
Abstract
Temporal artery biopsy (TAB) is the standard test for diagnosing giant cell arteritis. Our objective was to determine which specialists perform TABs and if there is variation across the United States. We performed a cross-sectional analysis in a multi-state health care system, evaluating differences between observed counts of surgical specialty by region, positive diagnoses by region, and positive diagnoses by specialty. Temporal arterial biopsy was performed on 3825 patients with the proportion of specialties performing TAB differing between regions. Temporal artery biopsy was performed by a significantly higher percentage of general surgeons in the Midwest (53.6%) and less vascular surgeons in the West (30.4%). The percentage of positive diagnoses was higher for vascular surgeons (32.7%). We concluded that TAB is performed by physicians of many specialties with the specialty performing most of these procedures varying by region. There is also a difference in the rate of positive diagnoses that varies with surgical specialty.
Temporal artery biopsy (TAB) is the gold-standard test for diagnosing giant cell arteritis (GCA), an auto-immune vasculitis affecting larger-diameter blood vessels with a predisposition to cranial arteries. 1 The main treatment for this condition involves high-dose steroids, which can come with a litany of side effects (eg, Cushing syndrome, immunosuppression, hepatic damage, or peptic ulcers). The current American College of Rheumatology’s diagnostic criteria include age greater than 50 years, temporal artery tenderness, new-onset localized headache, morning stiffness in shoulders/neck, erythrocyte sedimentation rate >50 mm/h, and positive TAB, with a score of equal to or greater than 6 meeting the classification for GCA. 2 Temporal artery biopsy can be performed by physicians from a variety of specialties including ophthalmologists, dermatologists, otolaryngologists, general surgeons, neurosurgeons, vascular surgeons, and potentially others. As a result of the broad range of specialists who perform the procedure, there is great variability in the training received to perform the procedure. 3 Furthermore, some of these aforementioned specialists may receive no formal training on the performance of TAB but receive referrals or consultations to perform it based on practice patterns in their health care system. Although TAB is generally considered a safe procedure, proper training and appropriate procedure volume are important to mitigate unnecessary complications (ie, facial nerve injury, stroke, and scalp necrosis) in practice. 3 We aimed to elucidate the specialties most likely to perform TAB and to determine the percent TAB positivity among physicians in different specialties. We conducted a retrospective cross-sectional analysis across 182 hospitals within the HCA Healthcare System over a 6-year period between January 1, 2016, and December 12, 2022. All patients >18 years old undergoing temporal artery biopsy were included in our data set. Data were extracted from the HCA Healthcare electronic data warehouse which contains patient data from the electronic medical records at 182 hospitals. Specialties reported in the EMR were grouped: CT_SURG; thoracic and cardiothoracic surgery, ENT_OPHTH; ophthalmology and otolaryngology, GEN_SURG; general surgery, bariatric surgery, colorectal surgery, trauma surgery, transplant surgery, and surgical oncology, MULTIPLE; multiple specialties of interest, NEURO; neurosurgery, and VASC_SURG; vascular surgery. Data were categorized by region, in alignment with US Census divisions into the Midwest, Northeast, South, and West. Chi-square analyses were performed to compare differences in observed counts of surgical specialty by region, as well as positive diagnoses by region and differences in positive diagnoses by reported specialty. From the total population of patients (N = 3825), 1100 records included procedure time, which was evaluated using an ANOVA to compare means of procedure time against reported specialty. A covariance matrix with unequal group variances was used due to differences in group sizes.
Positive Diagnosis by Specialty (Chi-Square Tests) Inclusive Dates January 1, 2016, and December 12, 2022 (N = 3825).
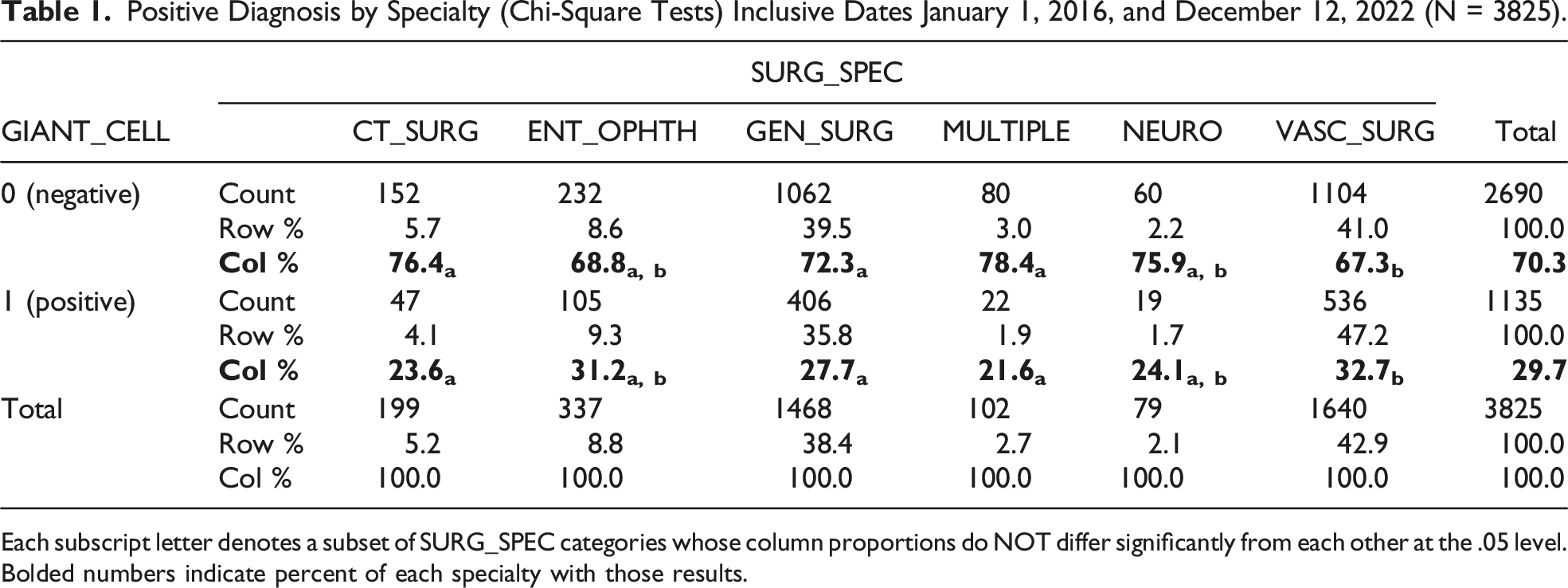
Each subscript letter denotes a subset of SURG_SPEC categories whose column proportions do NOT differ significantly from each other at the .05 level. Bolded numbers indicate percent of each specialty with those results.
In conclusion, temporal artery biopsies are performed by a variety of surgical disciplines across different regions of the United States. The majority of these procedures were performed by general surgeons and vascular surgeons, in the Northeast and Midwest with otolaryngologists and ophthalmologists adding substantially to the total in the South and West. Future research may investigate whether formal training in temporal artery biopsy procedures exists within their respective residency curricula. There also exists a significant difference in the rate of positive diagnosis by surgical discipline, highlighting an avenue for further study in order to assess whether this can be attributed to a function of referral pattern or surgical training and experience.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported (in whole or in part) by HCA Healthcare and/or an HCA-affiliated entity.