
Abstract
Background
Thyroid storm is a rare but potentially lethal manifestation of thyrotoxicosis. Guidelines recommend nonoperative management of thyroid storm, but thyroidectomy can be performed if patients fail medical therapy or need immediate resolution of the storm. Outcomes of thyroidectomy for management of thyroid storm remain ill-defined.
Methods
Using the National Inpatient Sample from 2016 to 2020, a retrospective analysis was conducted of patients admitted with thyroid storm. Outcomes of interest included operative complications and mortality. Multivariable logistic regression was performed to assess factors associated with receiving thyroidectomy and mortality.
Results
An estimated 16,175 admissions had a diagnosis of thyroid storm. The incidence of thyroid storm increased from .91 per 100,000 people in 2016 to 1.03 per 100,000 people in 2020, with a concomitant increase in mortality from 2.9% to 5.3% (P < .001). Operative intervention was pursued in 635 (3.9%) cases with a perioperative complication rate of 30%. On multivariable regression, development of acute decompensated heart failure (adjusted odds ratio [AOR] 1.66, 95% Confidence Interval [CI] 1.03-2.68, P = .037) and acute renal failure (AOR 2.10, 95% CI 1.17-3.75, P = .013) increased odds of receiving surgery. The same multivariable model did not show a significant association between thyroidectomy and mortality.
Discussion
The incidence of thyroid storm and associated mortality increased during the study period. Thyroidectomy is rarely performed during the same admission, with an overall perioperative complication rate of 30% and no effect on mortality. Patients with acute decompensated heart failure and renal failure were more likely to receive an operative intervention.
Key Takeaways
• Incidence and mortality rate of thyroid storm are increasing in the United States. • Thyroidectomy was performed in less than 4% of admissions, with comparable perioperative complication rates to non-emergent thyroidectomies. • Patients who developed acute decompensated heart failure and acute renal failure were more likely to receive operative intervention.
Introduction
Thyroid storm is an acute and life-threatening form of thyrotoxicosis caused by the excess release or response to thyroid hormone.1-3 Among patients with hyperthyroidism, .22% develop thyroid storm, accounting for ∼1%-2% of all hospitalizations nationwide.1,3 The point at which thyrotoxicosis becomes thyroid storm remains controversial, but it commonly leads to multiorgan failure and requires emergent treatment. Thyroid storm is clinically diagnosed, relying on manifestation of the multiorgan involvement, such as severe tachycardia (>130 BPM), fever (>38°C), respiratory failure, delirium, and gastrointestinal symptoms. The mortality of thyroid storm has been reported to be as high as 75%-100% when untreated and even with treatment persists at 10%-30%.1,3
Treatment of thyroid storm is primarily pharmacologic. Mainstays of treatment are anti-thyroid drugs, methimazole or propylthiouracil, to inhibit hormone synthesis and release, β-blockers and corticosteroids to reduce the effects of circulating hormones, and supportive care.1-4 Close monitoring in the intensive care unit is generally recommended. 4 Thyroidectomy is rarely pursued and typically reserved for patients who continue to worsen despite maximum medical management. 1 Thyroidectomy produces rapid resolution of hyperthyroidism and allows patients to discontinue anti-thyroid medication. However, hemodynamic volatility and acute inflammation of the thyroid may increase the risk of perioperative complications and mortality. Thus, most physicians choose to defer thyroidectomy to the elective setting in patients that respond to initial medical management. It is unclear whether any patients benefit from thyroidectomy at the same stay as the index admission for thyroid storm.
Outcomes of operative intervention for thyroid storm remain poorly defined in the literature and primarily rely on case reports and limited retrospective studies.5-7 The present study examined perioperative outcomes of thyroidectomy in the management of thyroid storm, as well as factors associated with receiving operative intervention through an analysis of a comprehensive national data set. We hypothesized that thyroidectomy during the initial admission for thyroid storm would be associated with high rates of perioperative complications.
Methods
Study Cohort
The study cohort was derived from the 2016 to 2020 National Inpatient Sample (NIS). The National Inpatient Sample is an administrative database maintained by the Healthcare Cost and Utilization Project (HCUP) of the Agency for Healthcare Research and Quality. It samples 20% of discharges of all inpatient admissions to nonfederal hospitals in states participating in HCUP, generating data from 7 million unweighted and 35 million weighted hospitalizations annually. This study was deemed exempt from full review by the Institutional Review Board of the University of California, Los Angeles. Using the International Classification of Disease, 10th Revision-Clinical Modification (ICD-10-CM) codes, we identified all adult (≥18 years) hospitalizations with a diagnosis of thyrotoxicosis (ICD-10 E05) and thyroid storm (ICD-10 E05.X1).
Study Variables
The incidence of thyroid storm was calculated by dividing the total number of admissions for thyroid storm by the U.S. population estimated in December of each corresponding year, as provided by the U.S. Census Bureau website (National Population by Characteristics: 2010-2019 [census.gov]). Study variables included age, sex, comorbidity burden, race, and insurance status. The Elixhauser Comorbidity Index, which is a composite score of 30 chronic conditions, was utilized as a measurement of comorbidity burden. Predisposing conditions to onset of thyroid storm were identified by ICD-10 codes (Supplemental Table S1) and included Grave’s disease, single toxic nodule, and history of noncompliance. Similarly, the presence of associated conditions was defined using corresponding ICD-10 codes (Supplemental Table S1). Patients who underwent thyroid surgery and parathyroidectomy were identified with ICD-10 procedure codes (Supplemental Table S1). Using NIS’s PRDAY variable, which identifies which hospital day a procedure was performed, an operation was considered to precipitate thyroid storm if it was performed on or before the day of admission. Patients who underwent thyroidectomy after hospital day zero were considered to have undergone therapeutic operation for resolution of thyroid storm. Postoperative neck hematoma was defined as having an ICD-10 diagnosis code of E36.0 or a procedure code of reoperation for open drainage of the thyroid gland or neck (Supplemental Table S1). Hospital costs were calculated using the HCUP cost-to-charge ratio, which converts hospital charges into actual costs of the admission. All costs were standardized to the 2020 Personal Health Care-Hospital Care index to account for inflation.
Statistical Analysis
All statistical analyses were performed using Stata v 16.0 (StataCorp LLC, College Station, TX, USA). Sample sizes reported in the study are national estimates generated with Stata’s (SVY) command, utilizing NIS’s stratified cluster design and hospital’s discharge-level weight. In accordance with HCUP, any sample sizes less than 11 have been reported as <10 to protect patient privacy. Categorical variables were compared using the chi-squared test and continuous variables with the adjusted Wald test. Temporal trends were analyzed with the Wilcoxon rank-sum test. A hierarchical, multivariable regression model of receiving thyroidectomy and mortality included variables such as age, sex, race, insurance status, hospital type, Elixhauser Comorbidity Index, predisposing conditions, and associated conditions. These variables were selected based on optimization of the receiver-operator curve.
Results
During the study period, an estimated 650 974 patients were admitted with thyrotoxicosis, of which 16 175 (2.5%) had a diagnosis of thyroid storm. Hospitalizations for thyroid storm increased from 8.22 to 10.6 per 100 000 admissions. The incidence of thyroid storm among the U.S. population increased from .91 per 100 000 people in 2016 to 1.03 per 100 000 people in 2020 (Figure 1). The overall mortality rate for patients with thyroid storm was 5.3%, with an increasing trend from 2.9% in 2016 to 5.3% in 2020 (P < .001) (Figure 1). Incidence of thyroid storm and associated mortality rate in the United States. The mortality rate trend increased from 2.9% in 2016 to 5.3% in 2020 (P < .001).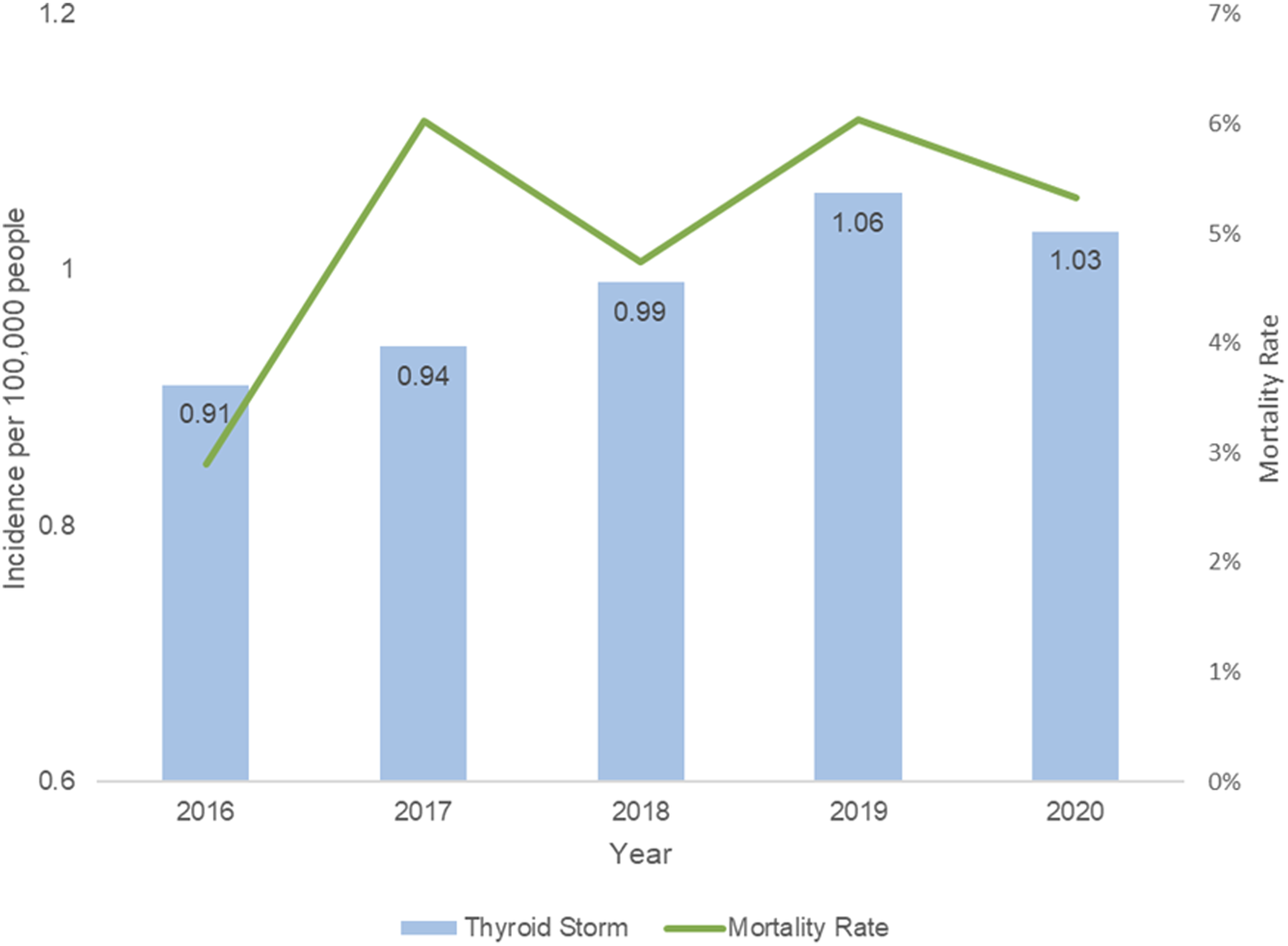
Demographic and Clinical Characteristics of Patients Hospitalized With Thyroid Storm Who Underwent Nonoperative and Operative Management.
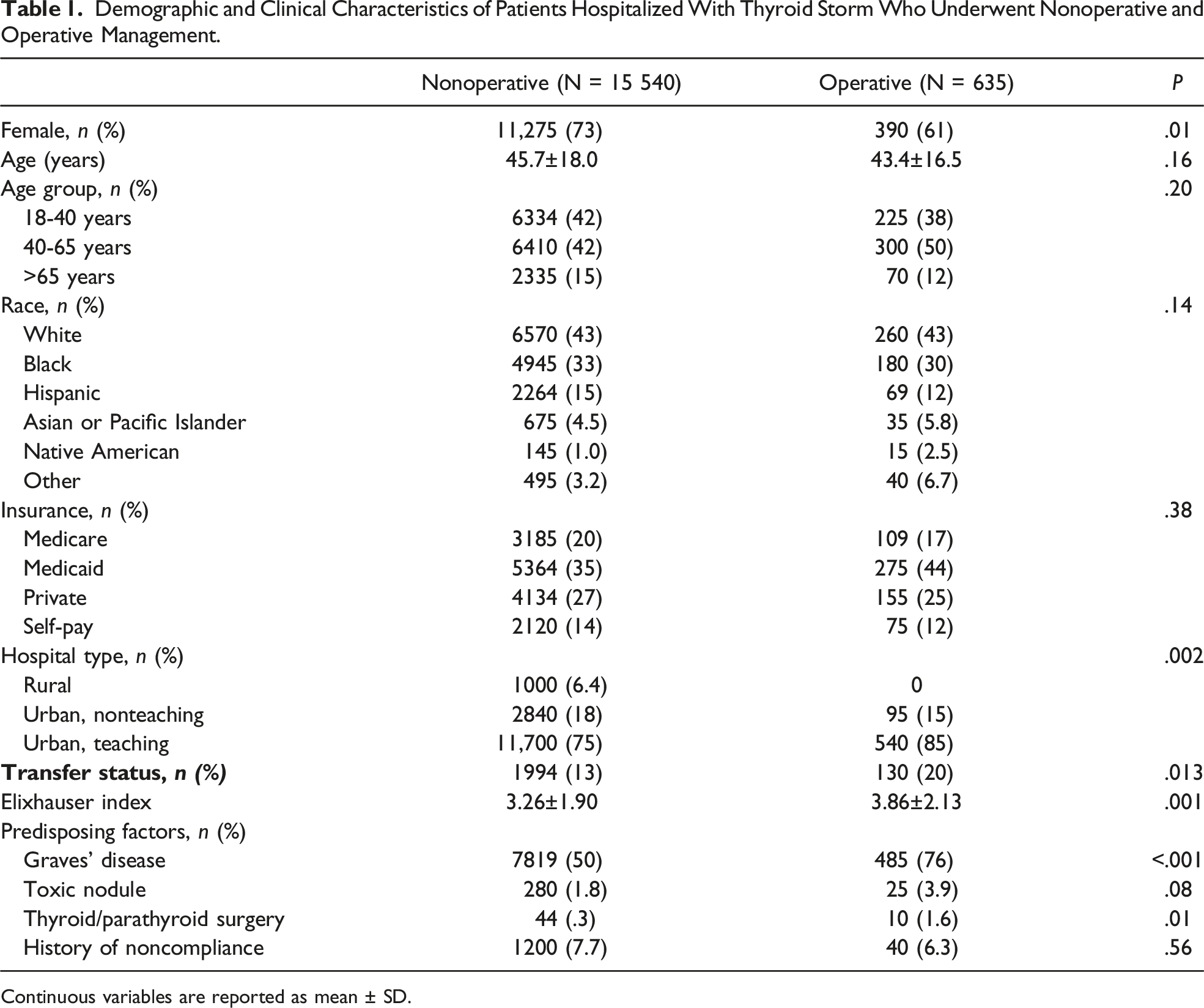
Continuous variables are reported as mean ± SD.
Associated Conditions and Outcomes During Hospitalization for Thyroid Storm.
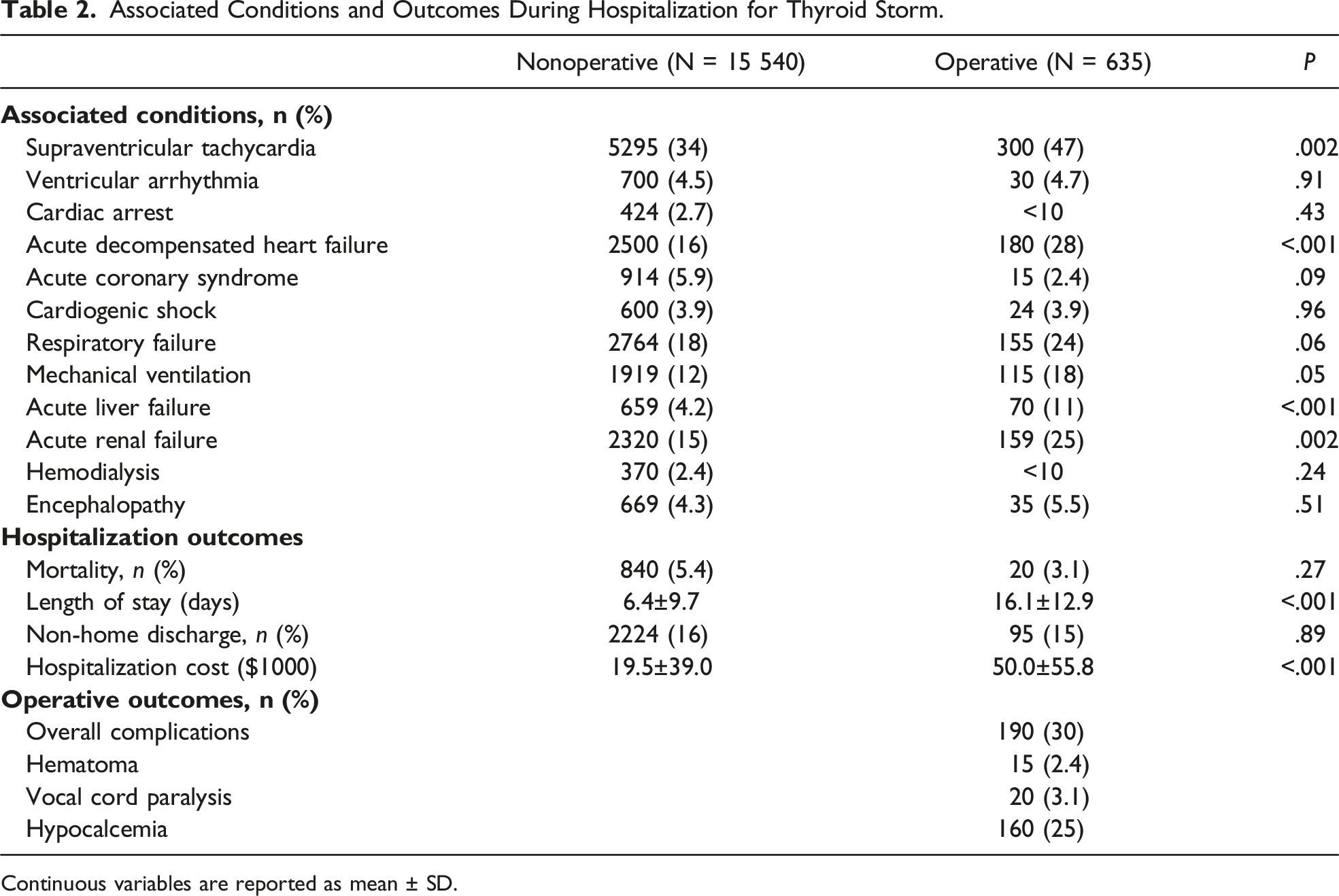
Continuous variables are reported as mean ± SD.
Multivariable Regression of Factors Associated With Receiving Operative Intervention.
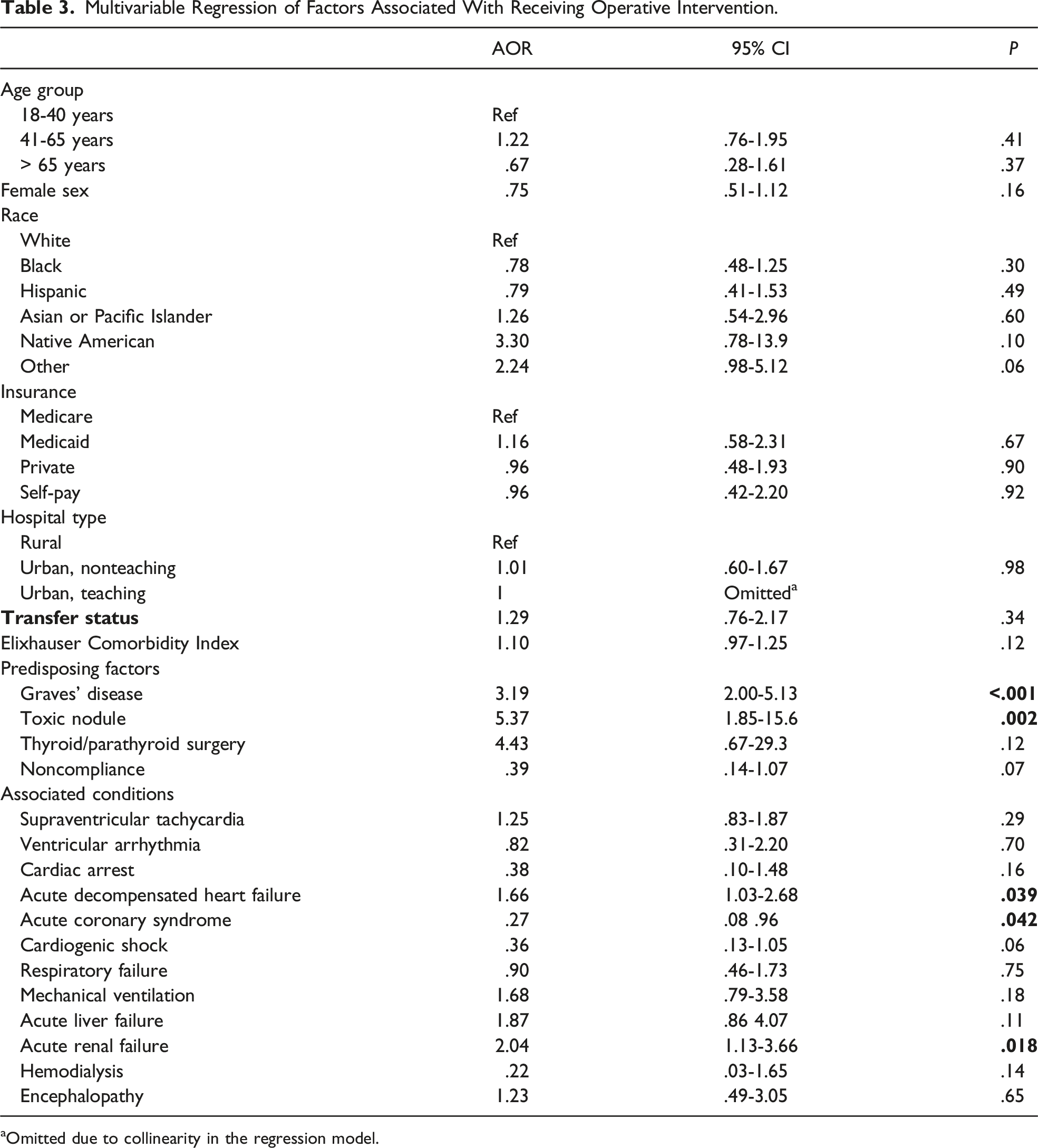
aOmitted due to collinearity in the regression model.
A multivariable regression model was applied to assess factors associated with receiving therapeutic thyroidectomy in patients admitted with thyroid storm (Table 3). In this model, patient demographic or hospital characteristics did not affect the decision for operation. Factors predictive of receiving a thyroidectomy included diagnosis of Graves’ disease (adjusted odds ratio [AOR] 3.16, 95% Confidence Interval [CI] 1.99-4.98, P < .001) or toxic nodule (AOR 4.60, 95% CI 1.59-13.3, P = .005), as well as development of acute decompensated heart failure (AOR 1.62, 95% CI 1.02-2.58, P = .039) and acute renal failure (AOR 2.02, 95% CI 1.15-3.55, P = .014) (Table 3). Those with a history of noncompliance (AOR .36, 95% CI .13-.97, P = .044) and acute coronary syndrome were less likely to receive surgical treatment (AOR .25, 95% CI .07-.87, P = .029). The same model was used to ascertain the effect of surgical treatment on survival, which showed no association between receiving thyroidectomy and mortality (AOR .39, 95% CI .11-1.42, P = .154).
Discussion
In this nationwide study, we showed that operative intervention was not associated with mortality and incurred an overall complication rate of 30%. Additionally, the incidence of thyroid storm hospitalizations has consistently increased from .91 to 1.03 cases per 100 000 admissions over a 5-year period. In a prior NIS survey of thyroid storm from 2004 to 2013, Galindo et al showed an incidence range of .57 to .76 per 100 000 people using similar estimation methods. 8 Since 2013, the cases have continued to increase. This trend may be due to a true increase in incidence or possibly from improved diagnosis and awareness of the disease process. Akamizu et al shared the Japanese experience with thyroid storm with their nationwide database and also showed an increased incidence throughout Japan. 9 The authors believed it to be secondary to improved awareness as noted by increased publications in the literature on the topic. 10
The mortality rate of thyroid storm remains high, with an average of 5.3% and an increasing trend throughout the years. Initial case series reporting on thyroid storm described mortality rates as high as 37%, 11 but more contemporary reviews based on retrospective data report mortality rate to be at 10%.1,9 The abovementioned NIS study from 2004 to 2013 for thyroid storm reported mortality rates ranging from 1.2% to 3.6% per year. 8 Retrospective surveys report most common cause of death in thyroid storm as multiorgan failure, followed by congestive heart failure, respiratory failure, arrhythmia, coagulopathy, gastrointestinal perforation, hypoxic brain syndrome, and sepsis.1,3,9 Unfortunately, the NIS does not detail a patient’s cause of death. However, up to 30% of the thyroid storm population in our study did experience acute decompensated heart failure, respiratory failure, acute renal failure, or acute liver failure.
Management of thyroid storm remains primarily pharmacologic. The 2016 American Thyroid Association Guidelines recommend multimodal therapy with β-blockers, anti-thyroid medication, inorganic iodide, and corticosteroids, as well as cooling, supportive therapy, and admission to the ICU. 4 No official recommendation exists on the operative therapy for management of thyroid storm. The guidelines do mention a few small retrospective studies have described thyroidectomy as a treatment option for patients who do not respond to medical therapy but provide no recommendations on the issue. 4 Scholz et al reported 10 cases of thyroid storm in older adults, average age 70 years (range 54-79), in which thyroidectomy was pursued. 5 All patients had severe cardiorespiratory and renal failure prior to the operation, and all patients survived the operation. Two of their oldest patients died 2-3 weeks postoperatively from myocardial infarction and respiratory failure, respectively. Thus, they conclude that early thyroidectomy should be considered in older, chronically ill patients with thyroid storm, especially if complicated by cardiorespiratory and renal failure, to quickly improve patient conditions in 12-24 hours. 5 Fazendin et al performed a retrospective study of thyroidectomy performed on controlled vs uncontrolled thyrotoxicosis—notably not thyroid storm—and showed equivalent complication rates with a rapid improvement in hyperthyroidism between the two cohorts. Thus, they concluded that thyroidectomy could be safely performed in patients who have not achieved a euthyroid state. 7 In our national analysis, we saw 3.9% of patients admitted for thyroid storm undergo thyroidectomy, without a significant trend in utilization throughout the years. There was no difference in mortality in both univariate and multivariate analyses of operative intervention.
Notably, thyroidectomy in setting of thyroid storm carried an overall complication rate of 30%, with hypocalcemia being most common at 25% and vocal cord paralysis at 3.1%. Currently reported rates of hypocalcemia for total thyroidectomy in the non-emergent setting range from 20% to 30%. 12 Recurrent laryngeal nerve injury, leading to vocal cord paralysis, is a feared complication in thyroid surgery, as bilateral nerve paralysis can lead to airway obstruction requiring tracheostomy. Rates of this complication in the literature range from .3% to 3% of permanent paralysis and 5% to 8% of temporary paresis. 13 It is important to note that even in the emergent setting of thyroid storm, complication rates fall within previously reported outcomes. This may be explained by operating on patients with lower risk factors that are not captured by this database, though patients with heart and renal failure were more likely to receive an operation. Possibly, if more thyroidectomies are performed during the same admission, complication rates overall would increase. While we cannot draw any conclusions on the benefit of thyroidectomy during episodes of thyroid storm, we demonstrate that thyroidectomy can be performed safely in difficult situations. Additional studies are needed to define which patients benefit from early thyroidectomy vs delayed thyroidectomy after discharge.
This study has several important limitations due to its nature as a retrospective study of an administrative database. Diagnosis was all based on ICD coding as the NIS does not have clinical or laboratory data. Thus, we were unable to make diagnostic criteria based on such variables. Additionally, there is no treatment data other than procedure codes. We do not know what medications the patients were prescribed as well as what the response to surgery was. We do not know if the diagnosis of hypocalcemia is permanent or temporary, as we only have data for the single admission. Moreover, we assumed undergoing thyroid surgery on or before day of admission was a precursor to thyroid storm. However, it is possible that therapeutic thyroidectomy for thyroid storm could be performed on day of admission, though we believe the incidence to be rare.
In this nationwide survey, we have shown an increasing incidence of thyroid storm with associated increasing mortality rate. Thyroidectomy during the same admission was pursued in 3.9% of cases, without an effect on risk of mortality on multivariate regression, and an overall operative complication rate of 30%. Patients with acute decompensated heart failure and renal failure were more likely to receive an operative intervention. Further studies are warranted to determine which specific criteria constitute failure of medical therapy and thus which patients benefit from operative intervention for thyroid storm.
Supplemental Material
Supplemental Material - National Trends and Outcomes in the Operative Management of Thyroid Storm
Supplemental Material for National Trends and Outcomes in the Operative Management of Thyroid Storm by Young-Ji Seo, Nikhil Chervu, Peyman Benharash, and James X. Wu in The American Surgeon™
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.