friends and family that she would wear “a dress pleasing to others around” to assert her feminine identity. 20
In 1866, Anderson founded the New Hospital for Women in London (Figure 3). This institution, similar to its predecessor in the United States, aimed to educate and support women wishing to pursue medical training that were rejected from male-only institutions.
21
This new environment specifically for women, and developed by women, allowed aspiring female surgeons to practice and build their confidence in the operating room.
22
Anderson’s sister and famous suffragette, Millicent Garrett Fawcett, writes the establishment of New Hospital for Women proved “the fallaciousness of the old-fashioned idea that women could not possibly do the work of surgeons.”
23
The New Hospital for Women site on Euston Road, opened in 1890 (Wellcome Collection).
Upon Anderson’s retirement in 1893, Dr Mary Scharlieb took over as Senior Surgeon at the New Hospital for Women.
24
Scharlieb was initially inspired to pursue medicine after moving to Madras, India. While in India, she was exposed to horrific postpartum practices by male doctors, leading to high rates of maternal death. She realized many of these deaths had been preventable with adequate regard to maternal health. Vowing to make a difference, Scharlieb enrolled at the Madras Medical College where she obtained accreditation in medicine, surgery, and midwifery (Figure 4).
25
Dr Mary Scharlieb in Elstree, Hertfordshire (Wellcome Collection).
Due to personal health issues, Scharlieb returned to London in 1878 after 12 years of practice. She hoped to create a program that would send aspiring female doctors to practice in India, knowing that entrenched societal norms would continue to limit women wishing to practice medicine in England. Her efforts were met with numerous critics, including a surgeon at Guy’s Hospital who challenged her directly by exclaiming: “I entirely disapprove of women becoming doctors and will do nothing to further your wishes.” 26 Public disapproval of Scharlieb’s medical endeavors were further echoed by Queen Victoria, who was famously against women practicing medicine in general. In an attempt to change her perspective, Scharlieb attended a lunch at Windsor Castle. In discussions with Queen Victoria, Scharlieb described her grueling experience in India and effectively advocated the need for female doctors when caring for female patients. By the end of the meeting, Scharlieb successfully convinced England’s most influential figure of the merits of her proposed plan. 26
Scharlieb returned to India in 1883 and established the Royal Victoria Hospital in 1884. 27 She recruited Dr Mary Pailtrope to become the hospital’s medical officer. Pailtrope was a recent graduate from Cambridge University in mathematics, medicine, and surgery. Scarlieb took Pailtrope under her wing, helping her develop both her clinical skills and fluency in Hindi to better serve the population in India. 28
In 1887, Scharlieb once again returned to England due to the ongoing deterioration of her health. Keen to establish a practice in London, she sought guidance from Elizabeth Anderson, who was the Dean of the London School of Medicine for Women at the time. She appointed Scharlieb as a lecturer of midwifery. Through Anderson’s help and guidance, Scharlieb continued to develop her legitimacy as a surgeon in England. In 1893, she became Senior Surgeon at the New Hospital for Women. 29 In 1902, Scharlieb would become the first woman to be appointed department head at a non-woman specific institution as head of gynecology at Royal Free Hospital. 30 Upon Scharlieb’s passing, her legacy was irrefutable. Dr Jane Walker, a colleague and fellow friend, would write in her obituary that “She was a most beautiful operator. […] almost [in a] commonplace manner that it seemed, even at the very beginning, to be the most ordinary thing in the world for a woman to be doing big abdominal surgery”. 31 Anderson’s daughter, Dr Louisa Garrett Anderson, added “Her surgical reputation was an immense asset to the medical women’s movement.” 31
Through her mentorship from Anderson, Scharlieb developed a way for women to thrive in surgery by actively creating spaces where they could practice, while also guiding newly enrolled and motivated female students. Dame Louisa Aldrich-Blake, the first British woman to qualify as a Master of Surgery, pioneered the concept of treating rectal cancers with surgical resections. 32 Dr Ethel Vaughan-Sawyer used the controversial Wertheim’s technique to treat cervical carcinomas. 33 Both surgeons trained at New Hospital under Dr Scarlieb’s guidance and are a testament to her valuable and enduring mentorship.
A Canadian Legacy Mirroring Its British Counterpart
Similar advancements promoting female representation in surgery were occurring concurrently in Canada. Dr Jennie Smillie Robertson, commonly known as Dr Smillie, would become the first female surgeon in Canada in 1909. 34 She expressed a desire to pursue medicine from an early age. When speaking to her friend, Dr Margaret Donnell, Smillie said, “When I was five, I asked my mother if women could be doctors. She told me they could and from then on I knew that is what I would do.” 35 Upon graduating medical school, she completed a surgical internship at Women’s Medical College in Philadelphia. She returned to Toronto following her surgical training, and soon found that no practicing surgeon was willing to work with her. She then returned to Philadelphia where she worked alongside female surgeons for six months. Smillie describes that her training in Philadelphia “did wonders for [her] confidence,” citing that working alongside like-minded women helped her see herself as a surgeon. 36
Later, she returned to Toronto and was met with a similar problem: no hospitals would authorize female surgeons to have operating privileges. Instead of being discouraged, she worked around this active discrimination by performing surgeries in her patients’ homes. During this time, Smillie was accredited for performing the first major gynecological surgery in Canada, in which she removed an ovarian tumor on the kitchen table of her patient’s home. 35
Unfortunately, Smillie’s experience of gender discrimination was not unique. Other qualified female physicians at the time found it impossible to establish a practice in Toronto. Many of these women, including Smillie, came together to establish the Women’s College Hospital in 1911 (Figure 5).
36
Women’s College Hospital had a purpose “to provide for women, medical and surgical care by physicians and surgeons of their own sex; to furnish opportunities for women medical graduates to continue their studies in all branches of medicine”.
37
What initially started as a rental property for female physicians to practice would later grow into one of Toronto’s most innovative and pioneering institutions. By 1961, there were 80 practicing physicians and surgeons at the hospital.
38
In the same year, the Women’s College Hospital would be integrated as a fundamental site of training and care as part of the University of Toronto.
36
Female volunteers raising funds for the Women’s College Hospital. (Miss Margaret Robins Archives of Women’s College Hospital).
The Women’s College Hospital would become a critical incubator for future extraordinary female surgeons to train and lead. In 1915, Dr Minerva Reid became the first appointed female Chief of Surgery in North America at Women’s College Hospital.
39
Dr Jessie Catherine Gray, dubbed Canada’s “First Lady of Surgery,” became the first woman to obtain the degree of a Master of Surgery in 1939, the first woman to be accepted into a surgical residency program in 1940, and the first women to be awarded a Fellowship of the Royal College of Surgeons in 1941 (Figure 6).
40
At the time, she was considered one of the top four surgical oncologists in North America.
40
In 1946, she was appointed as the Chief of Surgery at Women’s College Hospital, where she would teach and mentor the next generation of female surgeons.
40
In 1954, Gray was honored with the Elizabeth Blackwell Award, an homage to the original pioneer of promoting women in the operating room.
41
By her retirement in 1965, Gray became the first woman to be appointed onto the Science Council of Canada.
42
Gray was actively involved in teaching at the University of Toronto. In her obituary, it was written that “Her students loved her. She was dynamic, cheerful and forthright with a great sense of realism and self-discipline.”
43
Dr Jessie Gray (seated) with colleagues in 1956. (Miss Margaret Robins Archives of Women’s College Hospital).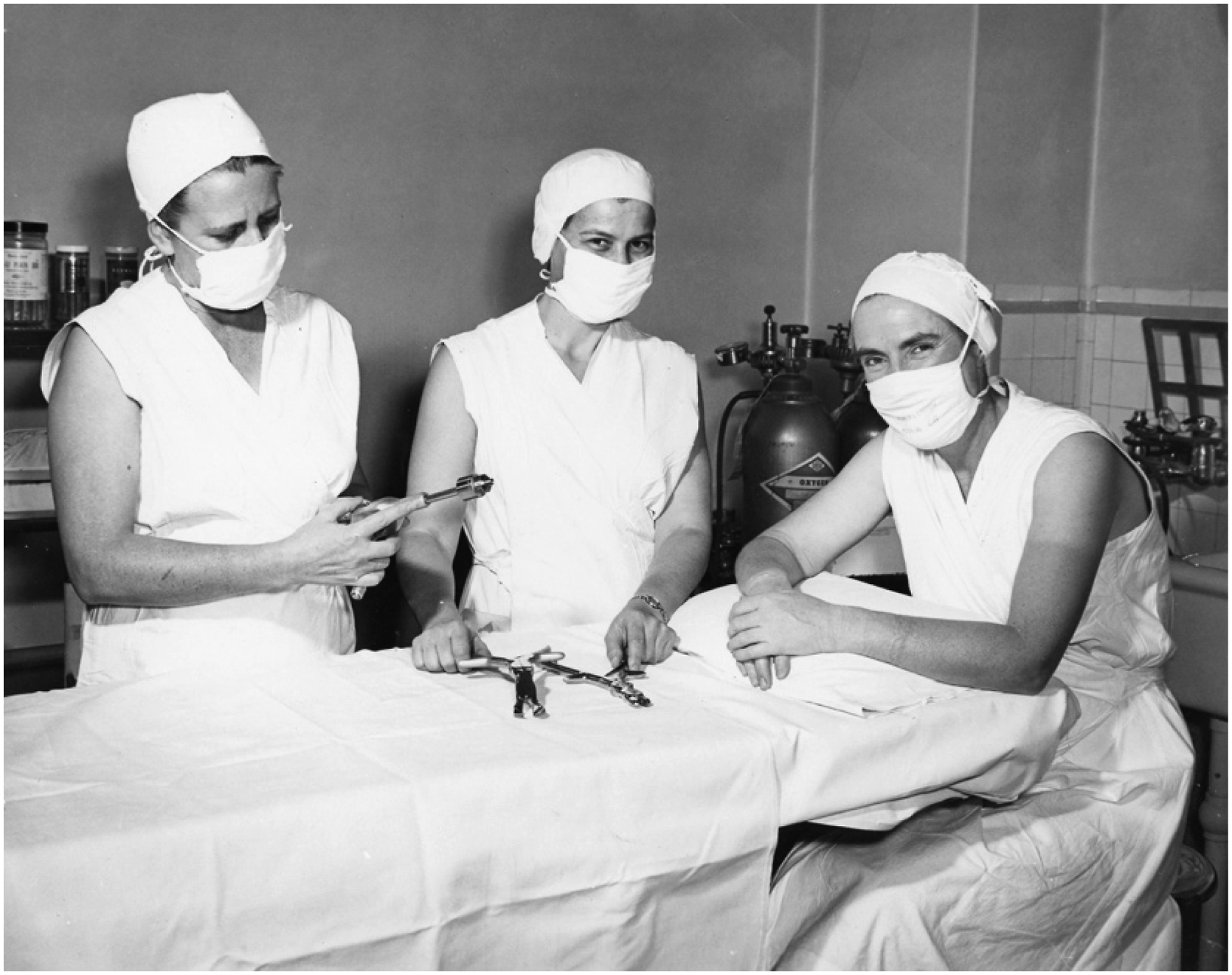
Despite Gray’s undeniable achievements, barriers remained. In 1980, Dr Anne Elizabeth Noelle Grace became the first female pediatric surgeon in Canada. 44 After obtaining her medical degree at Western University in 1965, Grace embarked on a surgical residency program at McGill University. While training at the Montreal General Hospital, she worked alongside her mentor, Dr Carime Emilia Isa Isa, the first female surgeon in the Dominican Republic.44,45 Claude Adams, a journalist at the Montreal Gazette, wrote of his experience shadowing Grace and Isa Isa for a routine operation at the Montreal General Hospital. He described his previous assumptions of what the “ideal” surgeon was supposed to resemble, citing the character Dr Ben Casey from a popular television show from the 1960s. Casey was a young but intense neurosurgeon who was able to save his patients from the brink of death. While describing his experience with Grace, he writes, “[They] began to chip away at the Ben Casey myth. […]. Dr Grace […] erased years of TV-induced fantasy from my mind. […]. It was nothing less than the shattering of an illusion”. 46
Dr Nancy McKee, after an internship at the Royal Victoria Hospital in Montreal, would later become the first female plastic surgeon in Canada. 47 She described her residency to be particularly challenging in regard to her peer relations. She was actively picked on due to her gender and was made to seem as if she had taken “a man’s spot” in plastic surgery. 48 This did not deter her ambition, and instead McKee had a fulfilling career as a plastic surgeon.
In 1979, she would become the first women to join the Division of Plastic, Reconstructive and Aesthetic Surgery at the University of Toronto. 49 In addition, she was credited with performing the first penile replantation in Canada in 1980. 47 She was a lifelong mentor to the future generation of surgeons throughout her career. Dr Christopher Forrest writes in her obituary that “she continued to […] mentor students from medicine and other health disciplines. Her enthusiasm for attempting to uncover the potential of any student she interacted with never waned.” 49
Upon her death, a fund was created in her name to support educational and research endeavors within the domain of plastic surgery. 50 Part of the funds was used to create annual lectures to promote equity, diversity, and inclusion for plastic surgery trainees. 48 At her death, she left behind three children. All of them would become physicians themselves, and are a testament to her enduring mentorship. 48
Conclusion
From Dr Elizabeth Blackwell to all women surgeons practicing today, the progress of women in surgery is undeniable. Previous female surgeons achieved this, in part, by mentoring the next generation of hopeful students and ensuring their space in surgical settings. Despite these advancements, there remains an enduring stereotype of surgeons present to this day. Arnold-Forster argues in her novel these stereotypes remain because they serve to elevate and uphold the exclusivity of the surgical profession. She writes, “Paternalism and heroism place the surgeon in an elevated position compared not only to his patients but also to society more broadly”. 51
Besides persistent ideologies, active structural discrimination of women pursuing medicine is not a barrier of the past. In 1969-1970, only 15.7% of enrolled medical students in Canada were women. 52 In 1961, only 4.3% of Canadian physicians were women. Of those, 2% were obstetricians, 1.9% were plastic surgeons, and .6% were in general surgeons. There were no female neurosurgeons, orthopedic surgeons, or urologists. 53 In addition in the 1960s, the Collège des Médecins du Québec, the professional order overseeing practicing physicians in Quebec prohibited women from leading a surgical team.44,45 In the 1970s, it was discovered during a United States Congressional hearing that medical school were systemically denying the admission of female students into their programs. 54 Since 2019, female medical students comprise most of newly admitted medical students. 1 In 2023, 50.6% of American medical school graduates were women. 55 Despite active discrimination since the 19th century, women now total 30% of all practicing surgeons in the United States. 55 In 2022, 36% of all Canadian surgeons were women. 56 Though this is an observable advancement, a minority presence suggests that some obstacles remain.
A qualitative study by Incorvaia and colleagues found that women surgeons cited successful mentors as one of the reasons why they pursued their careers. 57 Mentorship throughout one’s career is critical to professional development due to the nature of the evolving role of surgical trainees into professionals. 41 This process is facilitated by the establishment of organizations providing mentorship to the next generation of women wishing to pursue surgical careers. The Association of Women Surgeons, founded in 1981, is one of the largest organizations of its kind with a mission to “inspire, encourage and enable women surgeons to realize their professional and personal goals.” 58 These organizations, paired with the growth of female representation in the field of surgery, foster an environment of advocacy to uplift and support women as they develop professionally.
A once male-exclusive profession is now slowly, but surely, forced to see women as equal and qualified. Historical figures, such as Scharlieb, displayed exceptional technical skills that “She helped the women’s movement in what is perhaps the really best way, by the excellence of her work.” 32 In recent studies, female surgeons were associated with equal 59 or fewer 60 postsurgical complications compared to their male counterparts. In addition, popular media is actively playing a role in the representation of women in surgery. Although early television shows often depicted heroic male surgeons such as Casey, current shows like Grey’s Anatomy highlight the trials and tribulations of main female characters such as Dr Meredith Grey and Dr Cristina Yang as surgical residents.
One day, we hope to disseminate the gendered idea of what a surgeon is “supposed” to resemble, to the point a different riddle will need to be used to explain heuristic bias.
Footnotes
Acknowledgments
I would like to thank both Dr Thomas Schlich and Dr Annmarie Adams for their continuous feedback as I undertook this project. I’d also like to thank Dr Justin Barr for his guidance, particularly in the early stages of this essay. Lastly, I’d like to thank the History and Archived Committee of the American College of Surgeons for awarding me with special commendation as part of the 2024 Clinical Congress.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Appendix
This article was selected for commendation by the History and Archives Committee of the American College of Surgeons, as part of the history of surgery paper competition at the 2024 Clinical Congress.