
Abstract
Background
Enhanced Recovery After Surgery (ERAS) pathways improve healthcare quality, safety, and cost-effectiveness. We hypothesized that the RAND Method (a hybrid Delphi approach), involving anonymous sequential surveys and face-to-face meetings, would allow for more rapid agreement and initiation of new ERAS pathways.
Methods
Using the ERAS Society guidelines for cesarean section as a baseline, our institution’s ERAS Leadership Team (ELT) compiled published literature and institutional practices to design a 32-component survey that was sent to obstetricians, nurse midwives, anesthesiologists, pharmacists, and nurses. Components that did not reach 90% consensus were included in a second survey the following week, and meetings were held to review results.
Results
ERAS pathway components were compiled and reviewed by 121 stakeholders at 7 hospitals using iterative surveys with review meetings over a 13-week period. Survey response rates were 61% and 50% in the initial and follow-up surveys, respectively. There was agreement on 28/32 and 32/32 items on the initial and follow-up surveys. Using the RAND Method, time to agreement decreased by 54.1% (24 vs 13 weeks) compared to prior system-wide efforts to standardize the colorectal surgery ERAS pathway.
Discussion
With rapidly expanding healthcare systems, effective methods to gain consensus and adopt ERAS pathways are critical to implementation of ERAS guidelines. We demonstrate that the RAND Method allows for a transparent and efficient means of agreement across a diverse group of clinicians practicing in several settings.
Key Takeaways
System-wide education and consensus are necessary for adoption of Enhanced Recovery After Surgery (ERAS) pathways. We found that by combining sequential surveys with in-person meetings to discuss survey, we decreased implementation time across a larger number of hospitals within our health system. This technique, known as the RAND Method, is an excellent template for more rapid adoption of best clinical practice by all members of the healthcare team and will be used in future implementations across our system.
Introduction
Years pass between translational research discoveries and the implementation of those findings into clinical practice. 1 Although it is well established that patient outcomes improve with adherence to evidence-based guidelines, there is limited data on methods to expedite adoption of new practices. 2
A four-step model was proposed by Pathman et al to improve the utilization of clinical guidelines: awareness, agreement, adoption, and adherence. 3 The initial steps of awareness and agreement require reconciliation of clinical practice with published guidelines across institutions with variable personnel, medication formularies, and workflows. Several methods have been described to gain consensus among groups, including informal consensus meetings (ICM), the Delphi method, and the RAND Method (a Delphi method hybrid). 4
The Delphi method is a commonly used consensus method that consists of six steps: (1) identifying a research question; (2) summarizing the literature; (3) designing a survey; (4) conducting anonymous iterative survey rounds; (5) providing individual or group feedback between rounds; and (6) summarizing the findings.
4
The RAND Method is a hybrid approach
An Enhanced Recovery After Surgery (ERAS) pathway is a multi-disciplinary approach to standardization of the preoperative, intraoperative, and postoperative phases of care for specific surgical procedures. 5 Models for implementing and disseminating these pathways within large healthcare systems are currently under examination. 6 Our health care system is in the process of standardizing ERAS pathways across institutions, which requires input from up to 12 member hospitals, each with unique geography, patient demographics, and hospital settings. Recent implementation of a healthcare system ERAS pathway for colorectal surgery required 24 weeks for a multi-disciplinary content review group to reach agreement on the details of the pathway components.
We hypothesized that the RAND Method would allow more rapid evaluation and agreement on pertinent elements of complex ERAS pathways across a health care system. This study compares the development of two, separate health care system-level ERAS pathways with and without utilization of the RAND Method to reach consensus.
Materials and Methods
This study was exempted from the University of North Carolina IRB review as surveys were issued and completed for the purpose of improving services and programs. Privacy of participants was protected, confidentiality of individual responses was maintained, and survey participation was voluntary.
Our health care system currently is composed of 12 hospitals across the 9th most populous state in the US. To decrease care variation and improve clinical outcomes, we developed a system-level ERAS program. The first system-level ERAS pathway was created using ICM between two hospitals that had existing colorectal ERAS programs.
RAND Method
Using the recently published ERAS Society guidelines for the care of patients undergoing cesarean section,7–9 we used the RAND Method to reach health care system-level consensus on this novel system-level ERAS pathway.10,11
The health system uses a three-tiered approach to pathway implementation, consisting of: the ERAS Leadership Team (ELT), the Pathway Core Teams (PCT), and Subject Matter Experts (SME) made up of pathway end-users (Figure 1). Leadership structure for system-level Enhanced Recovery After Surgery (ERAS) pathway development.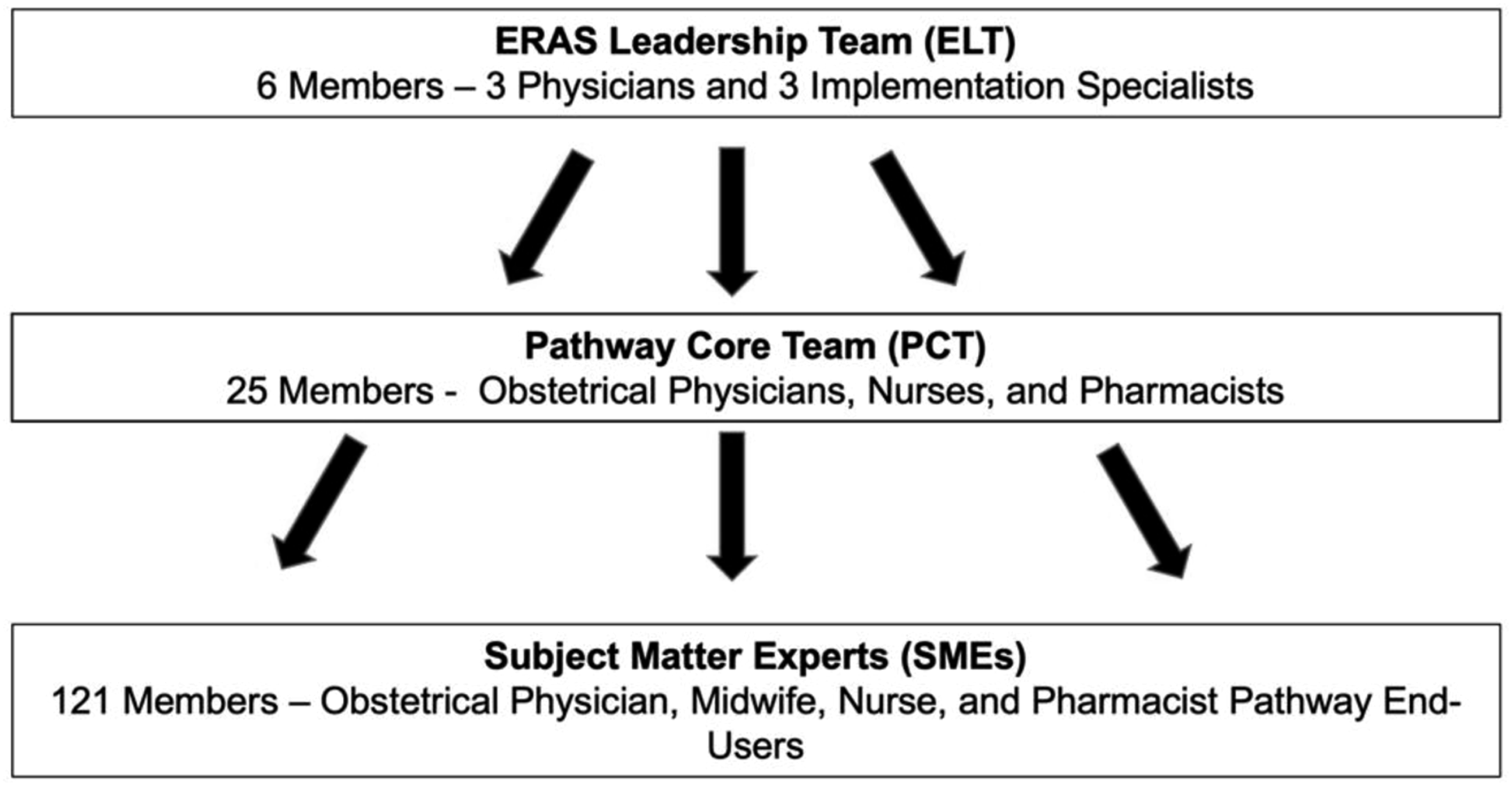
The survey was sent to a team of 121 SMEs with members from each system hospital that performs cesarean deliveries, including obstetricians, family medicine physicians, anesthesiologists, nurse midwives, pharmacists, and nurses who planned to be involved in the Enhanced Recovery Programs across the hospital system. Participants were required only to complete the sections for which they routinely provide care. The survey allowed votes to include, exclude, or revise each component. If a clinician voted to exclude or revise a component, the clinician was asked to provide rationale. The two open-ended questions “What did we forget?” and “What questions do you have for the ERAS team?” were included at the end of the survey to promote communication.
Prior to survey distribution, a threshold of 75% agreement was created by the ELT, and the decision was made to include each item below that threshold in subsequent surveys until consensus could be achieved. After the first survey distribution, greater than 75% consensus was reached on all items. To ensure agreement across the system, the ELT, in discussion with the PCT, increased the threshold to 90% for consensus.
Informal Consensus Meetings
The health care system-wide adult colorectal ERAS pathway was developed by the same ELT, and a PCT composed of colorectal surgeons, anesthesiologists, nurses, pharmacists, and ERAS program managers at the two hospitals with existing colorectal ERAS programs. These pathway development meetings took place in person when possible.
Analysis
Following completion of the health care system-level cesarean pathway for ERAS, the timeline was compared to health care system-level development of our adult colorectal ERAS pathway. The primary endpoint was time to gain clinician consensus.
Results
RAND Method
Subject Matter Expert survey responses, by health care job-type.
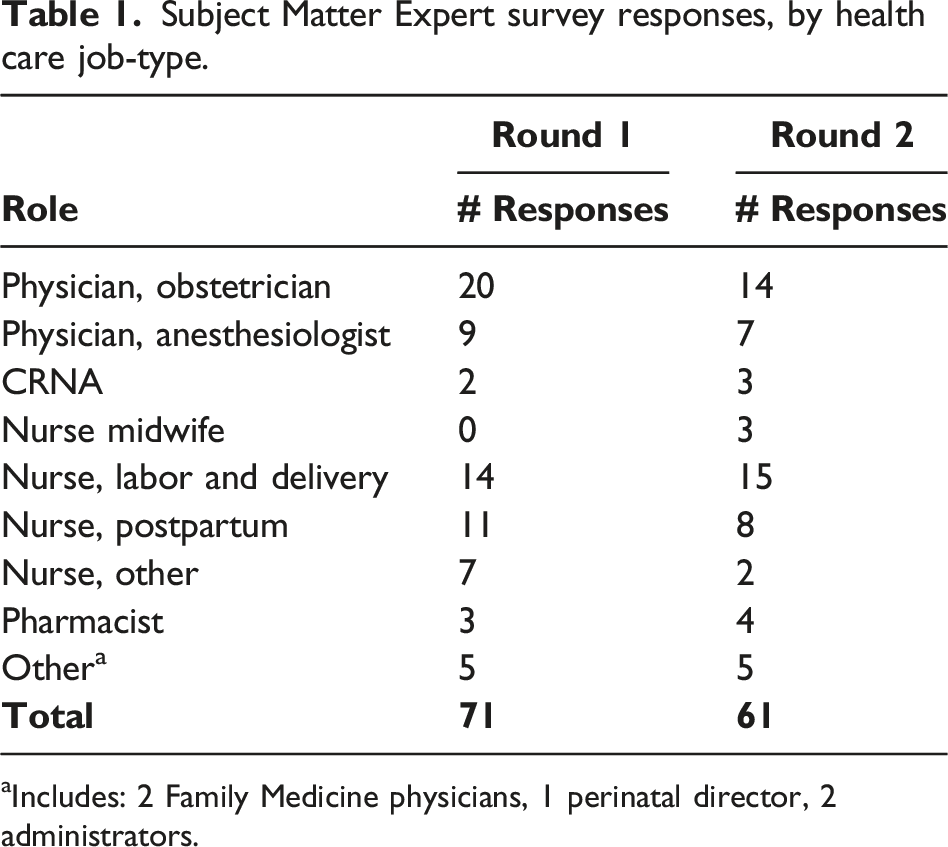
aIncludes: 2 Family Medicine physicians, 1 perinatal director, 2 administrators.
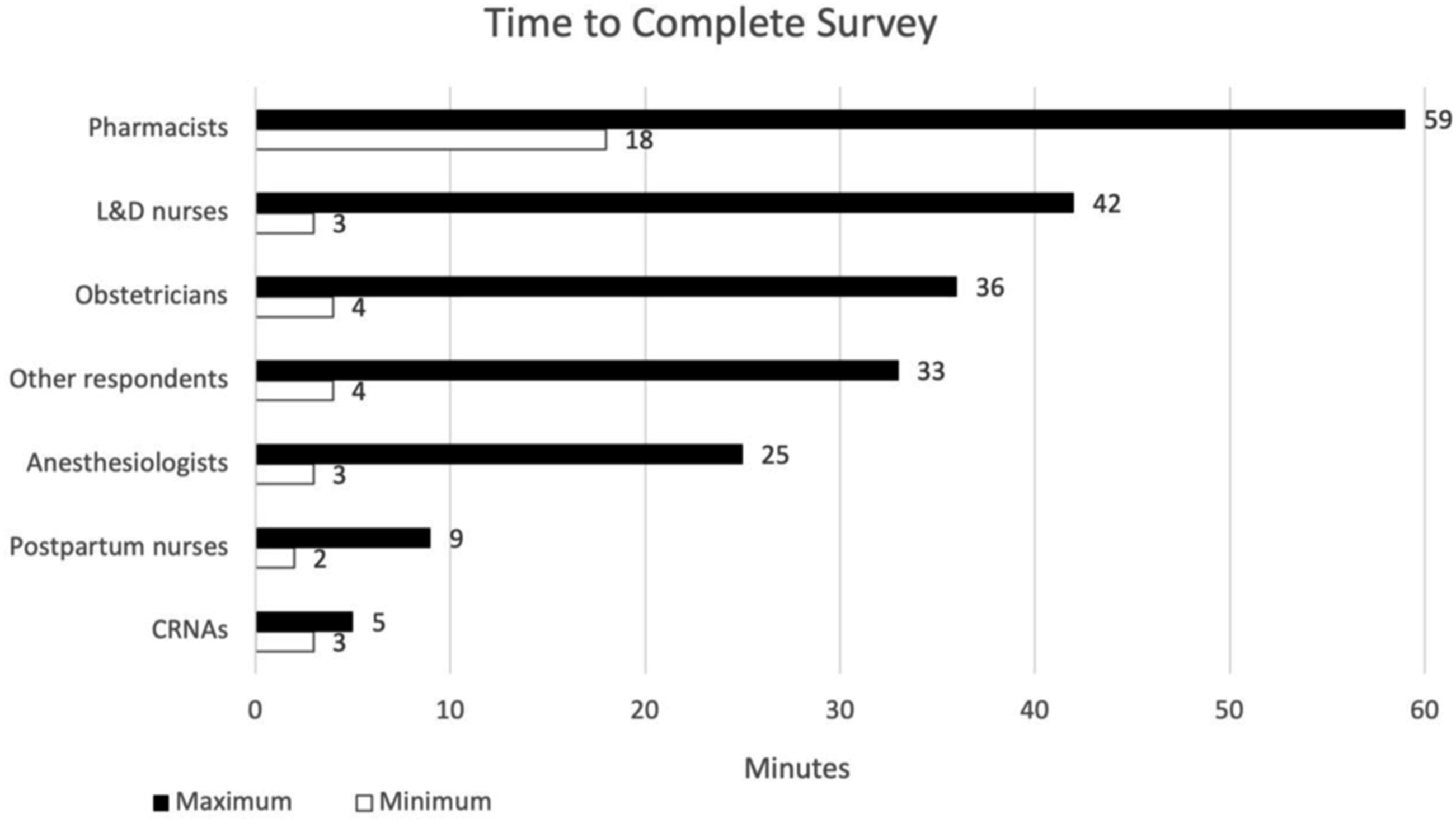
Range of time spent in survey completion by job-type.
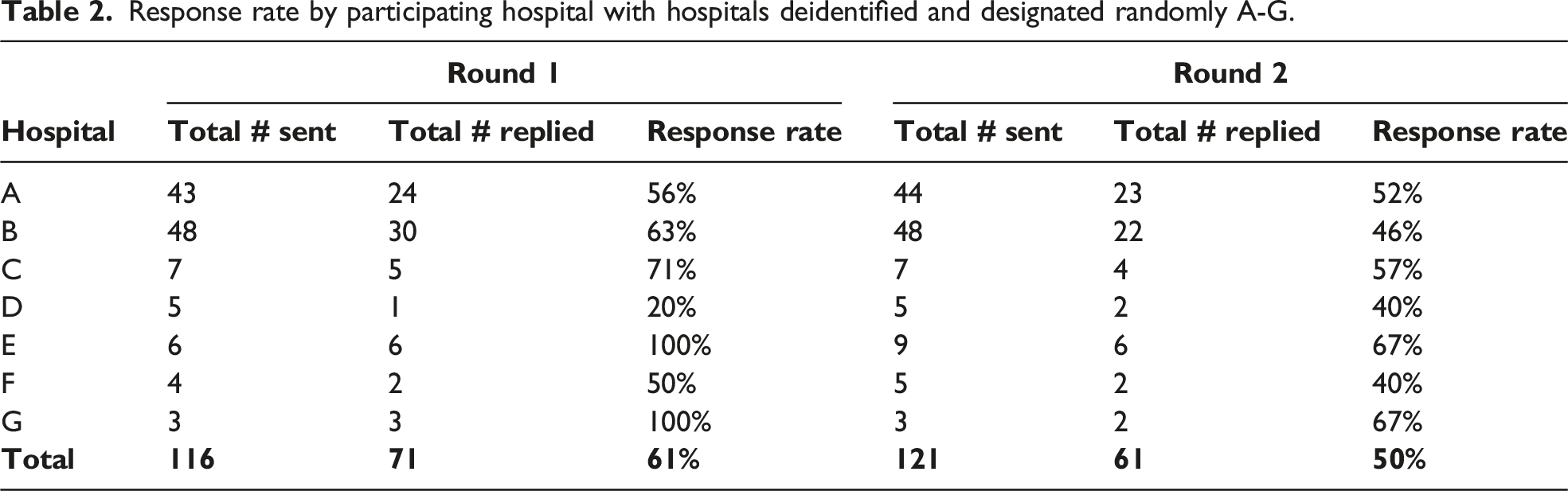
Response rate by participating hospital with hospitals deidentified and designated randomly A-G.
Survey response rates by pathway component.
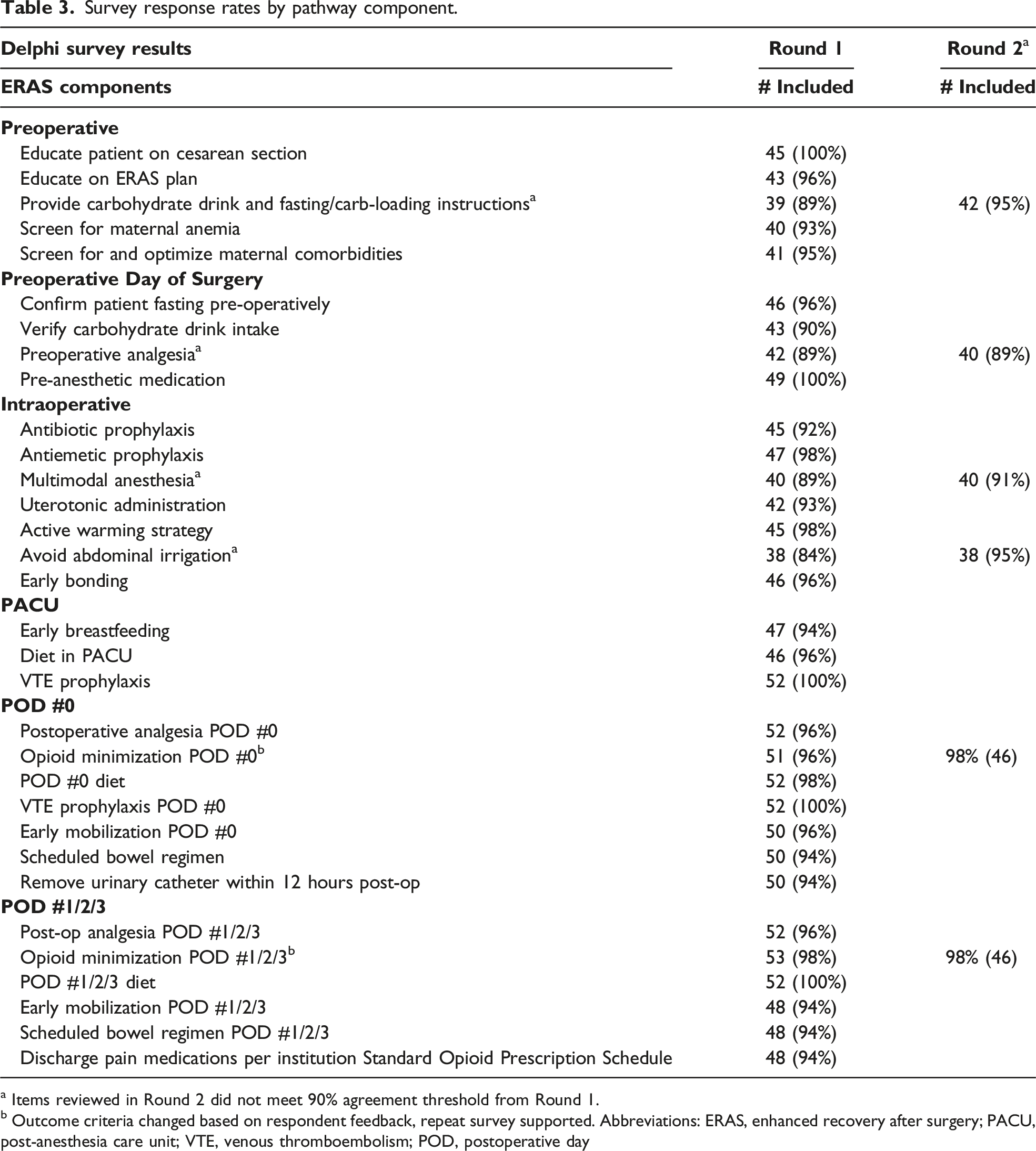
a Items reviewed in Round 2 did not meet 90% agreement threshold from Round 1.
b Outcome criteria changed based on respondent feedback, repeat survey supported. Abbreviations: ERAS, enhanced recovery after surgery; PACU, post-anesthesia care unit; VTE, venous thromboembolism; POD, postoperative day
After the second survey, one remaining item did not meet the 90% threshold. Following review, a group decision was made to retain this item (pre-operative analgesia) within the pathway. This decision was based on standardizing the cesarean section pathway with the existing metrics in the adult colorectal surgery pathway and to decrease care variation between ERAS pathways. Following this final meeting, a final system-level ERAS pathway for cesarean sections was agreed upon with nearly unanimous consensus. This occurred over the course of 13 weeks. (Figure 3) Timeline to reach consensus on system-level Enhanced Recovery After Surgery (ERAS) pathway for cesarean section surgery.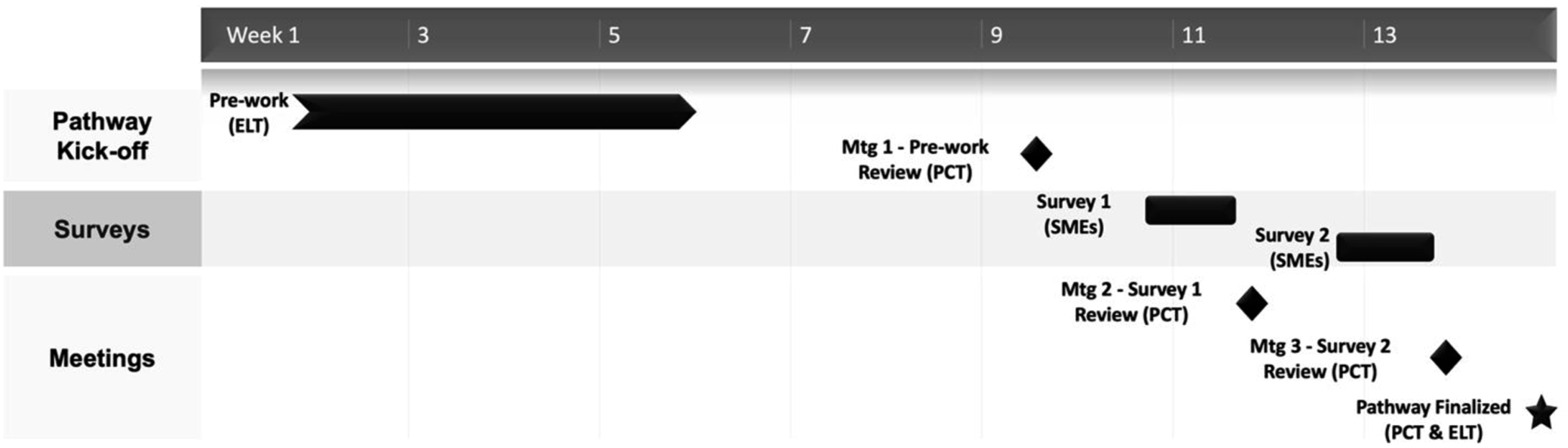
Informal Consensus Meetings
Despite
Discussion
We found that using the RAND Method to gain system-level consensus was more efficient and reached a larger audience than the use of ICM. The RAND Method shortened the time to consensus on pathway components by 11 weeks in a pathway with a similar number of components but involving far more hospitals within the health care system (7 vs 2 hospitals).
The awareness-to-adherence model described by Pathman includes increasing awareness and reaching consensus among stakeholders as its first two steps.
3
Our formalized use of these steps allow for inclusion of a wide range of knowledge and experience, interaction between members, and stimulation of debate. Additionally, they can prevent vocal and more senior members from overly influencing group decisions when the evidence is insufficient.
13
The RAND Method allows a large number of heterogeneous participants, limits dominance of highly opinionated individuals, and allows substantial time to express ideas and reflect upon answers. Additionally, it is inexpensive, convenient, and there are no geographic constraints.4,13 Unlike the Delphi technique alone, the RAND Method creates an opportunity for personal contact between experts with face-to-face meetings
While the Delphi method has been used to create an international consensus on an ERAS training curriculum and to reach consensus on topics related to perioperative fluid management, no other study describes the use of the Delphi method for initial pathway alignment across multiple hospitals.14,15 While the Delphi method allowed for asynchronous review of guidelines and multiple iterations, it did not afford a transparent review of the disagreements between stakeholders provided by the RAND Method. A recent study described the design, development, and implementation of ERAS pathways at Kaiser Permanente in Northern California. To create and align pathways, a multi-disciplinary workgroup compiled guidelines and held an in-person panel-based summit attended by 400 stakeholders, using ICM methods for their health care system (19). Additional large health systems have described their experience using large ICM with commercially available programs. 6 While those studies provide a difficult comparator because they include analysis of the entire implementation, our process of education and consensus utilized similar ICM methods of all involved stakeholders, but without extremely high resource requirements.
Because of its retrospective nature, one limitation of our study is a precise measurement of time to consensus on an individual and group level. Additionally, the pathways implemented were examined within different groups of clinicians and no baseline examination of pre-ERAS practice variation was performed to compare how disparate the clinical practice was before and after ERAS implementation. Specifically, it is unclear how clinical practice differed from ERAS principles in adult colorectal and scheduled cesarean sections prior to implementation. This could be responsible for differences in the time taken to gain pathway consensus. Additionally, while the survey participation was voluntary, and response rates were 61% and 50% for each round of surveys, it is unknown if non-respondents agree and whether potential disagreements would lead to variations in clinical care after pathway implementation. Thus, it remains to be determined what impact these developed pathways will have on clinician pathway compliance and patient outcomes. Lastly, it is difficult to estimate the degree to which ELT experience in pathway implementation vs consensus methodology had on the time to consensus.
One of the benefits of the RAND approach is that education occurs during pathway development and consensus building. More than half of stakeholders provided specific feedback on the pathway components, so less education was needed after implementation. The increased participation in pathway development enabled by the RAND Method has improved clinician enthusiasm and willingness to adopt new protocols at each site. We hypothesize that this will beget wider adoption, stronger adherence, and improved outcomes data.
Strengths of this study include engagement of diverse stakeholders from geographically disparate hospitals, with survey participation at all seven hospitals. An additional benefit to utilization of the RAND Method is that rapid consensus among variable institutions was obtained using a 6-member central ELT. The ELT was able to obtain input from the existing obstetrics staff without putting undue demands on busy clinicians.
Overall, based on the parameters of consensus opinion agreed upon by our ERAS leadership, the utilization of the RAND Method greatly expedited pathway development and will be used in implementation of additional pathways in the future. The use of sequential surveys and the RAND Method was time-efficient, effective at capturing input and areas of disagreement, easy to administer, while generating concrete action areas for discussion at more focused meetings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.