
Abstract
Background
Readmission at a non-index hospital, or care fragmentation (CF), has been previously linked to greater morbidity and resource utilization. However, a contemporary evaluation of the impact of CF on readmission outcomes following elective colectomy is lacking. We additionally sought to evaluate the role of hospital quality in mediating the effect of CF.
Methods
All records for adults undergoing elective colectomy were tabulated from the 2016 to 2020 Nationwide Readmissions Database. Patients readmitted non-electively within 30 days to a non-index center comprised the CF cohort (others: Non-CF). Hierarchical mixed-effects models were constructed to ascertain risk-adjusted rates of major adverse events (MAEs, a composite of in-hospital mortality and any complication) attributable to center-level effects. Hospitals with risk-adjusted MAE rates ≥50th percentile were considered Low-Quality Hospitals (LQHs) (others: High-Quality Hospitals [HQHs]).
Results
Of 68,185 patients readmitted non-electively within 30 days, 8968 (13.2%) were categorized as CF. On average, CF was older, of greater comorbidity burden, and more often underwent colectomy for cancer, relative to Non-CF. Following risk adjustment, CF remained independently associated with greater likelihood of MAE (adjusted odds ratio [AOR] 1.16, 95% Confidence Interval [CI] 1.05-1.27) and per-patient expenditures (β+$2,280, CI +$1080-3490). Further, readmission to non-index LQH was linked with significantly increased odds of MAE, following initial care at HQH (AOR 1.43, CI 1.03-1.99) and LQH (AOR 1.72, CI 1.30-2.28; Reference: Non-CF).
Conclusions
Care fragmentation was associated with greater morbidity and resource utilization at readmission following elective colectomy. Further, rehospitalization at non-index LQH conferred significantly inferior outcomes. Novel efforts are needed to improve continuity of care.
Key Takeaways
• Care fragmentation following elective colectomy is associated with greater morbidity and resource utilization. • Patients experiencing care fragmentation were more commonly older, insured by Medicare, and treated for colon cancer. • Readmitting hospital quality mediated the effect of care fragmentation, such that rehospitalization at low-quality institutions was linked with inferior outcomes, relative to others.
Introduction
Over the past two decades, a growing body of work has supported the centralization of specialized surgical care. Higher operative volumes have been linked with lower mortality and complication rates for a myriad of procedures, including coronary artery bypass grafting, pulmonary lobectomy, and esophagectomy. 1 In addition to improved outcomes, centralization of complex operations in the current era of value-based care has been touted as an important cost-containment strategy. However, regionalization has also been recognized to negatively affect continuity of postsurgical treatment, particularly upon rehospitalization. 2
The impact of care discontinuity is thought to be particularly relevant for complex elective operations, such as colectomy. Colorectal resections are linked with high readmission rates, with ∼15%–25% of patients requiring rehospitalization with 30 days of discharge. 3 Return to non-index centers, or care fragmentation, has been associated with significantly greater mortality and complications, relative to the original operating facility.4-7 Yet, while much is known about care fragmentation, the relationship between the quality of readmission hospital and associated outcomes remains unknown. A more nuanced understanding could guide patient counseling, quality improvement efforts, and broader policies around regionalization of care.
In the present work, we sought to examine whether the quality of readmission hospital mediated the impact of care discontinuity on rehospitalization outcomes following elective colectomy. We hypothesized that readmission to non-index, low-quality hospitals would confer significantly inferior outcomes.
Methods
Data Source and Study Cohort
All adult (≥18 years) hospitalizations entailing elective colectomy were tabulated from the 2016 to 2020 Nationwide Readmissions Database (NRD) using previously validated International Classification of Diseases, Tenth Revision procedure codes. 8 As the largest all-payer database reporting readmissions, the NRD accounts for >60% of all hospitalizations in the U.S., each year. Unique patient linkage numbers are utilized to track readmissions within each calendar year. 9
Only records involving non-elective readmission within 30 days of index hospitalization were considered for analysis. Those missing key data were excluded (<1%). Patients undergoing colectomy >5 days following hospital admission were not considered to ensure sample homogeneity. Patients receiving an operation in December of each year were similarly excluded, due to lack of complete 30-day readmission data (Figure 1). Study CONSORT diagram of survey-weighted estimates of 68185 patients meeting study inclusion criteria and 8968 (13.2%) experienced non-elective readmission to a non-index hospital and comprised the CF cohort. Of these, 4866 (54.3%) originally underwent a colectomy at LQH and 4102 (45.7%) at HQH. Considering patients initially treated at LQH, 1092 (22.5%) were readmitted to non-index LQH (Low-Low) and 717 (14.7%) to non-index HQH (Low-High). Meanwhile, of individuals who originally sought care at HQH, 884 (21.6%) were readmitted to non-index HQH (High-High), while 742 (18.1%) were rehospitalized at LQH (High-Low).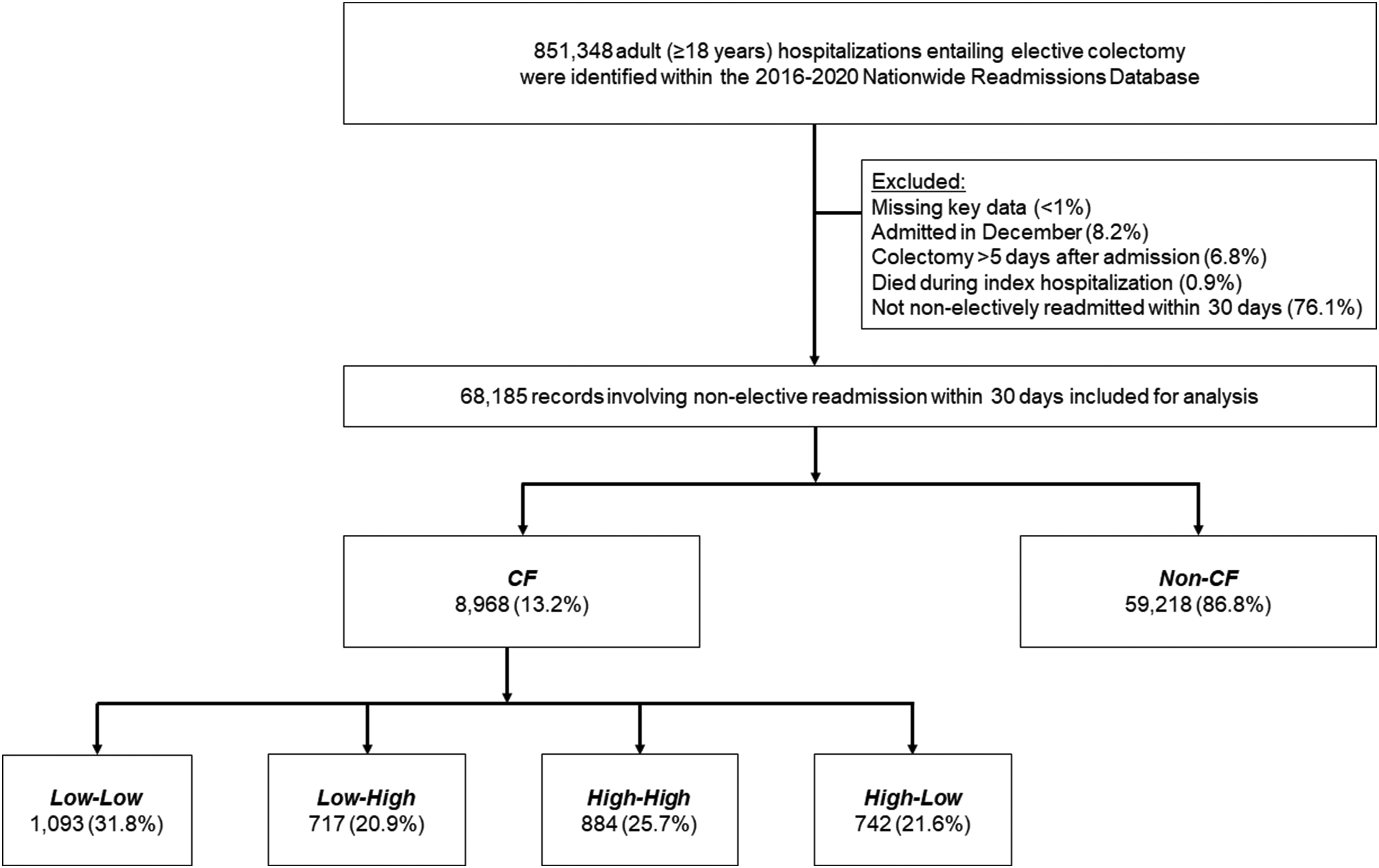
Variable Definitions
The Healthcare Cost and Utilization Project Data Dictionary was utilized to define relevant patient, disease, and hospital variables, including age, sex, income quartile, insurance coverage, and hospital teaching status. 9 The burden of comorbidities was quantified using the van Walraven modification of the Elixhauser Comorbidity Index. 10 Indication for colectomy was categorized as colon cancer, benign colonic neoplasms, diverticular disease, inflammatory bowel disease, or other. 8 Surgical approach was stratified as open or minimally invasive (MIS), including both laparoscopic and robotic techniques. Extent of resection was stratified as right/left hemicolectomy, transverse colectomy, sigmoidectomy, or total colectomy. The presence of patient comorbidities and perioperative complications was captured using previously reported ICD-10 diagnosis and procedure codes. 8 Complications were subsequently classified as cardiac, gastrointestinal, infectious, renal, respiratory, or thrombotic. Major adverse events (MAEs) were considered to be a composite of in-hospital mortality or the incidence of any major perioperative complication. Institutional volume was computed as the annual, hospital colectomy caseload. Hospitalization expenditures were calculated using hospital-specific, cost-to-charge ratios detailed in the NRD and then inflation-adjusted using the 2020 Personal Healthcare Price Index. Primary readmission diagnoses were identified using Diagnosis Related Group Codes, as previously detailed. 11
Hierarchical Modeling of Hospital Quality
We fit a two-level, mixed-effects logistic regression to consider factors linked with incidence of MAE. Patient characteristics including age, sex, insurance coverage, income quartile, and relevant comorbidities comprised the first level. The second level was the unique hospital identifier. The intraclass correlation coefficient (ICC) was calculated to represent the degree of observed variation in MAE attributable to interhospital differences. Using previously reported Bayesian methods, 12 we estimated random intercepts to generate the center-specific, absolute risk of MAE. Centers with MAE rates in the ≥50th percentile were designated Low-Quality Hospitals (LQHs), while those with rates <50th percentile were considered High-Quality Hospitals (HQHs).
Cohort Stratification
Patients readmitted to a non-index hospital were considered CF (others: Non-CF). Within this group, we stratified patients based on quality of the index and readmission facilities. Patients initially treated at LQH who were readmitted to non-index LQH comprised the Low-Low cohort, while those readmitted to HQH were classified as Low-High. Similarly, among patients initially treated at HQH, individuals originally admitted to HQH who were subsequently treated at LQH were defined as the High-Low cohort, while those readmitted to non-index HQH were considered the High-High cohort (Figure 1).
Study Outcomes
The primary endpoint of this study was the incidence of MAE upon readmission. We additionally considered duration of hospitalization (LOS), expenditures, and non-home discharge.
Statistical Analysis
Data are reported as medians with interquartile range (IQR) if continuous or as proportions (%) if categorical. The significance of intergroup differences was assessed using the Mann-Whitney U, Kruskal-Wallis, or Pearson’s Chi-squared test, as appropriate. Multivariable models were developed to assess the independent association of care fragmentation with outcomes of interest. All covariates were selected for inclusion using elastic net regularization. Briefly, this method applies a penalized least-squares approach to minimize factor collinearity and enhance out-of-sample generalizability. 13 Ultimately, regression models for readmission outcomes adjusted for patient age, sex, relevant comorbidities, income, insurance coverage, extent of colectomy, operative approach, surgical indication, incidence of any major complication during index hospitalization, reason for readmission, and readmitting center teaching status. Model discrimination was evaluated using receiver operating characteristics or the coefficient of determination. Logistic and linear model outputs are detailed as adjusted odds ratios (AORs) or as beta-coefficients (β), respectively, both with 95% confidence intervals (CIs).
All statistical analyses were performed using Stata 16.1 (StataCorp, LLC, College Station, TX). Statistical significance was set at α = .05. This study was exempted from full review by the Institutional Review Board at the University of California, Los Angeles, due to the deidentified nature of the NRD.
Results
Care Fragmentation
Demographic, Clinical, and Hospital Characteristics.
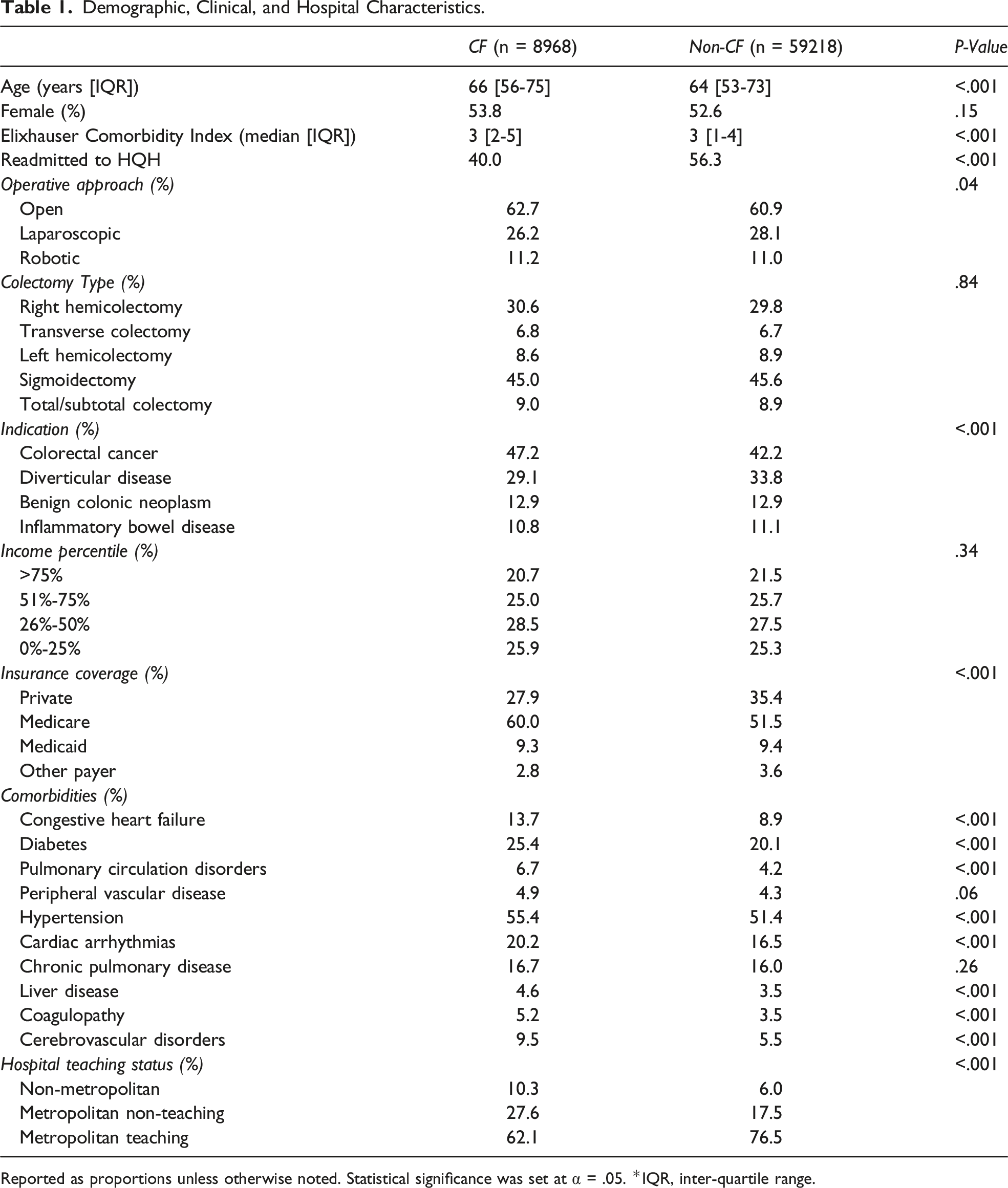
Reported as proportions unless otherwise noted. Statistical significance was set at α = .05. *IQR, inter-quartile range.
Outcomes Following Care Fragmentation
Unadjusted and Adjusted Outcomes.
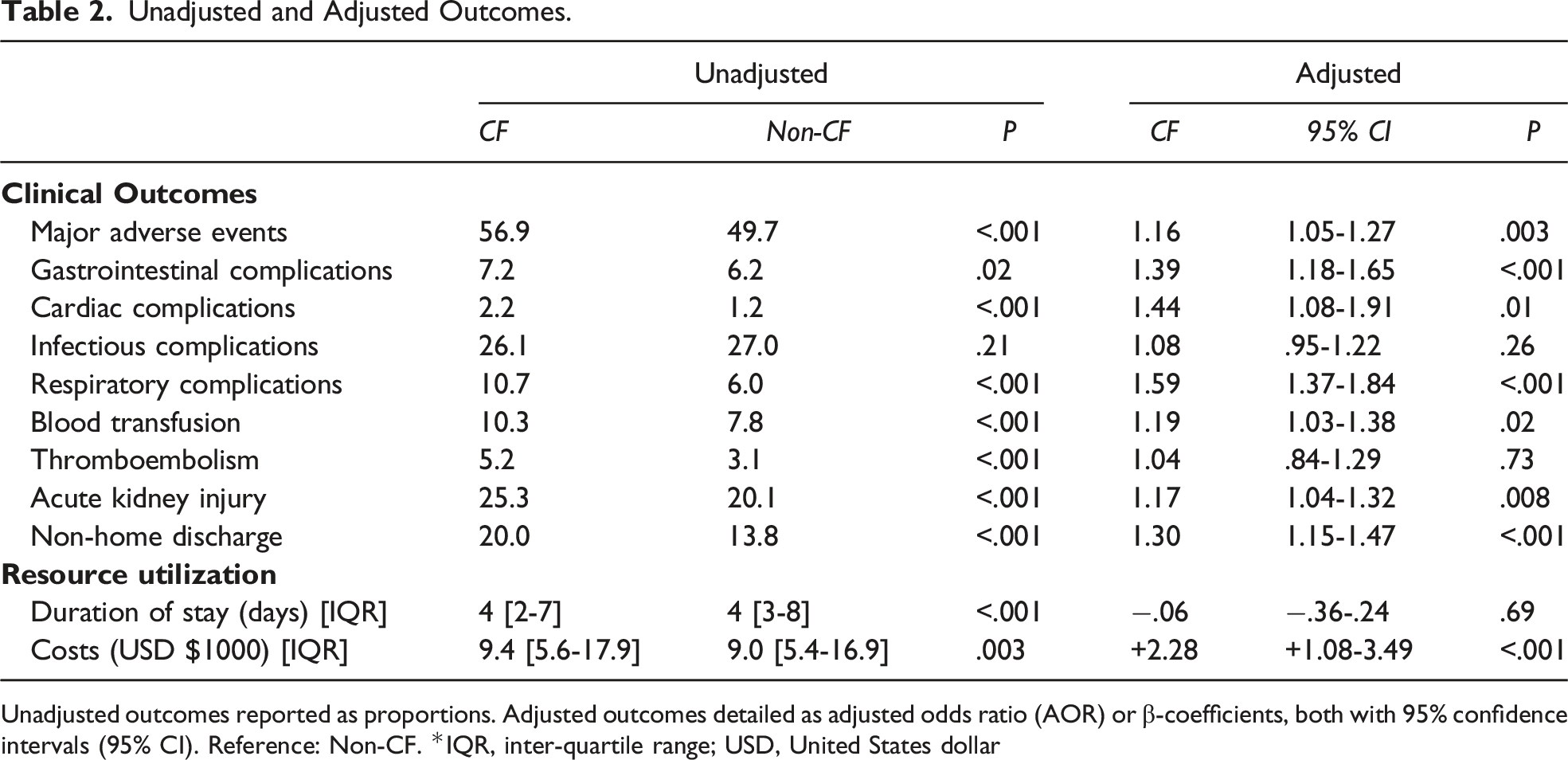
Unadjusted outcomes reported as proportions. Adjusted outcomes detailed as adjusted odds ratio (AOR) or β-coefficients, both with 95% confidence intervals (95% CI). Reference: Non-CF. *IQR, inter-quartile range; USD, United States dollar
Hierarchical Modeling and Hospital Quality
After applying a hierarchical multivariable model, 9.4% of variation in MAE rates was found to be attributable to hospital-level factors (intraclass correlation coefficient = .094; receiver operating characteristic: .74) (Figure 2). Interhospital variations in rates of MAE centers were ranked by the hospital-attributable, risk-adjusted rates of major adverse events (MAEs), comprising in-hospital mortality or any major complication following elective colectomy. Institutions with MAE rates in the ≥50th percentile were designated Low-Quality Hospitals (LQHs), while those with rates <50th percentile were considered High-Quality Hospitals (HQHs). Error bars represent 95% confidence intervals. For ease of visualization, only hospitals recorded in the 2019 Nationwide Readmissions Database are displayed.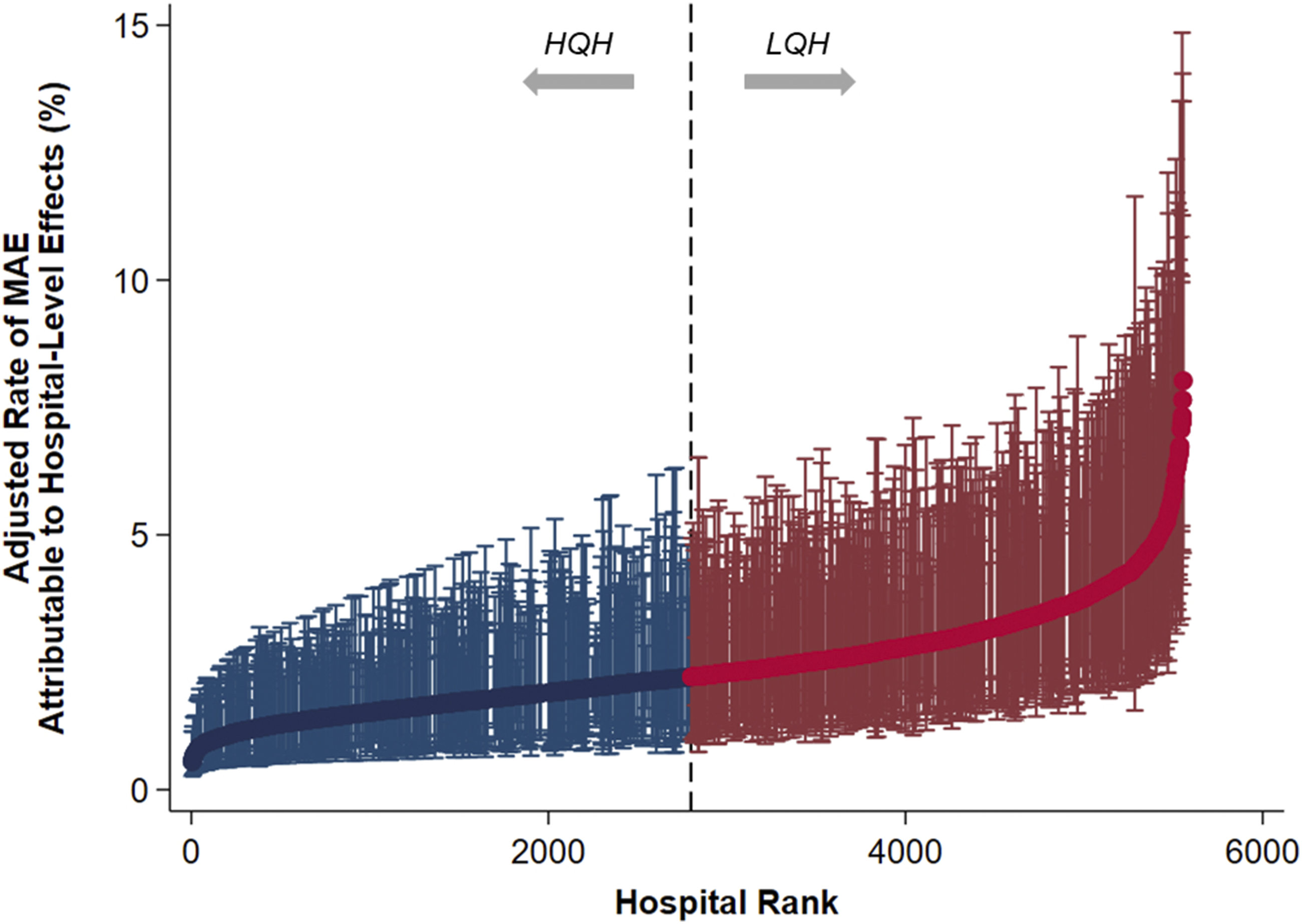
On average, LQH and HQH demonstrated similar annual elective colectomy caseloads (142 [71-258] vs 145 cases per year [68-264], P = .94).
Readmission Stratification
Of the 8968 patients who experienced care fragmentation, 4866 (54.3%) were initially treated at LQH and 4102 (45.7%) at HQH. Considering patients originally treated at LQH, 1092 (22.5%) were readmitted to non-index LQH (Low-Low) and 717 (14.7%) to non-index HQH (Low-High). Of those initially treated at HQH, 884 (21.6%) were readmitted to non-index HQH (High-High), while 742 (18.1%) were rehospitalized at LQH (High-Low).
On average, and relative to Non-CF, patients in the CF groups were older (Low-Low 65 [56-74] vs Low-High 66 [54-74] vs High-High 67 [55-76] vs High-Low 67 [57-76] vs Non-CF 64 years [53-73], P < .001) but of similar sex and income. The groups similarly often underwent minimally invasive resection. However, all CF subgroups more often underwent colectomy for malignancy, than Non-CF (Low-Low 48.3 vs Low-High 50.3 vs High-High 48.4 vs High-Low 44.9 vs Non-CF 42.2%, P = .01) (Supplemental Table S1). In addition, the CF cohorts were more often readmitted for cardiovascular issues (11.9 vs 10.2 vs 12.1 vs 12.0 vs 5.1%), while Non-CF was more frequently rehospitalized for gastrointestinal reasons (42.2 vs 24.1 vs 30.3 vs 30.9 vs 29.5%, P < .001).
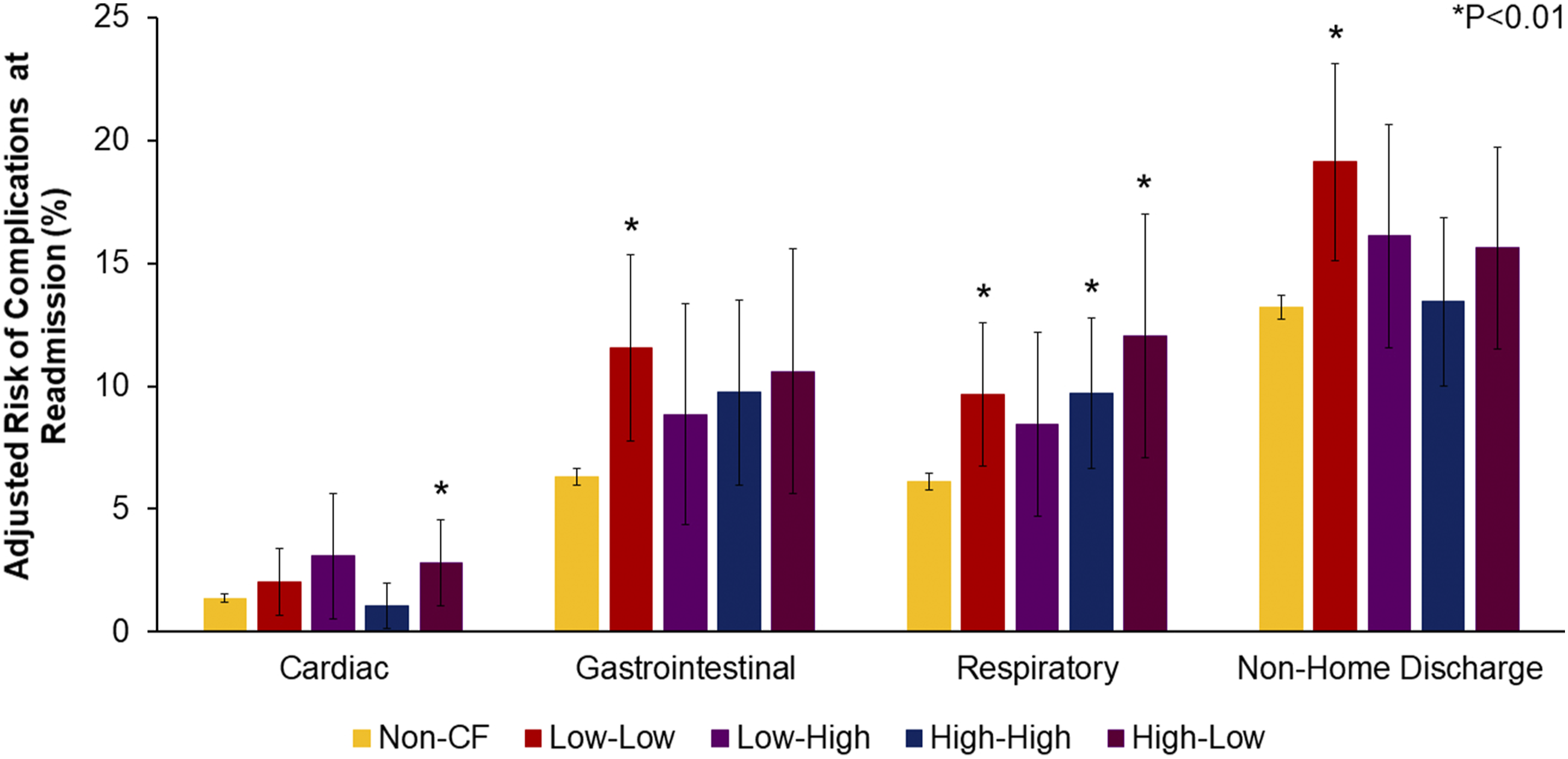
Unadjusted outcomes are detailed in Supplemental Table S2. After risk adjustment, Low-Low (AOR 1.72, CI 1.30-2.28) and High-Low (AOR 1.43, CI 1.03-1.99) demonstrated greater likelihood of MAE, with Non-CF as the reference (Figure 3). Further, Low-Low had greater odds of thromboembolism (AOR 1.83, CI 1.06-3.17) and acute kidney injury (AOR 1.35, CI .98-1.86) (Figure 4). The cohorts were similar in LOS. However, Low-High (β+$3,290, CI + 380-6200) and High-Low (β+$3,920, CI + 330-7510) faced increased expenditures, relative to Non-CF (Supplemental Table S3). Adjusted likelihood of MAE, stratified by care fragmentation subgroup following risk adjustment, Low-Low (59.3%, CI 54.2%-64.4%) and High-Low (56.0%, CI 49.9%-62.0%) remained associated with increased likelihood of MAE, with Non-CF (49.3%, CI 48.7%-49.9%) as the reference. Low-High (52.2%, CI 46.2%-58.2%) and High-High (52.4%, CI 46.8%-57.9%) were linked with similar odds of MAE. Risk-adjusted complication rates at readmission, stratified by care fragmentation subgroup risk-adjusted rates of cardiac, respiratory, and gastrointestinal complications, and non-home discharge, displayed for all CF subgroups. Reference: Non-CF. * indicates statistical significance.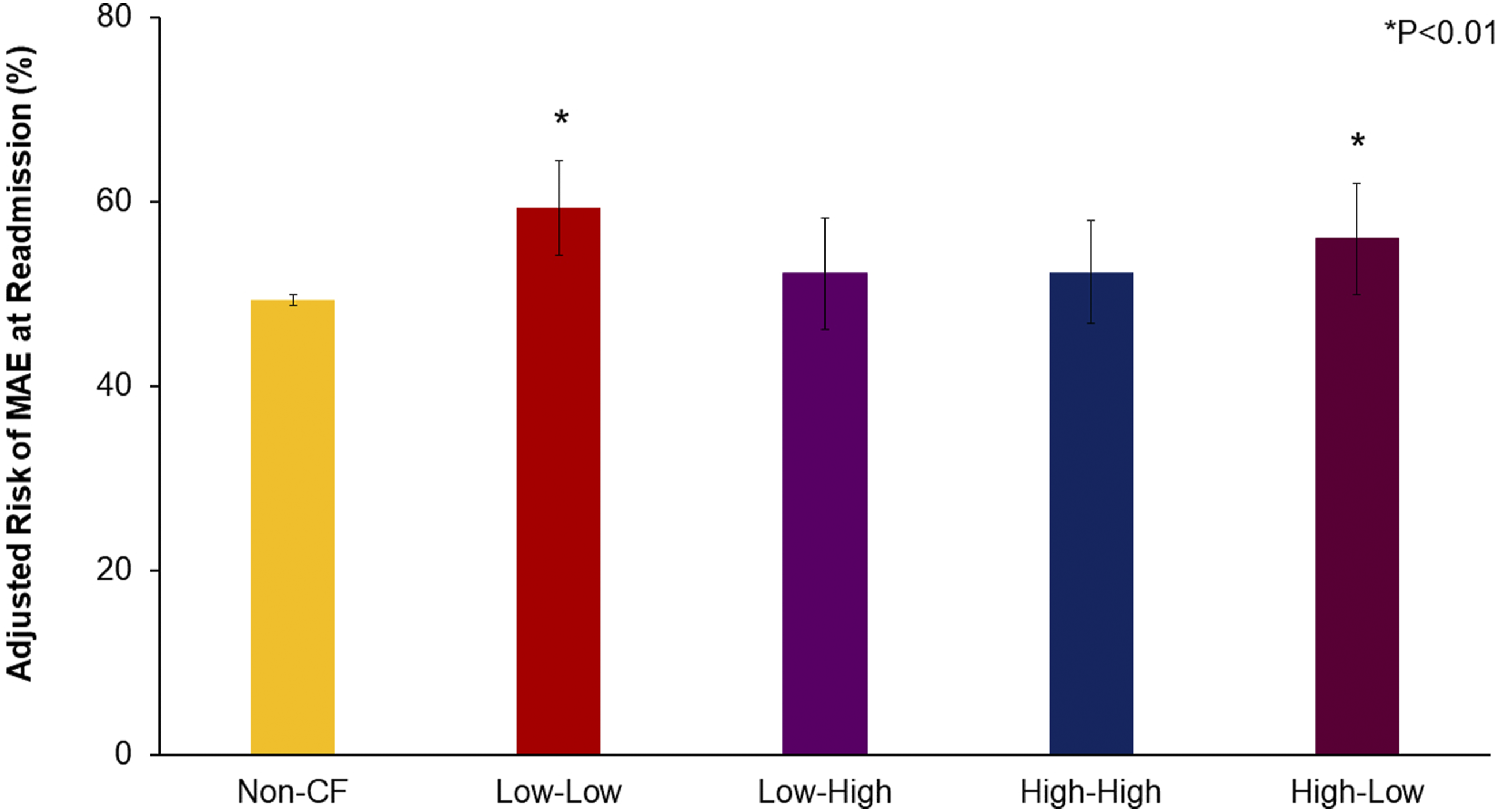
Discussion
In the present national analysis, we considered the impact of care fragmentation on readmission outcomes following colectomy and made several important observations. First, patients experiencing care fragmentation were older, of a higher comorbidity burden, and more often treated for colorectal cancer, compared to others. Following risk adjustment, care fragmentation remained linked with significantly greater likelihood of perioperative major adverse events, as well as increased hospitalization expenditures. Lastly, we identified that among all patients experiencing care fragmentation, readmission to non-index LQH was associated with significantly inferior clinical and financial outcomes, relative to non-index HQH. With implications towards national policies around centralization of care as well as patient management, several of these findings merit further discussion.
We found care fragmentation to confer significantly greater morbidity at readmission. Specifically, patients readmitted to non-index centers demonstrated increased likelihood of gastrointestinal and respiratory sequelae, acute kidney injury, and need for blood transfusion. These findings, therefore, corroborate prior limited series that considered readmission outcomes among patients undergoing colectomy.4-6 However, it is important to note that patients who suffered a major perioperative event may also, hypothetically, be more likely to experience care fragmentation. Because of this, we find it especially notable that patients experiencing care fragmentation more frequently received a colectomy for cancer. Ongoing centralization of cancer care has led patients to travel significant distances to undergo surgical management at highly specialized centers. Unsurprisingly, increased travel distance has been previously correlated with care fragmentation, with many patients presenting with acute events to local facilities, rather than the operating hospital, in the postsurgical period.7,14,15 However, optimization of care requires multidisciplinary involvement and awareness of the patient’s full treatment history and plan, which may not be easily accessible to local hospitals. Given this, triage efforts should seek to determine whether patients would benefit from transfer to their operating facility for continued management. While transfer itself involves time and resources, minimizing the care discontinuity these patients face may have significant implications for their short- and longer-term outcomes. As care of other complex conditions, including IBD, becomes increasingly centralized, future work should consider the implementation of similar interventions to improve treatment continuity and evaluate the ongoing impact of regionalization on care fragmentation risk.
Notably, we identified care fragmentation to be linked with a ∼$2000 incremental increase in per-patient hospitalization expenditures, despite similar duration of hospitalization. This financial disparity persisted after adjustment for incidence of major complications, indication for readmission, and relevant patient, disease, and hospital factors. We proffer this added cost burden may stem, at least in part, from redundant testing or imaging. 16 Improved information sharing across institutions could minimize the need for duplicate assessments, with the potential for significant cost savings. 17 Further, more efficient communication between clinicians and teams could also avoid potential delays in necessary treatment. Indeed, some have suggested more effective utilization of interhospital health information exchange systems has the potential to increase both the quality and value of care, as well as reduce unnecessary readmissions.16,18
Finally, we noted the quality of readmitting hospital to mediate the independent impact of care fragmentation, such that rehospitalization at LQH was linked with significantly inferior outcomes. While the definition of hospital quality can vary across studies and methodologies, we considered hospital-level rates of major adverse events, in line with previously validated literature. 12 Our analysis revealed readmission to non-index LQH was associated with greater morbidity and expenditures. Taken together, the negative effect of care fragmentation appeared to be augmented by readmission at a low-quality institution. We recognize, however, that in this analysis, we only considered non-elective rehospitalization. Therefore, many patients may not have had choice in their readmission destination, whether due to acuity of presentation, insurance coverage, or limited hospital access. Additionally, with continued centralization of care, avoidance of care fragmentation may not be entirely possible. Rather, efforts should be directed to improve outcomes among this cohort, where possible. For example, patient education on the importance of care continuity, as well as established clinic and follow-up appointments, could reduce rates of care fragmentation and strengthen relationships with the original operating facility. Future work is also needed to elucidate the specific aspects within care fragmentation that most directly contribute to adverse outcomes. This information could be used to guide both in-hospital interventions, as well as inform regional or national health policy.
The present study has several strengths. While previous work has considered the impact of care fragmentation, with conflicting findings, this literature evaluated smaller cohorts, exclusively evaluated Medicare patients, or only considered selected indications for colectomy.19,20 These factors ultimately limit generalizability to the current surgical landscape. In contrast, we analyzed a modern, nationally representative sample of adults undergoing colon resection for both benign and malignant conditions. Additionally, while other studies have considered non-index readmissions en bloc, we present the first analysis, to our knowledge, stratifying care fragmentation following elective colectomy by quality of readmitting institution. Therefore, our work presents the most comprehensive and contemporary analysis of this population, to date.
The present work has several important limitations. As an administrative database, the NRD does not provide granular laboratory, radiographic, or physiologic information nor does it include colonoscopy findings. Further, the NRD uses ICD-10 coding, which can vary based on clinician, hospital, or regional practices. While we could identify patients with colon cancer, we could not ascertain the stage of disease, presence of metastasis, or receipt of chemotherapy. We also could not identify incidence of an anastomotic leak. However, future work should consider the impact of anastomotic leak on readmission and likelihood of experiencing CF. Importantly for this study, we could only characterize the quality of NRD-participating institutions within each calendar year and could not capture readmissions to non-participating centers. We defined quality using risk-adjusted rates of major adverse events; future work could consider alternative metrics. Additionally, the NRD does not detail availability of hospitals nor extent of patient choice in selection of a readmitting facility. Due to the deidentified nature of the database, distance traveled to reach the operating facility was not available. Lastly, we could only tabulate indication for rehospitalization as broader categories and could not pinpoint the precise readmission diagnosis. Despite these limitations, we applied thorough statistical methods and considered a nationally representative sample to enhance the generalizability of our findings.
In conclusion, care fragmentation was associated with greater morbidity and resource utilization upon rehospitalization following elective colectomy. Yet, following stratification of care fragmentation subtypes, readmission to a non-index LQH was linked with significantly inferior outcomes, irrespective of the quality of the original operative center. Given continued emphasis on regionalization of care, novel interventions are warranted to improve care continuity among this cohort. Furthermore, additional studies are needed to more specifically ascertain the factors underlying disparities in outcomes among patients experiencing care fragmentation following colectomy.
Supplemental Material
Supplemental Material - Hospital Quality Mediates Impact of Care Fragmentation Following Elective Colectomy
Supplemental Material for Hospital Quality Mediates Impact of Care Fragmentation Following Elective Colectomy by Sara Sakowitz, Syed Shahyan Bakhtiyar, Saad Mallick, Nam Yong Cho, Shineui Kim, Nguyen Le, Hanjoo Lee, and Peyman Benharash in The American Surgeon™.
Footnotes
Authors’ Note
This study was accepted for Presentation at the Southern California Chapter of the American College of Surgeons Annual Meeting.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.