
Abstract
Introduction
There is wide variability in prescribing practices among providers, even for patients undergoing the same operations. Our study aims to analyze the variation in opioid prescription practices using a patient-centered approach to establish more appropriate prescribing guidelines for health care providers.
Methods
We conducted phone surveys 30 days after surgery to assess patient-reported opioid use. Over a two-year collection period, we identified patients that had undergone common outpatient pediatric surgery procedures in our 4-surgeon group. Included in the survey tool was the narcotic prescribed (if any), the amount used, and patient/family rating of pain control.
Results
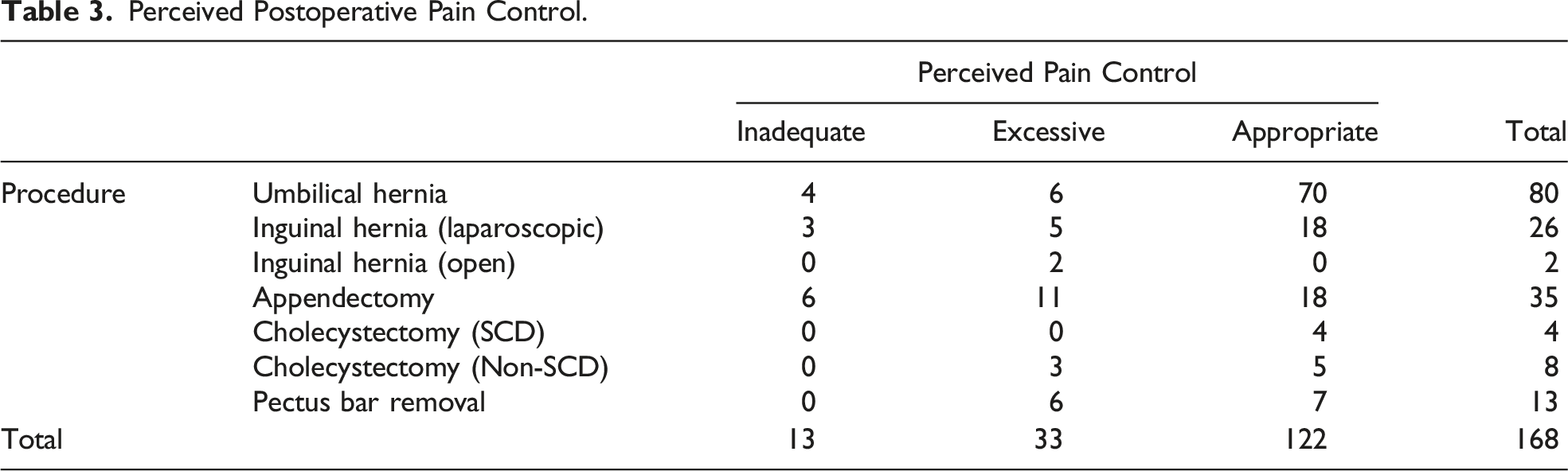
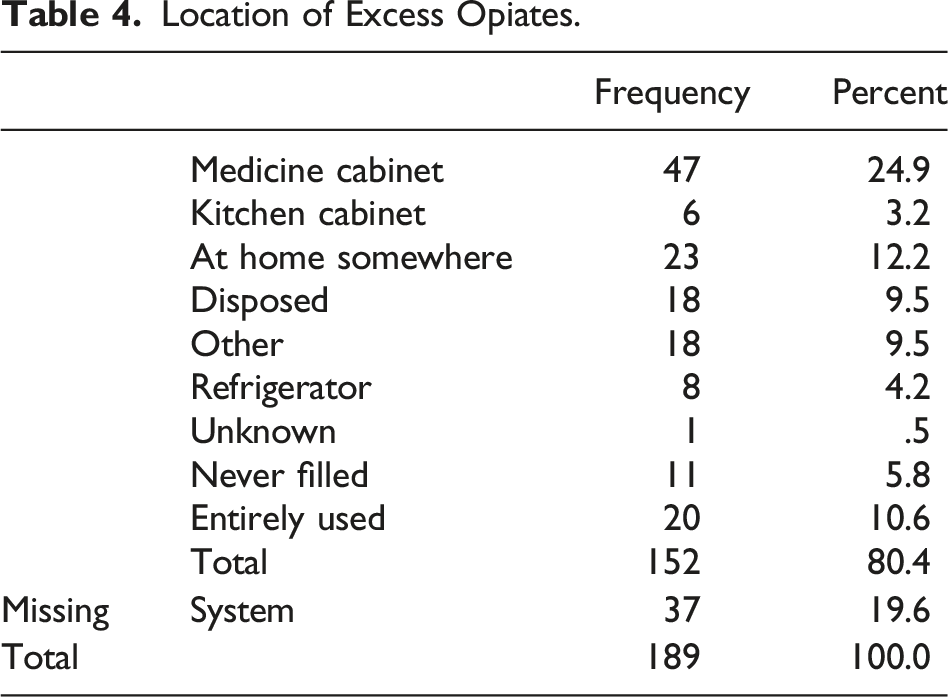
We collected data for 189 separate procedures (88 umbilical hernias, 30 laparoscopic inguinal hernias, 2 open inguinal hernias, 41 appendectomies, 15 laparoscopic cholecystectomies, and 13 pectus bar removals). Patient age ranged from less than 1 month to 246 months. 83.5% of patients had a narcotic prescribed. The average number of doses used was 4, ranging from 0 (11.3%) to 30 (1.5%). 72.6% of families surveyed felt pain control was appropriate. However, 19.6% did feel they received too much pain medication. 10.6% reported completing their entire prescription; however, only 13.6% of families with excess narcotics reported proper disposal.
Conclusions
Despite heightened awareness of the opioid epidemic, there is still a poor understanding of appropriate pain control regimens in the pediatric surgical population. We demonstrate that most patients are discharged home with excess opioids and that many families save the leftover pills/liquid. Further research and education are encouraged to limit the use of opioids in standard pediatric surgical procedures.
Introduction
The past 5 years have witnessed an increasing awareness of the insidious effects of opioids1,2 within the surgical community. This awareness has increased by multiple studies demonstrating the harmful effects of opioids across all segments of society. Unfortunately, and despite their age and resilience, children are not immune to the effects of the opioid epidemic.
Between 1999 and 2018, nearly 9000 children and adolescents died from opioid poisoning, with yearly mortality tripling during this period. 4 Opioid prescription rates, while slowly decreasing, continue to be prevalent among children and adolescents. In 2018, one in 10 girls and one in 12 boys had at least 1 prescription filled for an opioid within the previous year. 3 While many children have been exposed to the availability of opioids in their homes or social environments, more may become addicted through the prescribing practices of physicians and surgeons. This population, and especially the adolescent age group among them, are particularly susceptible to opioid addiction and the resultant sequelae, which result in hospitalizations and death.3,5,6
As surgeons, we prescribe 5% of all opioid prescriptions and often serve as the first “touch point” for infants, children, and adolescents with prescription opioids. 7 Unfortunately, despite increasing efforts to curb prescription and educate surgeons and their patients, data suggest that approximately 5% of opioid naïve pediatric patients develop new persistent opioid use following common surgical procedures. 8
Our group has previously reported that the prescription of opioids at a tertiary care children’s health system can be inconsistent between providers and is often excessive. 9 Follow-up studies demonstrated that low-fidelity educational interventions effectively decreased the doses prescribed following common pediatric surgical procedures in our health system and others.10,11 Despite these successes, the effects of opioid-restrictive policies have yet to be evaluated regarding patient pain control and parental satisfaction. While our first 2 studies targeted identifying the problem and a potential solution at the provider level, the aims of this third study are patient centered. In this study, our primary aims are to evaluate (1) parent-reported opioid consumption, (2) parental assessment of postoperative pain control in the era of decreased opioid prescription, and (3) evaluate how the opioids are disposed following 5 common outpatient pediatric general surgical procedures. With this information, we hope to define further reasonable, patient-centered, procedure-specific prescribing practices and identify ways to empower parents as we confront this public health crisis.
Methods
This study was determined to be exempt from review by the Institutional Review Board at the Medical University of South Carolina due to its inception as a quality improvement project. Over the collection period, we identified patients that had undergone common outpatient pediatric surgery procedures with any of the surgeons in our 4-surgeon group: umbilical hernia repair, inguinal hernia repair (laparoscopic and open), laparoscopic cholecystectomy, laparoscopic appendectomy, and pectus bar removal. In addition, patients undergoing selected surgical procedures were all included for analysis, with no other inclusion or exclusion criteria.
Survey Tool.
Results
Pediatric Surgery Cases Performed and Opioids Prescribed.
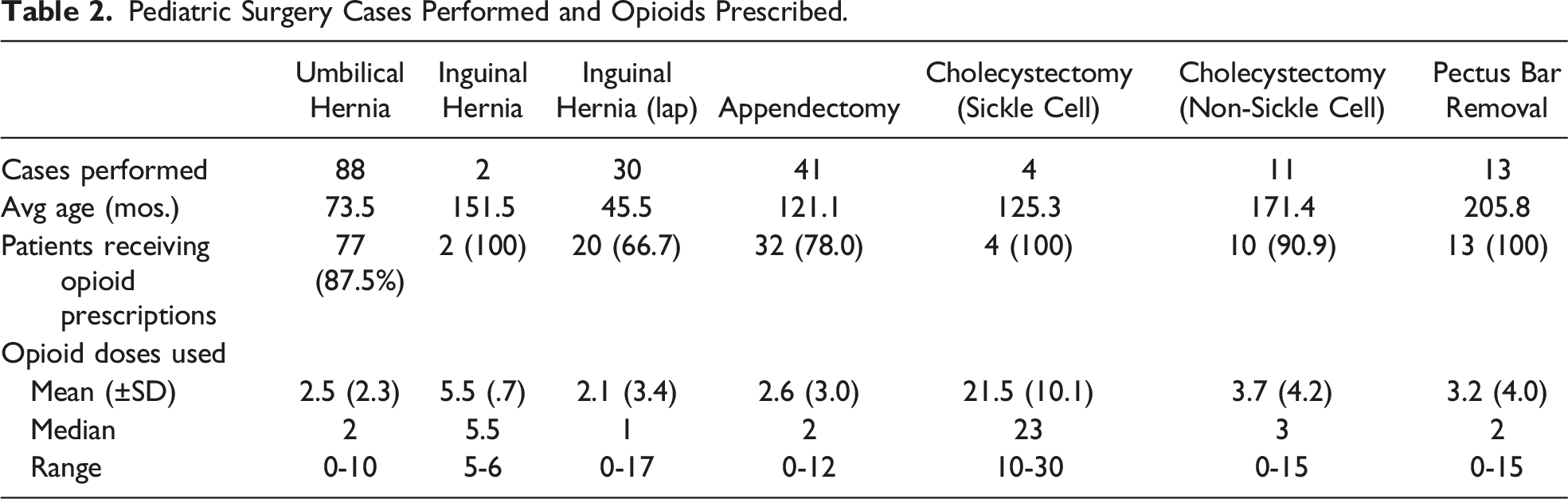
Overall, a high proportion of patients received opioid prescriptions (83.5%). Most patients were prescribed hydrocodone/acetaminophen at the time of discharge (46.6%), followed by oxycodone (35.4%), and Tylenol with codeine (1.1%). Some variability existed in procedure-based prescribing practices, but 100% of patients did receive opioids after open inguinal hernia repairs, laparoscopic cholecystectomies in sickle cell (SCD) patients, and pectus bar removals (Figure 1). For each procedure, the median morphine milligram equivalents prescribed per kilogram of weight (MME/kg) were umbilical hernia (.70), laparoscopic inguinal hernia (.59), open inguinal hernia (1.5), appendectomy (.70), cholecystectomy (SCD) (2.9), cholecystectomy (non-SCD) (.88), and pectus bar removal (1.5). Opioid doses prescribed postoperatively by procedure type. For each procedure studied, the x-axis is represented by the number of doses prescribed in morphine milligram equivalents to the patient postoperatively, adjusted for body weight. The y-axis represents the number of patients reporting each value.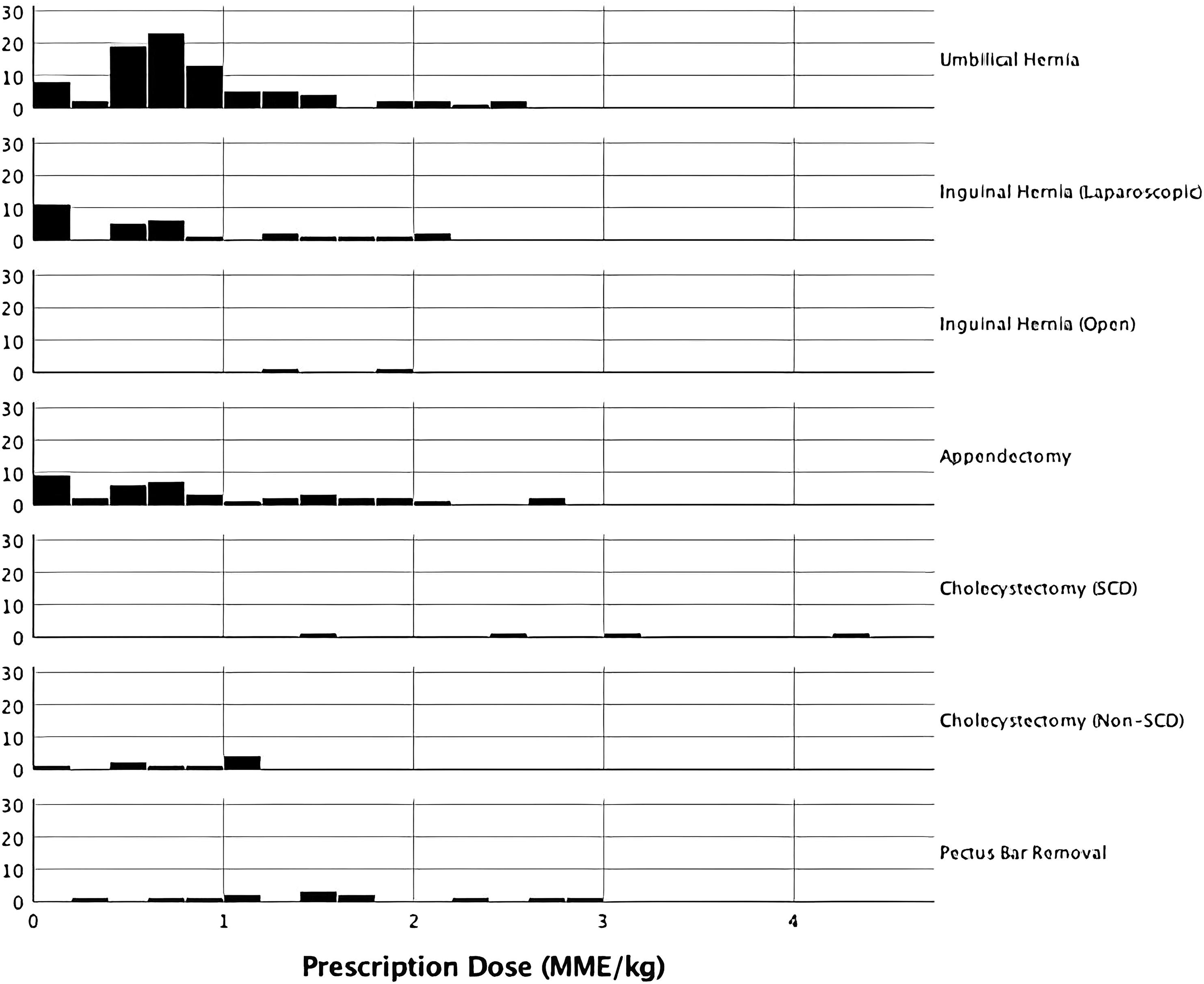
Similarly, the number of opioids used postoperatively varied drastically by procedure type. The average number of doses used was 3, with a range of 0 doses (27%) to 30 doses (1.1%) (Table 2). As Figure 2 demonstrates, most patients required relatively little of their respectively prescribed opioids. Indeed, except for the sickle cell patients that underwent laparoscopic cholecystectomy, most patients had a minimal requirement for the narcotic they were prescribed. For each procedure, the median MME/kg utilized by patients were umbilical hernia (.30), laparoscopic inguinal hernia (.10), open inguinal hernia (.53), appendectomy (.20), cholecystectomy (SCD) (2.1), cholecystectomy (non-SCD) (.25), and pectus bar removal (.23). Opioid doses taken postoperatively, by procedure type. For each procedure studied, the x-axis is represented by the number of doses (in morphine milligram equivalents, adjusted for weight in kg) used of the respective opioid prescribed to the patient postoperatively. The y-axis represents the number of patients reporting each value.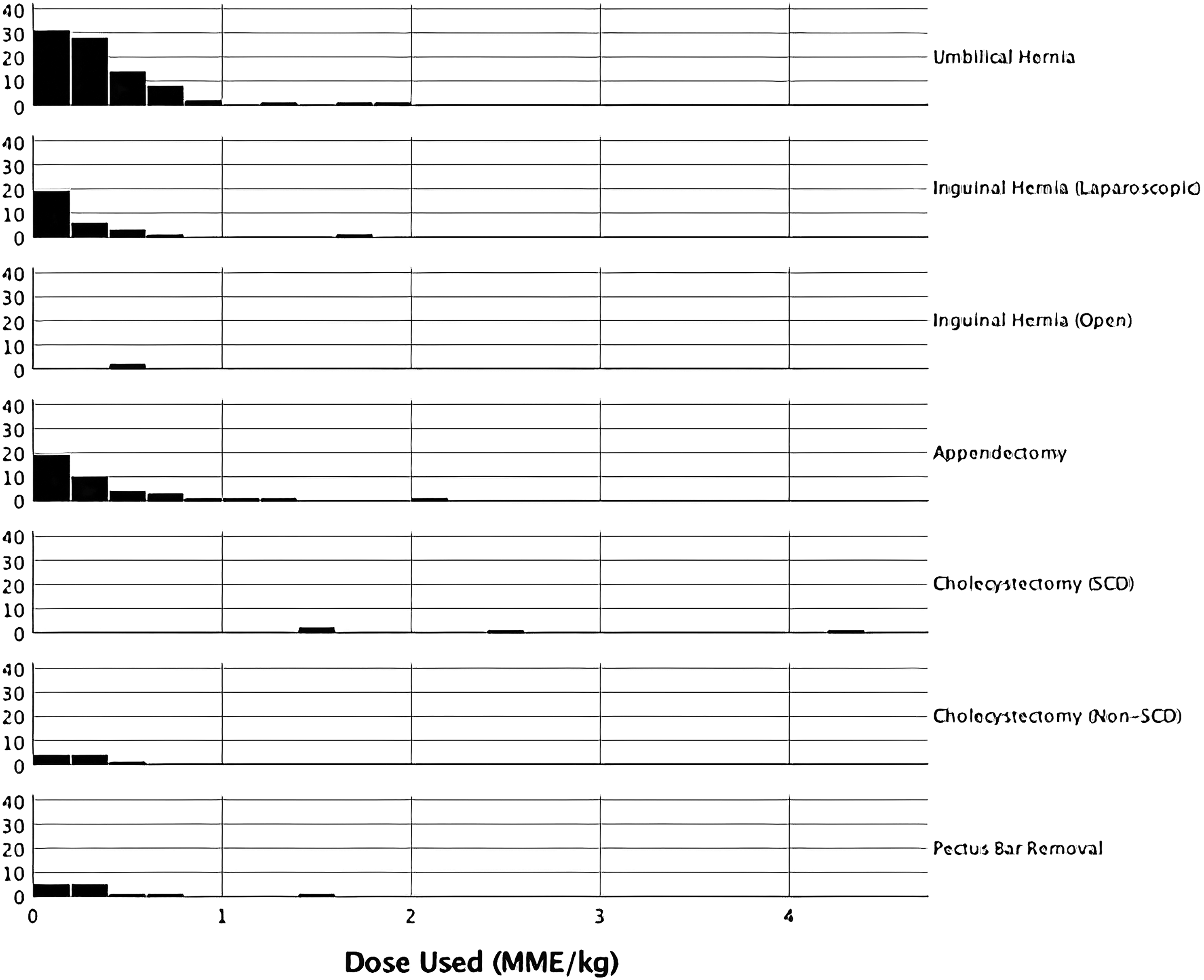
Perceived Postoperative Pain Control.
Location of Excess Opiates.
Discussion
Awareness of the current opioid epidemic is at an all-time high. Over the last several years, many in the surgical community have taken steps toward addressing our role in the crisis. In our department, the publication by Hill et al has anecdotally had a significant impact on our prescription practices after outpatient procedures. 1 The pediatric surgery division has been no exception to this change. Moreover, the awareness of opioid overprescription among residents and attendings alike has impacted our views and practices. The caveat is that experiences with adult surgical procedures have largely informed the shift. As such, our goal has been to assess the current state of opioid prescription practices in our pediatric surgery group and to define guidelines to which our prescribers may refer more clearly.
The findings of our study demonstrated several patterns regarding our management of outpatient procedures. First, for every procedure studied, there was a trend toward overprescription. For the most common procedures (umbilical hernias, laparoscopic inguinal hernias, and appendectomies), a plurality of patients used .25 or fewer MME/kg. It is important to note that the low opioid use we have documented here comes with increased awareness of the opioid epidemic. We can then infer that the opioid prescription practices were already affected by this fact, and despite this, we still saw very little intake of opioids vs the amount prescribed. As with our previous studies, this suggests a role for multimodal therapy (narcotic and non-narcotic) and that better education (for prescribers and parents) could potentially obviate the need for opioids for these patients.
We also found several procedures for which large amounts of opiates continued to be prescribed. In addition to pectus bar removals mentioned above, open inguinal hernia repairs and laparoscopic cholecystectomies in patients with SCD were all associated with large postoperative MME prescriptions. One assumes that this pattern reflects the pre-conceived expectation that these patients will have more pain after these procedures and/or require more narcotic analgesia. However, the number of patients in these groups was relatively low, making the data somewhat difficult to interpret. Regardless, it is worth noting that even in these groups, prescribed MME/kg drastically overestimated actual need.
The issue of overprescription raises the importance of improving provider education. Recent literature and expert panels from multiple institutions have shown that opioid prescriptions are unnecessary for most common pediatric surgical procedures.12,13 The Opioid Prescribing Engagement Network (OPEN) recommends avoiding opioids for appendectomy, inguinal hernia, and umbilical hernia, which aligns with the procedures in our study. 12 Additionally, evidence suggests that procedures such as pectus bar removal and laparoscopic procedures can be performed without opioids. 13
In addition to the prescription of opioids, it is crucial to consider the type of opioid used. As mentioned earlier, whenever possible, a multimodal approach using opioid-free and balanced analgesia should be attempted to mitigate the adverse effects associated with opioid overuse. 13 Some alternative forms of analgesia include the use of acetaminophen, NSAIDs (ibuprofen/ketorolac) in oral, rectal, and intravenous forms, as well as neuraxial blocks when feasible and appropriate for the procedure. Furthermore, it is important to note that 1.1% of patients were prescribed codeine, which now carries a black box warning from the FDA due to the risk of respiratory depression, particularly in rapid metabolizers. 14
Salient to the opioid discussion, as it pertains to children, is the question of excess narcotic disposal. It has been well documented that narcotic addiction often begins and/or is fueled by unused, excess medication stored long-term within the household. Further exploration of this phenomenon within the dynamic of a family where the adults of the household could be artificially influencing our perception of opioid usage was required.
Interestingly, we found that many families were not disposing of excess opioids. Only 9.5% of the responders indicated disposal. In addition to the 35% that either never filled their prescription, completed it, or provided no response, almost 55% of our patients have unused opiates somewhere in their homes. This information, coupled with the fact that most families felt they were given adequate or excessive amounts of opioids, makes one question why so many still saved the surplus. Whether these were forgotten or being saved for future use, this represents an area for improvement in care, potentially through return programs, perhaps at follow-up clinic appointments. Current recommendations promote providing caregivers secure storage as well as providing an infrastructure and means for safe opioid disposal.
Proper disposal of unused opioids is critical to prevent misuse, abuse, and environmental contamination. The U.S. Food and Drug Administration (FDA) provides guidelines for the safe disposal of medicines, including opioids. According to the FDA, flushing opioids down the toilet or throwing them in the trash can pose potential risks. However, the FDA has identified a small number of medications, including certain opioids, that should be flushed down the toilet when no alternative disposal methods are available. This list, known as the FDA’s flush list, aims to address the immediate risk of harm from accidental ingestion or misuse of these specific medications. For opioids not included in the flush list, it is recommended to follow specific guidelines provided by authorized collection sites, take-back programs, or participating pharmacies. By following these disposal practices, individuals can contribute to reducing the availability of opioids, protect both themselves and the environment, and ensure proper medication management. 15
Multiple factors limit this study. First, while it is prospectively collected data, the survey tool leans heavily on the participation of patients’ families and their recall of the immediate postoperative period. Given that some pediatric patients cannot speak for themselves, actual pain control cannot be truly determined with certainty. We are also limited here by the single center studied here. Our medical center sees pediatric patients from a moderately large catchment area. Still, our patients are mostly rural/suburban and underinsured, although there is some urban presence in our patient population. Lastly, there has been very little standardization of opioid prescriptions across our practice, and the prescription patterns were largely attending/resident dependent. This fact was, of course, also part of the impetus to undertake our study.
In conclusion, our findings align with adult data on opioid prescription patterns, highlighting the excessive administration of narcotic medications to pediatric patients following various outpatient surgeries. It is evident that most patients do not require more than minimal doses for adequate pain relief. Over the past few years, despite evolving prescription practices and insights from our previous studies, we have continued to overestimate pain requirements, resulting in the unnecessary overprescription of opioids. Except for sickle cell patients who require intensive opioid studies, we are approaching a time where opioid prescriptions may become obsolete through the diligent implementation of multimodal pain treatment and effective management of patient expectations. Furthermore, it is crucial to emphasize the importance of education on securing and safely disposing of opioids at the time of prescription, ensuring responsible medication management practices.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.