
Abstract
Background
Patients with Graves’ Disease often have a larger thyroid size than patients without thyroid disease. These patients also have elevated T3 and T4 with decreased TSH.
Purpose
We evaluate whether these thyroid labs, the use of antithyroid agents, or the size of a thyroid on ultrasound, correlate with the pathological size of a thyroid in patients who undergo total thyroidectomy for Graves’ Disease. We further determine whether these parameters affect perioperative complications.
Research Design
A retrospective review of patients undergoing total thyroidectomy for Graves’ Disease was performed from January 2004 to December 2016 in a single institution.
Study Sample
392 patients were included in the study.
Data Collection and/or Analysis
Univariate analyses were performed to compare thyroid size on US and pathology as well as weight to preoperative thyroid hormone values and medical comorbidities. Spearman rank correlation and ANOVA were used to identify factors associated with thyroid weight, total pathology size, and differences in size. Multivariate analysis was also performed to evaluate for correlation between thyroid function and perioperative complications.
Results
We found that elevated pre-operative T3 levels were associated with larger pathologic size (P = .027) and a greater difference in pathology vs. US thyroid volumes (P = .005), but not increased thyroid weight (P = .286). No significant differences were found for thyroid weight, pathology size, or difference in size for TSH, T4, or any specific preoperative ATD given. Only postoperative calcium levels were found to be statistically significant for TSH < 0.27 (P = .024) for peri-operative complications.
Conclusions
These findings may allow for more accurate preoperative planning and intraoperative expectations in patients with Graves’ Disease.
Key Takeaways
• Preoperative T3 levels may correlate with thyroid size, whereas TSH and T4 levels, use of antithyroid medications, and patient’s past medical history do not have an effect. • It may be beneficial to obtain a patient’s T3 level just prior to surgery, as this may be most predictive in the patient’s actual thyroid size intraoperatively. • Intraoperative factors, including nerve identification, blood loss, incidental parathyroid glands removed, and estimated blood loss as well as postoperative morbidity, do not correlate with preoperative T3 levels
Introduction
The average size and weight of the thyroid gland tend to be higher in patients with an underlying pathology, such as Graves’ disease (GD), Hashimoto’s thyroiditis, or multinodular goiters. 1 While certain ultrasound characteristics correlate with thyroid function in children with autoimmune thyroid disorders, ultrasound (US) characteristics, and pathologic thyroid size in adults with GD have not been evaluated. 2 Additionally, the severity of GD oftentimes correlates with T3 levels, but it has not been shown whether this has any correlation on the size of the thyroid gland. 1
GD patients are commonly prescribed anti-thyroidal drugs (ATDs), including methimazole, propylthiouracil (PTU), beta-blockers, steroids, or sodium saturated potassium iodide (SSKI), which have been shown to decrease thyroid gland vascularity. 3 ATDs may control preoperative thyroid hormone levels, but only SSKI has been used to decrease gland vascularity and improve thyroid function tests, resulting in decreased intraoperative estimated blood loss. 3 While the ATA guidelines recommend giving SSKI, improved postoperative outcomes have not been consistently proven with its use. In addition, there are currently no studies that evaluate whether the use of these ATDs have an effect on the size of the thyroid gland. Thyroid size is important in preoperative planning as larger thyroid size may increase the complexity of the operation. The aim of our study is to evaluate factors that may correlate with increased size on US, pathology, and weight in GD patients who undergo total thyroidectomy (TT), including preoperative lab values and the use of ADTs, and to determine whether these factors have an impact on surgical outcomes.
We hypothesized that elevated T3 and T4 as well as decreased TSH would correlate with increased thyroid size, and that increased thyroid size would lead to increased intraoperative and postoperative complications. In other words, we hypothesized that higher T3 levels would correlate with a higher rate of surgical complications.
Methods
Appropriate IRB approval was obtained as this study was deemed as exempt. A retrospective review of patients undergoing TT was performed from January 2004 to December 2016. Patients were included if they were 18 years of age or older and underwent TT for a diagnosis of GD. GD diagnosis was given when the patient had either a free T3 greater than 4.2, free T4 greater than 1.48, or TSH less than .27. Diagnosis could also be obtained if positive thyroid receptor antibodies were present or if patients presented with thyrotoxicosis or two outpatient diagnoses of thyrotoxicosis, hyperthyroidism, or GD. Although preoperative thyroid function data was easily accessible, numerous patients were diagnosed outside of the studied hospital system. Because of this, exact values for thyrotropin receptor antibody (TRAb), thyroid stimulating immunoglobulin (TSI), and anti-thyroid peroxidase (TPO) antibodies were unable to be reliably obtained.
Patients were excluded if they underwent surgeries other than TT (including lobectomy, subtotal thyroidectomy, or prior thyroid surgery), if surgery was not performed within our health system, or if they had concomitant other procedures.
Patient demographics including age, gender, and Charlson Comorbidity Index (CCI) were evaluated. Medical comorbidities evaluated included congestive heart failure (CHF), cardiopulmonary disease (CPD), cardiovascular disease (CVD), myocardial infarction (MI), liver disease, and peripheral vascular disease (PVD). Preoperative TSH, T3, and T4 were obtained as well as utilization of preoperative medications, including SSKI, beta-blockers, steroids, methimazole, and PTU. Thyroid US and pathology sizes were compared. Thyroid size was determined by preoperative US as well as postoperative pathological measurements. Volume was calculated as V (mL) = .479 x Depth x Width x Length (cm). Thyroid weight was also recorded.
Univariate analyses were performed to compare thyroid size on US and pathology as well as weight to preoperative thyroid hormone values and medical comorbidities. Spearman rank correlation and ANOVA were used to identify factors associated with thyroid weight, total pathology size, and differences in size. All statistical tests were two sided with a P value of less than .05 considered to be statistically significant. Analyses were performed using SAS 9.4 (SAS Institute, Cary, NC).
Ease of surgical dissection was identified by intraoperative factors including surgical duration, estimated intraoperative blood loss (EBL), inadvertent parathyroid tissue removal, and ability to identify the recurrent laryngeal nerve. Recurrent laryngeal nerve injury was noted when documented by the performing surgeon or clinical team. Postoperative factors evaluated included postoperative hypocalcemia, recurrent laryngeal nerve injury, and hospital length of stay. Final pathology specimens were evaluated for presence of cancer as well as number of inadvertent parathyroid glands removed. A diagnosis of hypocalcemia was made if “hypocalcemia” was documented in the patient’s chart, the patient needed IV calcium replacement, or was prescribed Calcitriol postoperatively.
Univariate analysis was also performed comparing patient demographics with lab values consistent with poor hormone control to those euthyroid/hypothyroid: TSH <.27 vs normal or >4.2; T3 >4.3 vs <2.5 or normal; and T4 > 1.7 vs <.7 or normal. Intraoperative and postoperative variables were also compared. Multivariate analysis was then performed to evaluate for correlation between TSH, T3, and T4 with patient factors associated with EBL, surgical duration, ability to identify the RLN, and inadvertent removal of parathyroid glands (as identified by reimplantation or pathology report). Multivariate analysis was also performed to compare preoperative hormone levels to postoperative complications including hypocalcemia, RLN injury, and length of stay.
Results
392 patients were included in the study, and 233 of these patients had thyroid size data from US and pathology available for comparison. Average age was 46.8 years old (+/- 16.18 years). Mean BMI was 29 (+/- 7.21). 196 (84.1%) were female. CCI was 0 for 97 patients (41.6%), 1 for 50 patients (21.5%), 2 for 39 patients (16.7%), 3+ for 46 patients (19.7%), and 1 (.4%) was unknown. 11 (4.7%) had CHF, 62 (26.6%) had CPD, 16 (6.9%) had CVD, 2 (.9%) had a history of MI, 6 (2.6%) had mild liver disease, none had severe liver disease, and 14 (6.0%) had PVD. Comorbid condition data was missing for 1 patient for all comorbidities. The length of time from the labs and ultrasound being obtained to the patient undergoing surgery was also determined. The median length of time from TSH level drawn to surgery was 36 days with an interquartile range (IQR) of 10-71, T3 to surgery was 40 days (IQR 12-81), and T4 to surgery was 34 days (IQR 9-70). Median length of time from undergoing thyroid US to surgery was 121 days (IQR 56-273).
Preoperative TSH was normal in 66 patients (28.3%), <.27 for 155 (66.5%), >4.2 for 8 (3.4%), and unknown for 4 (1.7%). Preoperative T3 was normal for 118 patients (50.6%), <2.5 for 19 (8.2%), >4.3 for 74 (31.8%), and unknown in 4 (1.7%). Preoperative T4 was normal for 159 patients (68.2%), <.7 for 14 (6.0%), >1.7 for 56 (24%), and unknown for 4 (1.7%). Preoperative TSH was available for 387 (98.7%) patients, T3 data was available for 355 (90.6%) patients, and T4 data was available for 382 (97.4%) patients. 163 patients (70.0%) took methimazole preoperatively, 31 (13.3%) took PTU, 82 (35.2%) took SSKI, and 21 (9.2%) took steroids preoperatively.
Mean pathology volume was 56.95 ± 53.15 mL (right 28.96 ± 26.79 mL, left 27.98 ± 32.68 mL, and isthmus .88 ± .49 mL). Median thyroid weight was 31.5 grams (range 19.28-52.00 grams). Mean thyroid US volume was 31.3 ± 25.73 mL (16.7 ± 14.82 mL for the right, 14.56 ± 14.45 mL for the left, .71 ± .71 mL for the isthmus). Pathology volumes were found to be significantly higher than US volumes (P < .0001). The right side was significantly larger on both pathology (P = .0037) and US (<.0001).
Univariate Analysis of Patient Characteristics on Thyroid Weight, Increased Pathologic Volume, and Difference in Pathology vs US Volumes.
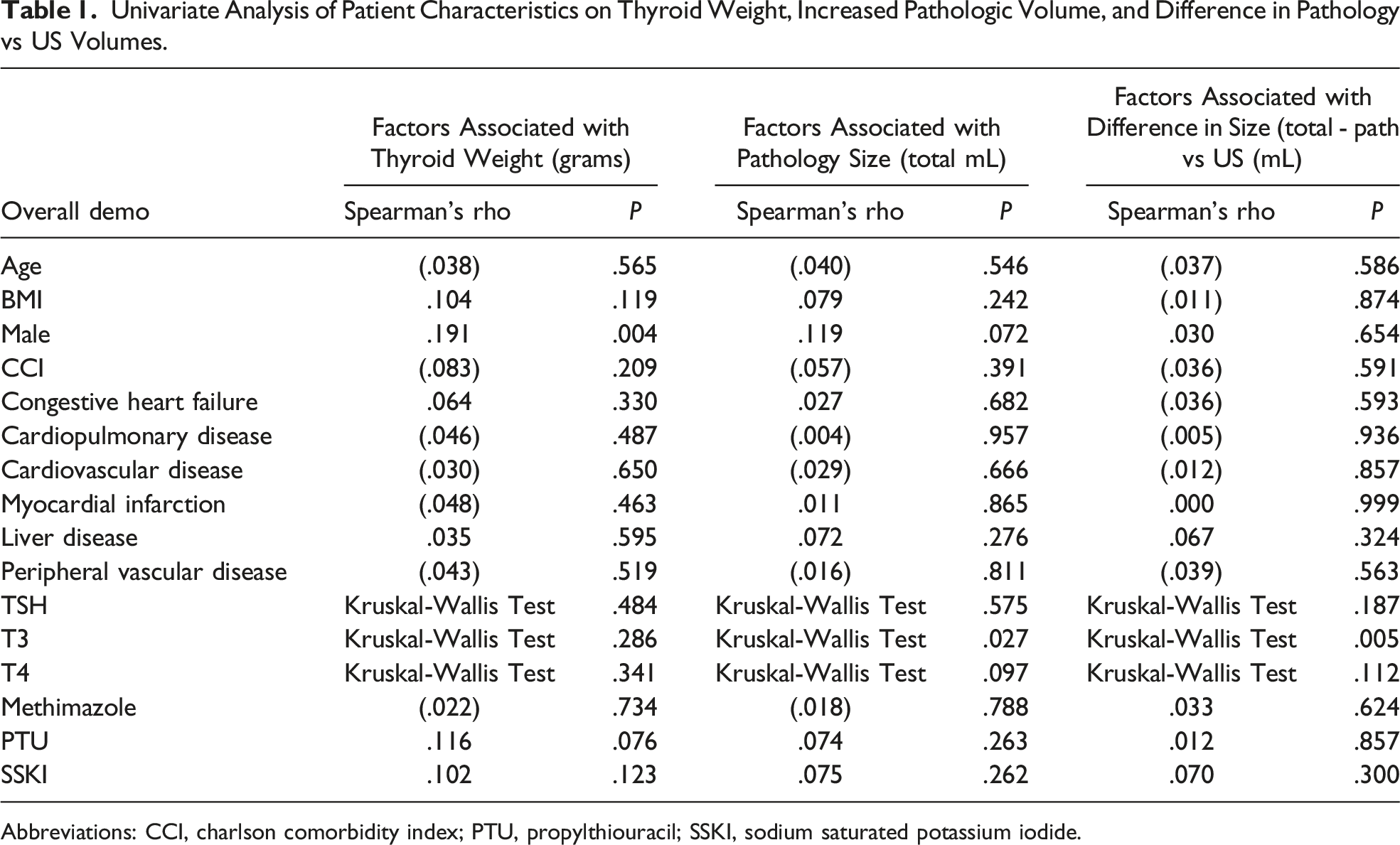
Abbreviations: CCI, charlson comorbidity index; PTU, propylthiouracil; SSKI, sodium saturated potassium iodide.
Univariate Analyses of TSH vs Patient Demographics and Preoperative Treatments.
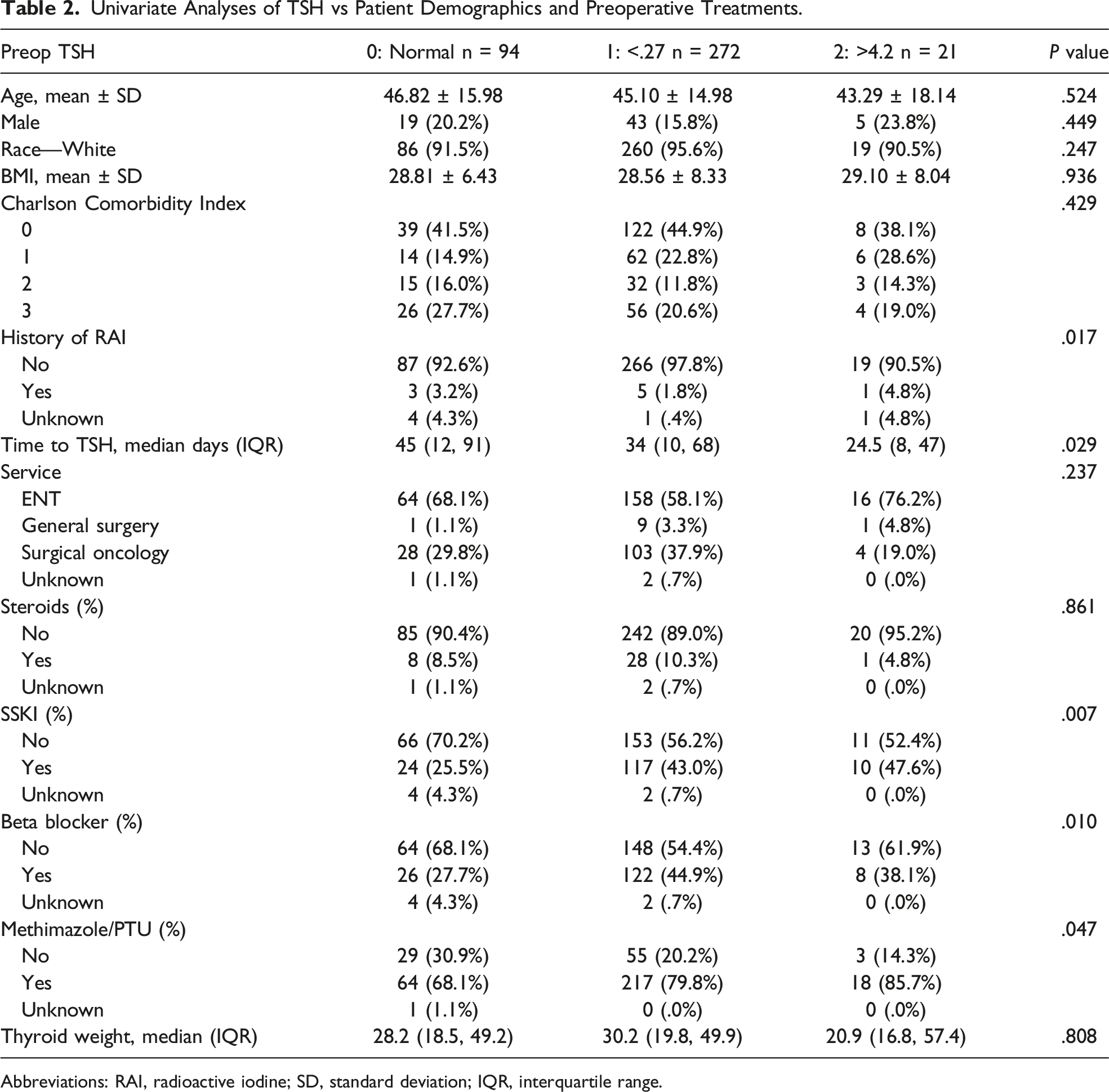
Abbreviations: RAI, radioactive iodine; SD, standard deviation; IQR, interquartile range.
Univariate Analyses of T3 vs Patient Demographics and Preoperative Treatments.
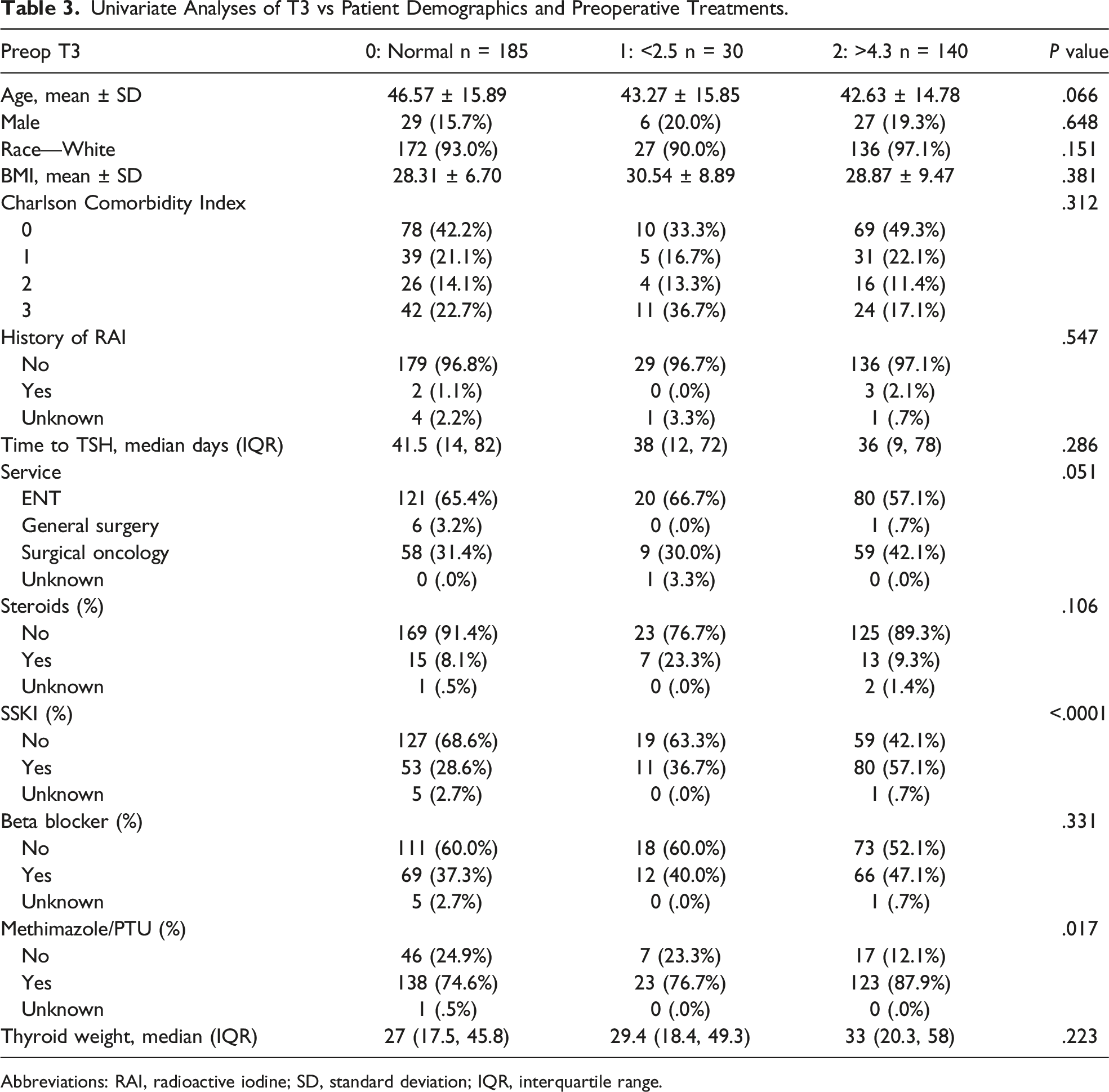
Abbreviations: RAI, radioactive iodine; SD, standard deviation; IQR, interquartile range.
Univariate Analyses of T4 vs Patient Demographics and Preoperative Treatments.
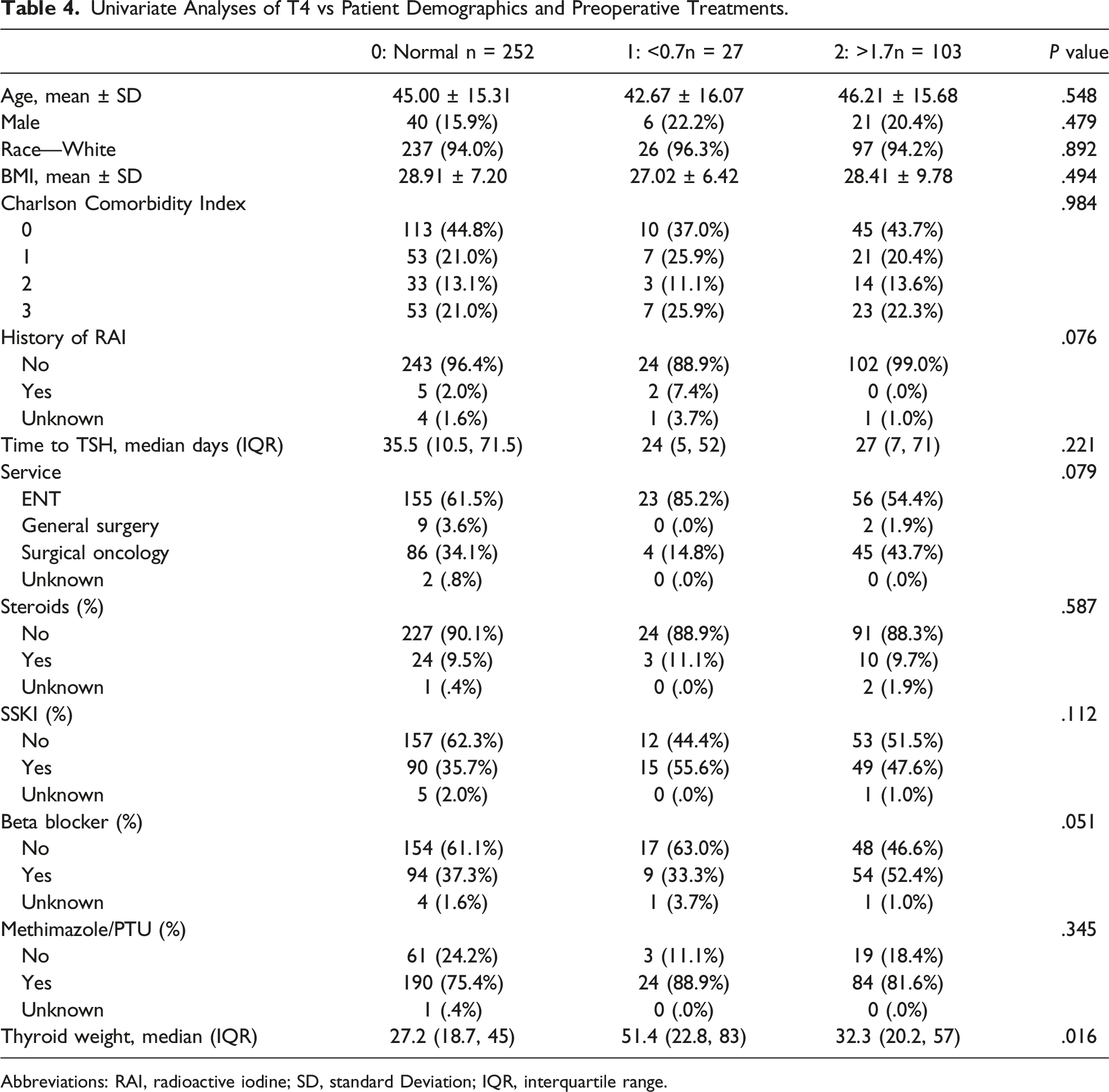
Abbreviations: RAI, radioactive iodine; SD, standard Deviation; IQR, interquartile range.
Median EBL was 20 mL (range 5-300 mL). The recurrent laryngeal nerve was identified in 381 (97.4%) of patients. Parathyroid tissue was removed inadvertently in 77 (23.2%) patients. Average surgical duration was 141.6 minutes (±61.9 minutes). Median length of stay was 2 days. Recurrent laryngeal nerve injury was diagnosed in 3 patients (.8%) and postoperative hypocalcemia was diagnosed in 73 patients (18.6%).
Pre-op TSH and Outcomes.
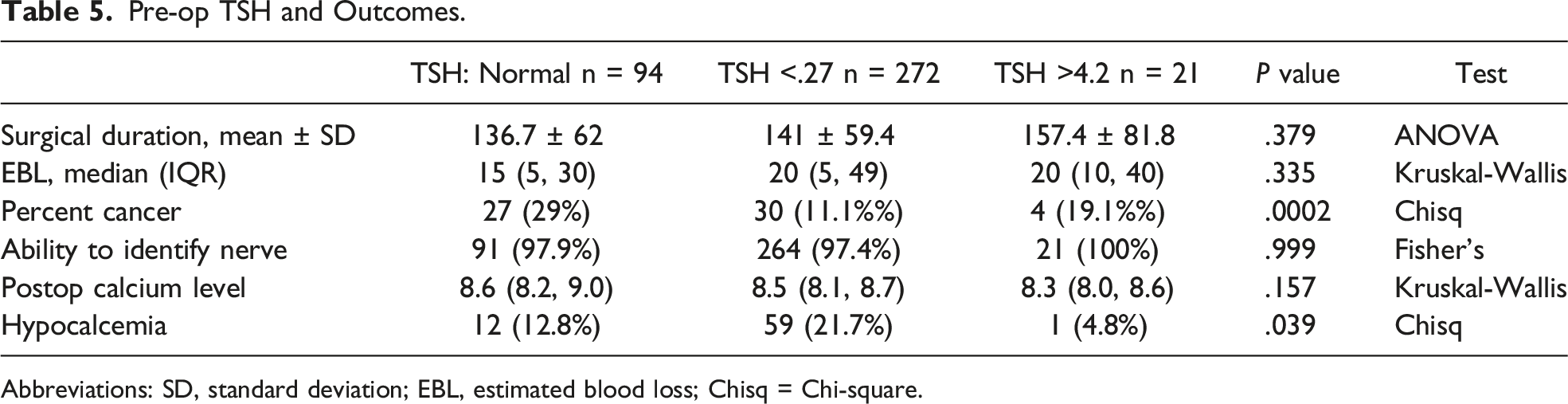
Abbreviations: SD, standard deviation; EBL, estimated blood loss; Chisq = Chi-square.
Pre-op T3 and Outcomes.
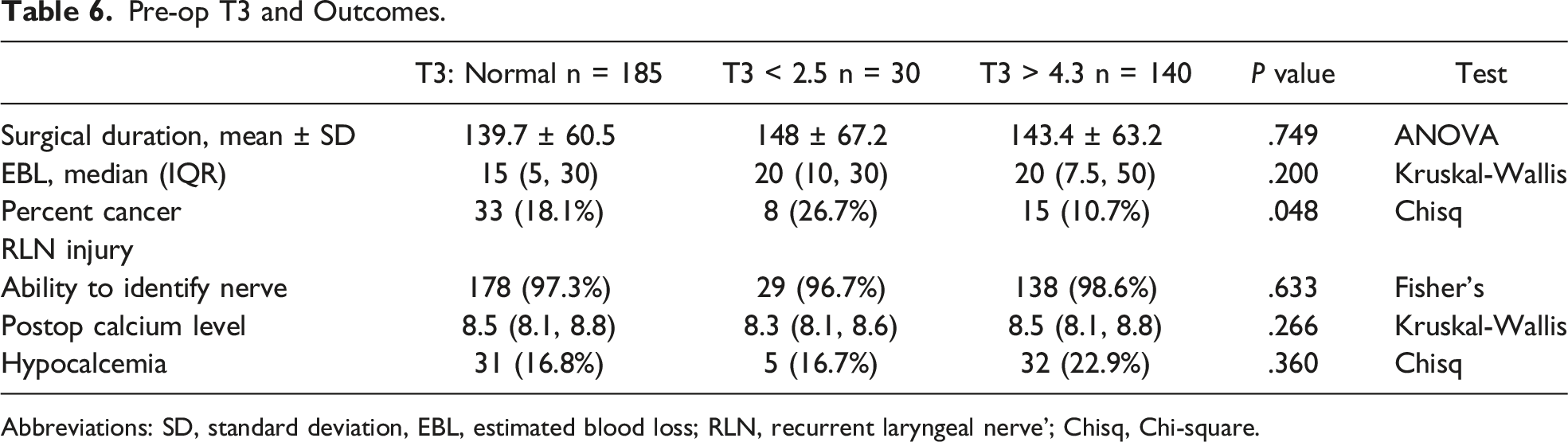
Abbreviations: SD, standard deviation, EBL, estimated blood loss; RLN, recurrent laryngeal nerve’; Chisq, Chi-square.
Pre-op T4 and Outcomes.
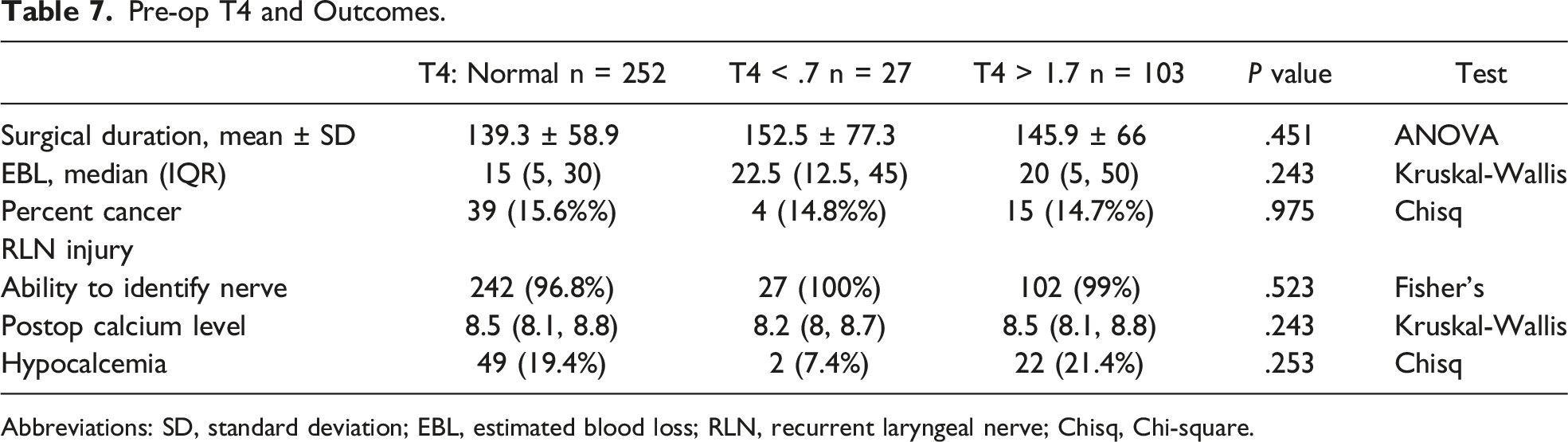
Abbreviations: SD, standard deviation; EBL, estimated blood loss; RLN, recurrent laryngeal nerve; Chisq, Chi-square.
Discussion
The aim of this study was to determine if there was a correlation between a patient’s thyroid lab values (TSH, T3, and T4), the use of antithyroid medications, or preoperative thyroid volume based on ultrasound and the pathological size of the thyroid and these effects on surgical complications. Although it has been shown that certain ultrasound characteristics in children correlate with thyroid function and that GD severity correlates with T3 levels, there have not been any studies that determine whether T3, T4, and TSH levels, as well as antithyroid medications have an effect of the pathological size of the thyroid.1,2
Our study showed that only T3 correlated with total thyroid size on pathology and change in size from US to pathology, whereas TSH and T4 levels, use of antithyroid medications, and patient’s past medical history do not have an effect. Furthermore, pathology volumes were significantly higher than US volumes, and time to surgery from US and preoperative lab values were longer than expected. This study shows that it may be beneficial to obtain a patient’s T3 level just prior to surgery, as this may be most predictive in the patient’s actual thyroid size intra-operatively. This may then be used to determine the overall complication of thyroid dissection as well as post-operative complication rate as prior studies have found that in patients with GD who underwent surgical intervention, those with higher thyroid weight had a higher complication rate, including a higher cancer recurrence risk, persistence of disease, and mortality. 4 Although there have been studies showing that thyroid stimulating antibodies can be used to predict response to methimazole, and others showing that thyroid antibody use could be used to assess recurrence, there have been no studies evaluating thyroid antibody to size.6-8 However, we were unable to study specific thyroid antibodies due to a large number of our cohort being diagnosed outside of our hospital system. Future research may help determine this relationship. Overall, our findings may allow for more accurate preoperative planning and intraoperative expectations in patients with GD.
While the ATA recommends patients be euthyroid prior to thyroidectomy, this is often not possible due to the need for thyroid surgery secondary to intolerance of ATDs. Additionally, thyroidectomy remains the treatment of choice when other treatment modalities fail. 5 Although SSKI use may decrease vascularity of the thyroid gland, thereby contributing to decreased intraoperative morbidity, the use of SSKI has not been shown to correlate with thyroid gland size in our study. 3 We questioned if preoperative thyroid function may help predict more active glands, also leading to increased surgical difficulty. However, intraoperative factors (which included nerve identification, blood loss, incidental parathyroid glands removed, estimated blood loss, etc.) and postoperative morbidity did not correlate with preoperative T3 levels. While significant differences were seen in those taking SSKI and Methimazole/PTU for TSH and T3, these medications were not associated with preoperative T4 levels in our study.
Limitations to this study include that it was performed in a single institution with a relatively small sample size of 392. Furthermore, the time from obtaining preoperative lab values (TSH, T3, and T4) was longer than anticipated. Obtaining these lab results closer to the date of surgery could have more accurately allowed us to assess the effects of ATDs on thyroid size. While patients selected for this study all required thyroidectomy, different indications for surgery were used in our patient population, which allowed comparisons of groups of those that were hormone controlled vs not hormone controlled. Our population was therefore not biased to patients needing surgery for poor hormone control.
In conclusion, T3 levels correlate with pathological thyroid size, and there may be benefit in obtaining a T3 level closer to the date of surgery to more accurately predict this, but increased T3 levels do not correlate with intraoperative or post-operative complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.