
Abstract
An aberrant right hepatic duct is a rare congenital anomaly of the biliary system. Failure to recognize these anomalies can result in serious complications. In this case, we present a patient who underwent laparoscopic cholecystectomy for chronic cholecystitis. Post-operatively she developed a bile leak for which she underwent reoperation. On re-exploration, she was discovered to have a cystic stump leak and a rare Hisatsugu type V anatomic anomaly of the right hepatic duct originating from the cystic duct. She was subsequently managed with oversewing of the cystic duct stump and drainage. This case demonstrates the importance of recognizing these rare anomalies and the challenges of management in a rural, resource-limited setting.
Congenital anomalies of the biliary tract are relatively common with a reported incidence between 15% and 24%.
1
However, of these anomalies, aberrant right hepatic duct (ARHD) draining into the cystic duct (Hisatsugu type V anomaly) continues to be a rare phenomenon, with an overall incidence of around .4%
2
(Figure 1). In this report, we present a case of an aberrant right hepatic duct identified post-operatively, resulting in a bile leak. Various types of aberrant right hepatic ducts as described by Hisatsugu et al redrawn and adopted from image as seen in Kurahashi et al.
2
GB = gallbladder; ARHD = aberrant right hepatic duct.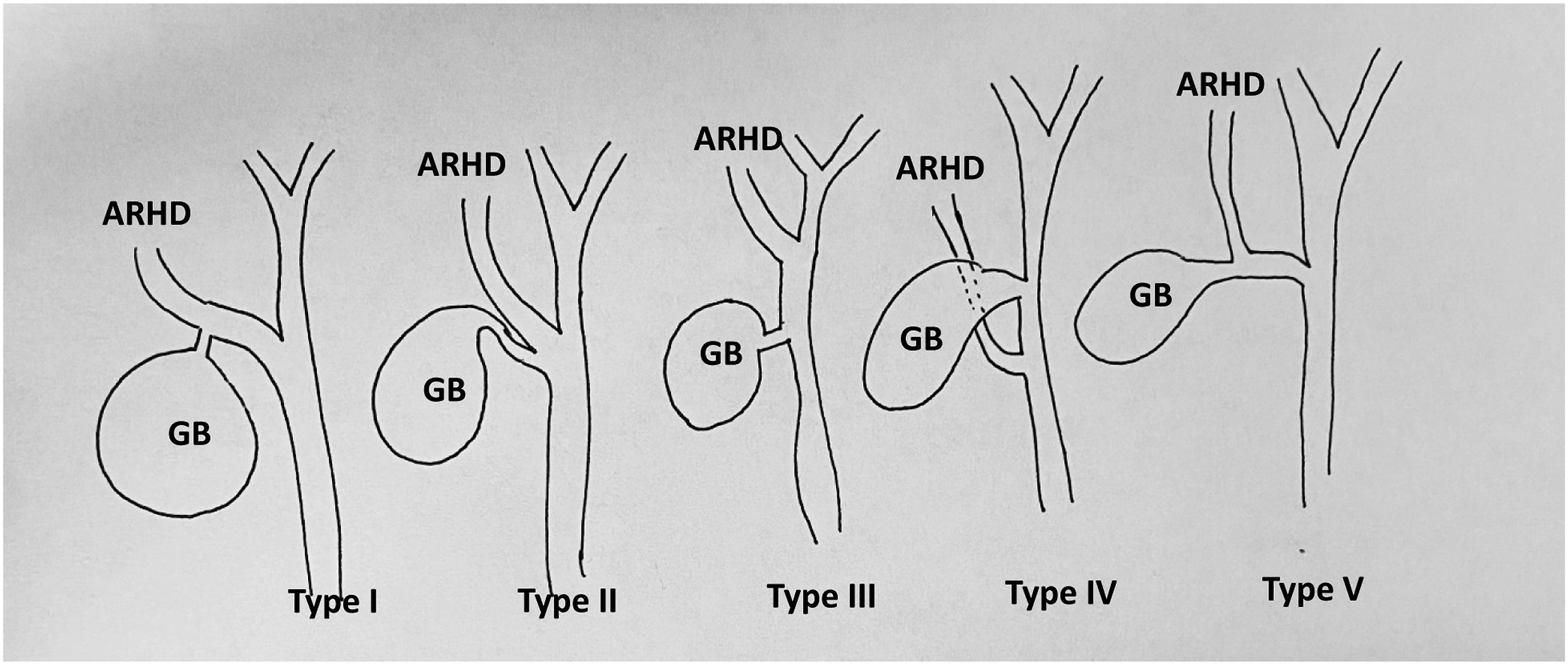
The patient is a 76-year-old female who presented to a rural medical center with months of post prandial right upper quadrant pain not relieved by anti-reflux medications. Outpatient evaluation with right upper quadrant ultrasound showed cholelithiasis with impacted stones. Liver function tests at that time were within normal ranges. She was taken to the operating room for laparoscopic cholecystectomy. The abdomen was entered using a Hasson technique and pneumoperitoneum was established. General sweep of the abdomen showed a chronically inflamed gallbladder with multiple omental adhesions. After omental adhesions were taken down, it was noted that a large, impacted stone had begun to erode through the gallbladder wall at the insertion of the cystic duct. During mobilization to achieve the critical view of safety, the cystic duct detached from the gallbladder at this site of the eroding stone, precluding intraoperative cholangiogram. The cystic artery was identified and clipped, the gallbladder was removed from the gallbladder fossa in the traditional retrograde fashion, and the cystic duct stump was closed with a polydioxanone (PDS) suture, surgical clip, and an Endoloop (Ethicon Endosurgery, Somerville, NJ). As an alternative to an intraoperative cholangiogram, to confirm anatomy, 2.5 mg of indocyanine green was given, and the common bile duct was identified to be medial to the cystic duct stump. The area was inspected and given the traumatic detachment of the cystic duct from the gallbladder wall; a 15 Fr. surgical drain was placed. The patient was closed and taken to recovery.
On post-operative day 2, the patient was noted to have bilious drainage from her surgical drain. The patient was offered transfer to another facility for endoscopic retrograde cholangiopancreatography (ERCP); however, she refused. An exploratory laparotomy was performed, and the patient was found to have a bile leak emanating from the cystic duct stump. At this time, a cholangiogram was successfully performed and showed an ARHD inserting into the cystic duct. The cystic duct then joined with the left hepatic duct to form the common bile duct which drained normally into the duodenum (Figure 2). No hepatic or common bile duct injuries were identified. The cystic duct stump was reinforced with PDS suture, a drain was again left in place, and the patient was taken to the recovery room. On post-operative day 4, the patient was discharged with her surgical drain. Follow-up magnetic resonance cholangiopancreatography (MRCP) reconfirmed the right hepatic duct anomaly and did not demonstrate a right hepatic duct injury (Figure 2). On post-operative day 8, the drain was no longer bilious and was removed in clinic. The patient was seen 3 months later and has fully recovered. She had normal liver function tests and complete resolution of her biliary colic symptoms. (A) Intraoperative cholangiogram during reoperation demonstrates a cystic stump leak and type V aberrant right hepatic duct. (B) Post-operative MRCP similarly shows aberrant right hepatic duct anatomy. (C) Representative image of type V ARHD anatomy in this case. ARHD = aberrant right hepatic duct; CBD = common bile duct; CD = cystic duct; LHD = left hepatic duct; GB = gallbladder.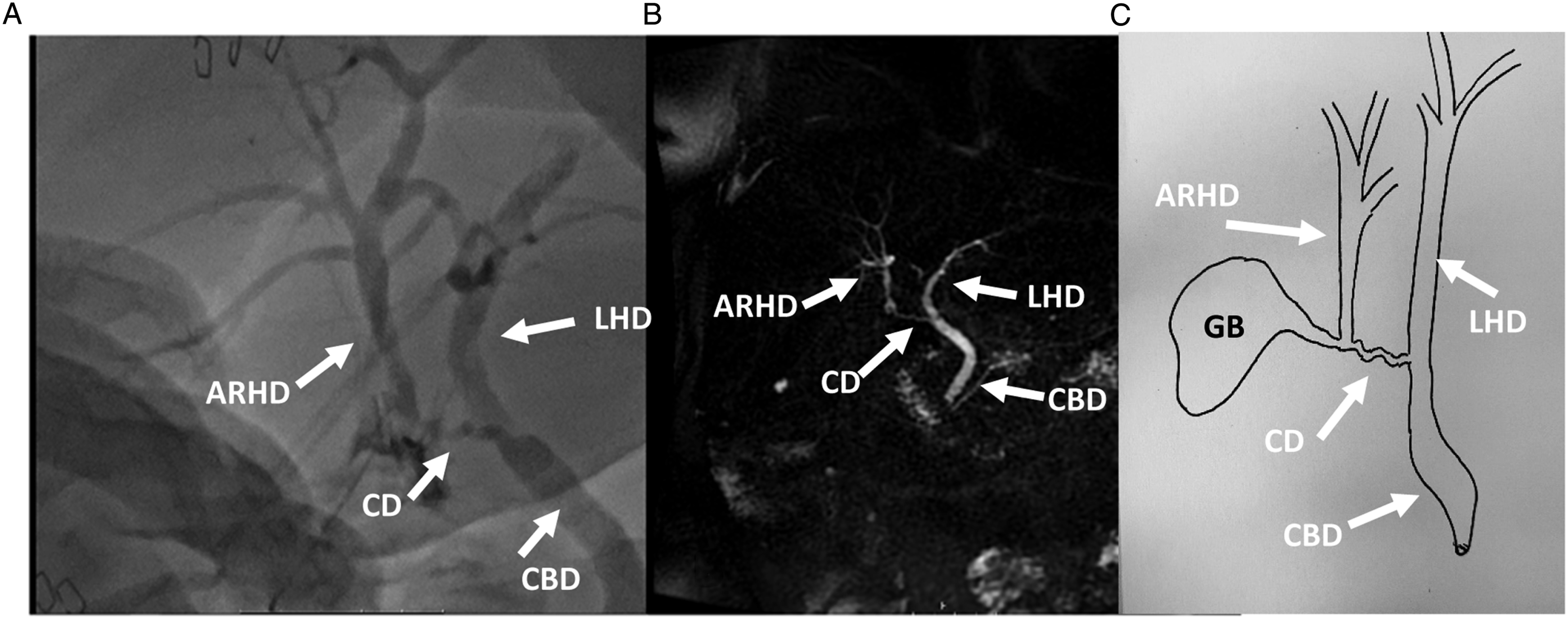
Aberrant right hepatic duct anatomy continues to be a rare yet clinically important biliary anomaly with its presence accounting for an increased risk in bile duct injury.1-3 In this case, a rare type V ARHD anomaly was observed post-operatively after the development of a bile leak. It is our belief that the cystic stump leak developed partly due to back pressure given the short proximity between the cystic duct stump and inflow from the ARHD. In this case, continued management with surgical drain for an additional 8 days was sufficient to allow closure of the cystic duct stump.
All rural surgeons should be aware of these rare but important anomalies of the biliary tree, particularly if their practice areas are limited in advanced endoscopy and availability of advanced imaging. While preoperative diagnosis of biliary duct anomalies is preferred, these anomalies are often encountered at the time of operation or post-operatively. 4 Planning for potential anomalies; establishment of transfer protocols to referral centers if complications occur; strict adherence to maintaining the critical view of safety; and use of intraoperative imaging are all important practices to ensuring a safe and technically successful cholecystectomy in the rural setting. In this case, the use of indocyanine green during the initial operation was a helpful alternative to determine biliary anatomy when intraoperative cholangiogram fails or is unavailable.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.