
Abstract
Eosinophilic myenteric ganglionitis (EMG) is a rare pathologic finding within the Auerbach myenteric plexus characterized by eosinophilic infiltration on light microscopy. The plexus’s ultimate obliteration results in chronic intestinal pseudo-obstruction (CIPO). EMG is almost exclusively seen in the pediatric population. The diagnosis of EMG is made through full-thickness rectal biopsy and EMG is not detectable through routine screening measures such as imaging or colonoscopy. The current treatment modality for this disorder is not standardized, and has often been treated with systemic steroids given its eosinophilic involvement. This case presents a 73-year-old male with chronic constipation presenting with new obstipation in the setting of recent orthopedic intervention requiring outpatient opioids. Admission radiographs were consistent with sigmoid volvulus. Following endoscopic detorsion, exploratory laparotomy revealed diffuse colonic dilation and distal ischemia requiring a Hartmann’s procedure. Surgical pathology revealed EMG, increasing the complexity of subsequent surgical decision-making after his urgent operation.
Introduction
Eosinophilic myenteric ganglionitis (EMG) is a rare cause of bowel dysmotility most commonly seen in pediatric patients. 1 Its key diagnostic feature is the infiltration of eosinophils through the Auerbach myenteric plexus, only visible through full-thickness biopsy sample. Ultimately, this infiltration is thought to result in complete destruction of the plexus. As EMG manifests as dysmotility and constipation and there is no readily available screening examination or imaging; it remains a rarely detected disease. While a universal standard of care has yet to be established, current literature reports cases of EMG responsive to systemic steroids.1,2 Positive response to steroids has been reported in pediatric patients, without much exploration in adult populations due to rarity.
Case Presentation
We present a case of a 72-year-old man who presented to the emergency department (ED) with acute worsening of chronic abdominal pain, abdominal distension, and constipation as well as new-onset obstipation. For the last 10 years, he was reliant upon both oral and rectal agents for a daily bowel regimen. He had never had a colonoscopy, Sitzmark study, or other evaluation given lack of access to care. On questioning in the ED, he noted recent labrum repair requiring the use of outpatient narcotics that seemingly coincided with his worsening symptoms.
On arrival to the ED, he was hemodynamically stable. On exam, he had a distended though compressible abdomen with mild tenderness in the left lower quadrant. He had no evidence of peritonitis. Laboratory evaluation revealed a lactic acidosis that resolved with fluid resuscitation.
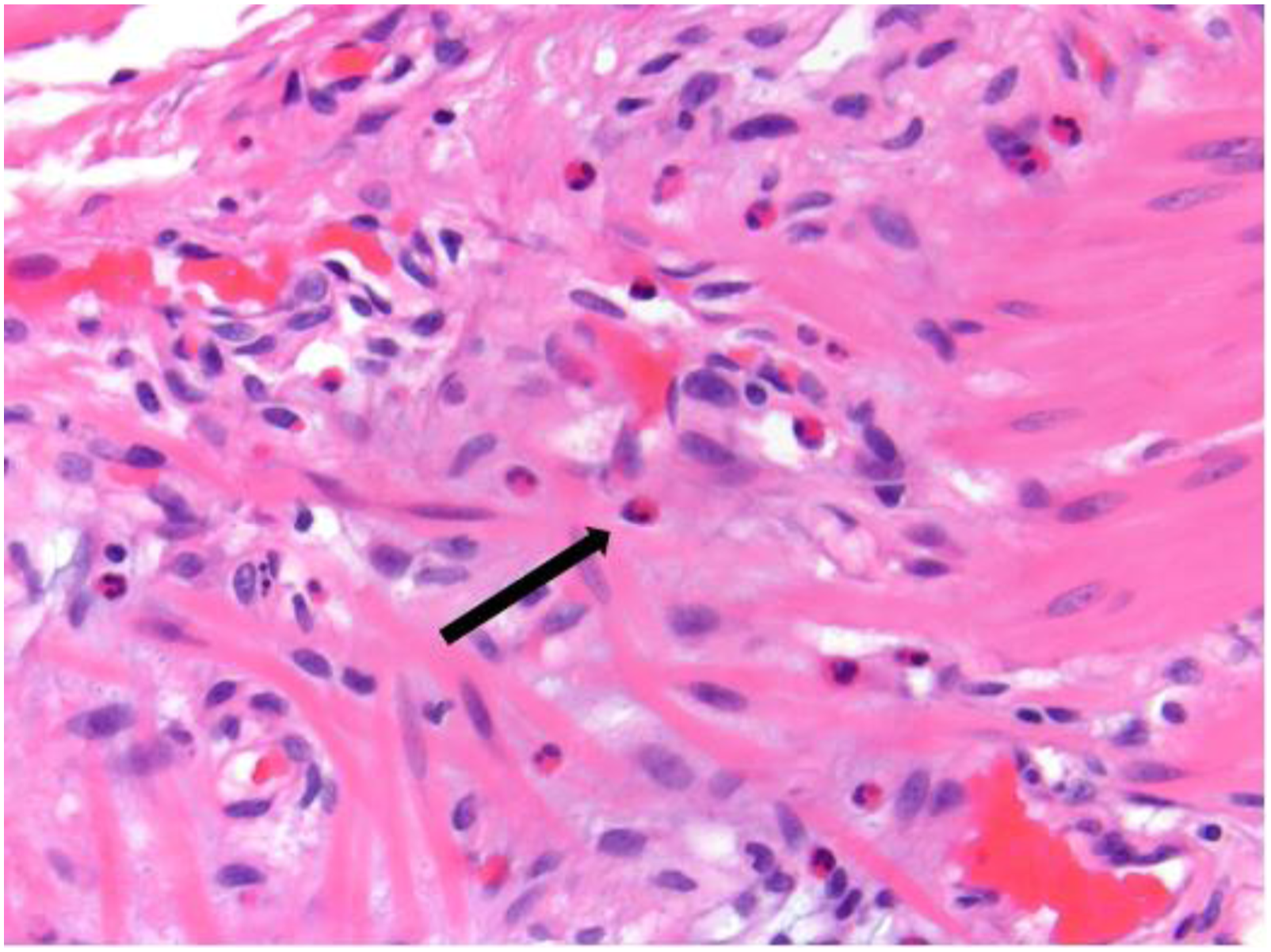
Abdominal x-ray demonstrated sigmoid volvulus (Image 1) and he promptly underwent successful endoscopic detorsion. Given findings of sigmoid mucosal ischemia on flexible sigmoidoscopy and worsening abdominal pain post-procedurally, he proceeded to exploratory laparotomy. Upon gross inspection, the colon was vastly dilated and edematous, most notably in the sigmoid and descending colon, with transmural sigmoid ischemia. Given these findings, a Hartmann’s procedure with end transverse colostomy was performed. His rectal stump was drained with a rectal tube. His postoperative course was complicated by a prolonged ileus demonstrated on cross sectional imaging for which he was discharged on total parenteral nutrition on postoperative day 15. Following discharge, his surgical pathology revealed EMG (Image 2). Within the next month, the patient gradually advanced to a regular oral diet with return of bowel function via his end colostomy. In postoperative follow-up, the patient’s preference was to keep the colostomy as he found his current bowel function markedly improved from his preoperative baseline and also desired to avoid any further surgery. Abdominal X-ray imaging of sigmoid volvulus. Eosinophilic infiltration of the muscularis propria and myenteric plexus, 400x. Arrow indicates eosinophil.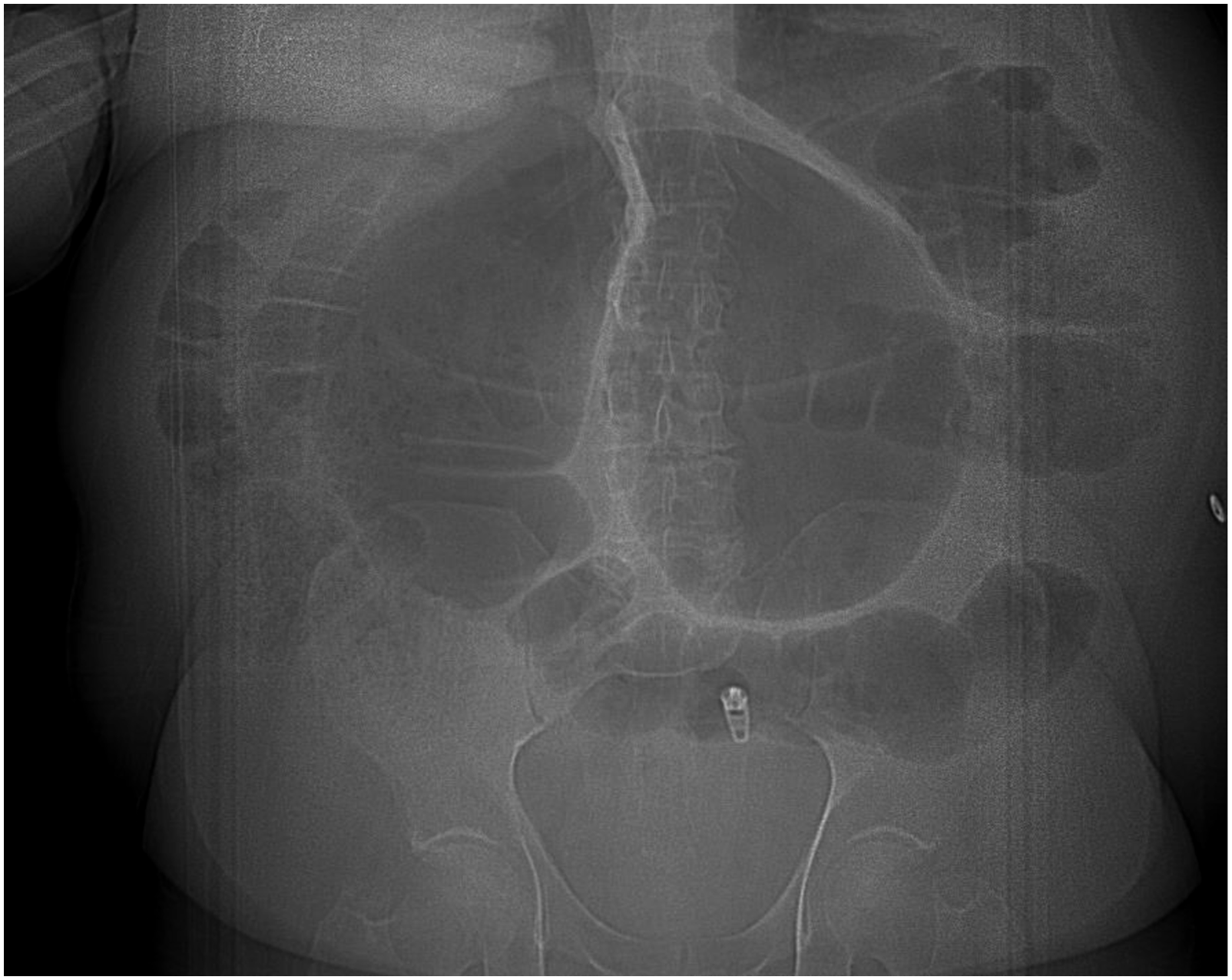
Discussion
EMG is a rare disorder characterized by impaired colonic propulsion and eosinophilic inflammation of the myenteric ganglia. The precise etiology of EMG is not clearly understood. The disease is predominantly reported in the pediatric population, with age of onset ranging from as early as infancy up to 15 years. 3 Its exact prevalence in the general population remains undefined due to the rarity of the disease state; however, various case reports have indicated success with systemic steroid treatment and biologic agents. 1 Previous reports have found an increase CD 4+ cells in the setting of EMG, leading to the possible conclusion that the disease process originated from a systemic immune reaction which later progressed into a chronic inflammatory state. 4 The eosinophilic involvement of the disease may largely represent its inflammatory nature, thus possibly lending itself to the responsiveness of biologics and steroids. There is no formal pathologic grading system to quantify eosinophilic involvement at this time.
In this patient’s case, screening colonoscopy prior to acute presentation would not have diagnosed his underlying pathology, but functional studies such as Sitzmark transit test could have provided further insight into the severity of his dysmotility. His recent narcotic medication use for postsurgical pain management following labrum repair likely was an acute insult on a chronic condition precipitating the sigmoid volvulus. In retrospect, his prolonged return of bowel function was likely related to his baseline dysmotility given the absence of any signs of obstruction on cross sectional imaging. Taking his prolonged ileus and new pathologic findings into account, had the patient been desirous of colostomy reversal, formal assessment of his motility might improve patient counseling and led to a balanced discussion regarding ostomy reversal and consideration of coloproctostomy vs ileorectal reconstruction.
Sigmoid volvulus is typically a sporadic event in otherwise healthy colon. However, in some cases, it can be a manifestation of rare dysmotility disorders such as EMG. While rare disorders of dysmotility are unlikely to be suspected in the acute setting, the knowledge of their presence postoperatively should influence ongoing surgical planning.
Footnotes
Author Contributions
JLR and NMS provided inpatient care. All authors reviewed the case and pathology. AK led manuscript composition. All authors reviewed the manuscript and provided edits.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was not specifically funded; however, LHM is supported by National Institute of Diabetes and Digestive and Kidney Diseases-1K08DK124687 and the Measey Foundation.