
Abstract
Background
While cholecystectomy is one of the most common operations performed in the United States, there is a continued debate regarding its prophylactic role in elective surgery. Particularly among patients with peritoneal carcinomatosis who undergo cytoreduction surgery with hyperthermic intraperitoneal chemotherapy (CRS-HIPEC), further abdominal operations may pose increasing morbidity due to intraabdominal adhesions and potential recurrence. This bi-institutional retrospective study aims to assess postoperative morbidity associated with prophylactic cholecystectomy at the time of CRS-HIPEC.
Methods
We performed a bi-institutional retrospective analysis of 578 patients who underwent CRS-HIPEC from 2011 to 2021. Postoperative outcomes among patients who underwent prophylactic cholecystectomy at the time of CRS-HIPEC were compared to patients who did not, particularly rate of bile leak, hospital length of stay, rate of Clavien-Dindo classification morbidity grade III or greater, and number of hospital re-admissions within 30 days.
Results
Of the 535 patients available for analysis, 206 patients (38.3%) underwent a prophylactic cholecystectomy. Of the 3 bile leaks (1.5%) that occurred among patients who underwent prophylactic cholecystectomy, all 3 occurred in patients who underwent a concomitant liver resection. There were no significant differences in hospital length of stay, postoperative morbidity, and number of hospital re-admissions among patients who underwent prophylactic cholecystectomy compared to those who did not.
Conclusion
Prophylactic cholecystectomy in patients undergoing CRS-HIPEC is not associated with increased morbidity or increased bile leak risk compared to historical data. While the benefits of prophylactic cholecystectomy are not yet elucidated, it may be considered to avoid potential future morbid operations for biliary disease.
Key Takeaways
• Patients who undergo prophylactic cholecystectomy at the time of cytoreductive surgery with hyperthermic intra-peritoneal chemotherapy are not at an increased risk of morbidity or hospital length of stay. • Prophylactic cholecystectomy should be considered to avoid potential operative dilemmas in patients who may develop biliary disease in the future.
Introduction
Cholecystectomy is one of the most common operations performed in the United States, occurring between 400,000 and 750,000 times per year. 1 The introduction of laparoscopic cholecystectomy has increased the rate of cholecystectomy among patients with a variety of biliary diseases.2,3 Although overall mortality associated with cholecystectomy is minimal, morbidity is variable ranging from surgical site infection to common bile duct injury. Bile leak after laparoscopic cholecystectomy is estimated to be between 1% and 4%, while open cholecystectomy infers a lower incidence of bile leak of about .5%–1%.4-6
Many studies have shown that prophylactic cholecystectomy is not associated with increased morbidity among patients undergoing various operations with different underlying diseases, including small bowel neuroendocrine tumor, hepatocellular carcinoma, and gastric cancer, among others.7-10 However, no study has evaluated the morbidity of prophylactic cholecystectomy among patients with peritoneal carcinomatosis undergoing cytoreductive surgery with hyperthermic intraperitoneal chemotherapy (CRS-HIPEC). The frequency at which CRS-HIPEC is performed in the United States is increasing as emerging data show that CRS-HIPEC improves survival in select patients with peritoneal carcinomatosis due to appendiceal, colorectal, and ovarian cancer.
Patients with peritoneal carcinomatosis are predisposed to postoperative morbidity in the elective or acute setting, given their disseminated disease and associated frailty and comorbidities. Given the high incidence of biliary disease requiring cholecystectomy and increasing frequency of CRS-HIPEC, an increasing number of patients with potential disseminated cancer will require cholecystectomy after CRS-HIPEC. Thus, prophylactic cholecystectomy may prevent the potential morbidity of future cholecystectomy in this patient population.
Thus, the primary objective of this study is to examine the postoperative morbidity of prophylactic cholecystectomy at the time of CRS-HIPEC among patients with peritoneal carcinomatosis.
Methods
Data Sources and Definitions
Data were retrospectively obtained from a prospectively maintained database of all patients who underwent CRS-HIPEC with curative intent between 2011 and 2021 from 2 cancer centers after receiving approval from our institutional review board (IRB #200638). The database was used to collect patient demographic information, baseline oncologic characteristics, and operative details. Patients were excluded if they had previously undergone a cholecystectomy prior to CRS-HIPEC. Patients were divided into 2 groups based on whether or not a prophylactic cholecystectomy was performed at the time of CRS-HIPEC: the prophylactic cholecystectomy group (PCY) consisted of patients who did, while the control group (CONT) consisted of patients who did not based on the operative report. Patients were excluded from the study if they had previously undergone a cholecystectomy prior to CRS-HIPEC. The presence of a bile leak was derived from daily progress notes and the patient’s discharge summary. Postoperative hospital length of stay, rate of Clavien-Dindo III/IV complication, and number of hospital readmissions within 30 days of discharge were compared between the 2 groups.
Statistical Analysis
Categorical variables were compared using Chi-squared test, and continuous variables were expressed as means and compared using Mann-Whitney U test. All analyses were performed using the IBM Statistical Package for the Social Sciences for Mac, Version XX (IBM Corp., Armonk, NY, USA).
Results
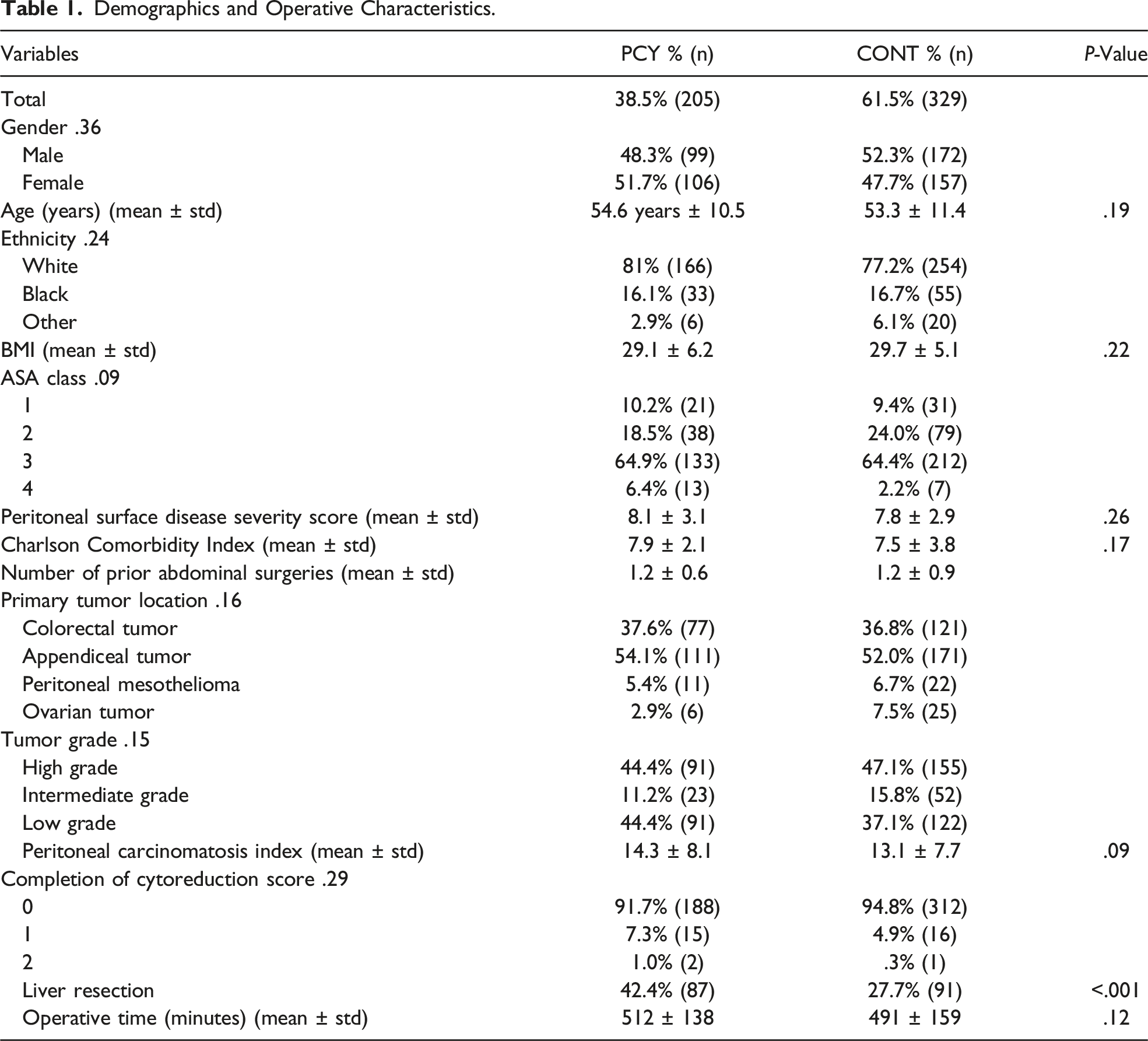
Patient and Operative Characteristics
Demographics and Operative Characteristics.
Postoperative Complications
Postoperative Outcomes.

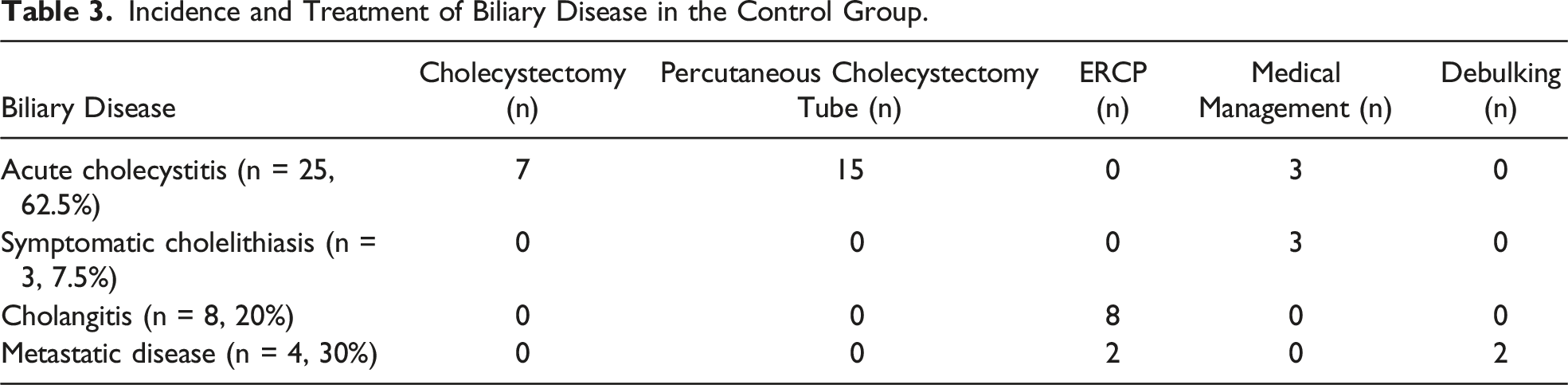
Incidence and Treatment of Biliary Disease in the Control Group.
Discussion
In this bi-institutional retrospective study, we observed that prophylactic cholecystectomy among patients undergoing CRS-HIPEC is associated with a 1.5% risk of bile leak, which occurred in 3 patients all of whom underwent concomitant liver resection. This rate of bile leak was similar to the bile leak rate in the CONT group in patients who underwent liver resection. This is comparable to historical data for rate of bile leak after open or laparoscopic cholecystectomy. Additionally, prophylactic cholecystectomy did not incur a significantly longer operative time, hospital length of stay, postoperative morbidity, or increase in hospital re-admission within 30 days compared to patients who did not undergo prophylactic cholecystectomy at the time of CRS-HIPEC in this patient cohort. Furthermore, all bile leaks in the PCY group occurred in patients who underwent a concomitant liver resection and were managed with endoscopic biliary drainage. Patients in the control group had a similar rate of bile leaks, indicating that the likely cause of bile leaks in the PCY group were related to the concomitant liver resection, rather than the cholecystectomy, and does not increase morbidity.
These data are consistent with historical data regarding the incidence of bile leak after open cholecystectomy.4,6 Furthermore, several studies have affirmed the relative safety of prophylactic cholecystectomy at the time of oncologic surgery. The CHOLEGAS randomized control trial conducted among patients undergoing gastrectomy for cancer showed a bile leak rate of 1.5% in their experimental group with no differences in operative duration, hospital length of stay, or postoperative morbidity. 8 Relatedly, a retrospective NSQIP study of 1300 patients undergoing small bowel resection for small bowel neuroendocrine tumor showed no difference in postoperative morbidity or mortality but did show significantly increased operative times when prophylactic cholecystectomies were performed. 9
As the treatment of peritoneal carcinomatosis has improved over the last several decades, the number of people living with disseminated cancer who then develop biliary disease is also increasing. The safety of cholecystectomy has been well-established, but little data exists for outcomes following cholecystectomy in patients with disseminated cancer. A recent NSQIP study of over 3000 patients examined postoperative outcomes after cholecystectomy in patients without cancer compared to those with disseminated cancer found that patients with cancer sustained higher rates of wound infections, cardiopulmonary complications, longer hospital length of stay, and higher 30-day mortality. 11 Thus, patients who have a high rate of cancer recurrence or continued systemic therapy may benefit from prophylactic cholecystectomy at the time of CRS-HIPEC to avoid heightened operative risk should they develop biliary disease in the future. While the present study did not aim to quantify the risk associated with cholecystectomy after CRS-HIPEC, 12.1% of patients developed biliary disease, the majority of whom were managed nonoperatively. This observation suggests there may be hesitancy among surgeons to offer cholecystectomy in patients with biliary disease after previously undergoing CRS-HIPEC. Additionally, nearly 10% of patients had tumor involvement of the gallbladder, suggesting that prophylactic cholecystectomy may aid in accomplishing a complete cytoreduction even when not obviously involved with disease.
The limitations of this study revolve mainly around its retrospective nature and sample size. Although this is the largest analysis of prophylactic cholecystectomy at the time of CRS-HIPEC, bile leaks after cholecystectomies are rare. This retrospective study describes the relative safety of concomitant prophylactic cholecystectomy at the time of CRS-HIPEC with potential to reduce perioperative morbidity should these patients develop biliary disease in the future. Given that biliary disease is the most common surgical disease in the United States, further studies are needed to identify specific patients who would derive benefit from prophylactic cholecystectomy, particularly among those with disseminated cancer who undergo CRS-HIPEC.
Nonetheless, the data in this large retrospective study suggests that prophylactic cholecystectomy at the time of CRS-HIPEC is safe, does not significantly prolong operative time, hospital length of stay, does not increase postoperative morbidity, and should be considered for patients who may develop biliary disease in the future.
Footnotes
Acknowledgments
We would like to acknowledge our funding source, the National Cancer Institute (T32CA106183).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We would like to acknowledge our funding source, the National Cancer Institute (T32CA106183).