
Abstract
Introduction
The optimal management of major stump complications (operative infection or dehiscence) following below-knee-amputation (BKA) is unknown. We evaluated a novel operative strategy to aggressively treat major stump complications hypothesizing it would improve our rate of BKA salvage.
Methods
Retrospective review of patients requiring operative intervention for BKA stump complications between 2015 and 2021. A novel strategy employing staged operative debridement for source control, negative pressure wound therapy, and reformalization was compared to standard care (less structured operative source control or above knee amputation).
Results
32 patients were studied, 29 of which were male (90.6%) with an average age of 56.1 ± 9.6 y. 30 (93.8%) had diabetes and 11 (34.4%) peripheral arterial disease (PAD). The novel strategy was used in 13 patients and 19 had standard care. Novel strategy patients had higher BKA salvage rates, 100% vs 73.7% (P = .064), and postoperative ambulatory status, 84.6% vs 57.9% (P = .141). Importantly, none of the patients undergoing the novel therapy had PAD, while all progressing to above-knee amputation (AKA) did. To better assess the efficacy of the novel technique, patients progressing to AKA were excluded. Patients undergoing novel therapy who had their BKA level salvaged (n = 13) were compared to usual care (n = 14). The novel therapy’s time to prosthetic referral was 72.8 ± 53.7 days vs 247 ± 121.6 days (P < .001), but they did undergo more operations (4.3 ± 2.0 vs 1.9 ± 1.1, P < .001).
Conclusion
Utilization of a novel operative strategy for BKA stump complications is effective in salvaging BKAs, particularly for patients without PAD.
Keywords
Introduction
Despite improvements in the management of peripheral vascular disease, it is estimated that 150 000 patients in the United States have non-traumatic lower-extremity amputations yearly. 1 Above-knee amputation (AKA) and below-knee amputation (BKA) are associated with significant morbidity and mortality, yet the import of maintaining a BKA has major physical (decreased energy expenditure) and emotional (quality of life) health benefits.
The incidence of BKA stump complications is disturbingly common, ranging from 8 to 18% of cases.2-5 Management of BKA stump complications varies considerably, ranging from antibiotics and/or local wound care to need for a more proximal amputation at the above-knee amputation (AKA) level. The conversion of BKA to AKA for stump complications has been reported at 12-51%.2-4,6 Nevertheless, a small single-center series of patients with non-healing BKAs reported an 86% ambulation rate for select patients who successfully underwent a re-do BKA compared to no patients that were revised to AKA. 7
To improve BKA salvage rates, our institution developed a novel operative strategy to manage BKA stump complications with a goal of reducing need for more proximal amputation. We hypothesized that this strategy would lead to improved outcomes and maintain the current amputation level compared to conventional surgical management.
Methods
Study Design
Following exemption from the Institutional Review Board at Harbor-UCLA Medical Center, consecutive patients undergoing two-stage non-traumatic BKA between 2015 and 2021 were identified retrospectively via CPT code and confirmed by chart review. At our institution, both vascular surgeons and acute care surgeons manage severe diabetic and ischemic foot complications requiring BKA. Because the acute care surgeons only utilize a two-stage approach to BKA (surgical indication unanimously being active infection), we tried to standardize the comparator by only studying a two-stage BKA, and not the single-stage BKA that is performed electively for chronic limb-threatening ischemia (CTLI). Patients lost to follow-up before the outcome of their BKA was known were excluded.
Patients with major BKA stump complications (infection or dehiscence) within 60-days, requiring surgical management were included. Patient demographics, comorbidities, indications for BKA (infection vs CTLI), time from guillotine amputation to formalization, and time from formalization to stump complication were collected. All comorbidities were extracted by chart review; the diagnosis of peripheral arterial disease (PAD) was confirmed by the authors based on imaging and/or prior vascular intervention. The nature of the stump complication and labs at time of complication were recorded. Patients who had a novel surgical approach to their BKA stump complication were compared to those having standard surgical care. The primary outcome was salvage rate of the BKA. Secondary outcomes included number of operations to manage the complication, ultimate ambulatory status, and time to prosthetic referral. Ambulatory status was defined as documentation of a patient being ambulatory with or without assistive devices (front wheel walker, cane, etc).
After initial analysis determined that patients progressing to AKA all had PAD, we did a separate analysis of patients who had their BKA salvaged comparing the novel technique to standard surgical care, evaluating aforementioned secondary outcomes.
Description of Standard and Novel BKA Stump Complication Salvage Techniques
Operations were usually performed under monitored anesthesia care with femoropopliteal nerve blocks. Standard therapies for a BKA stump complication included source control via incision and drainage or wound debridement with or without negative pressure wound therapy (NPWT) followed by healing via secondary intention. For several patients, AKA was pursued.
The novel technique involved a more aggressive surgical approach to the stump complication. In the first operation, any existing skin sutures or staples are removed and the deeper fascial sutures are cut to completely open the stump. Deep wound cultures are obtained to tailor antibiotics. Aggressive debridement of all infected soft tissues and bone to healthy tissue is performed (Figure 1(A)). Negative pressure wound therapy (NPWT) utilizing a black (or more recently utilized silver impregnated) sponge is applied to the open stump, bringing any remaining posterior flap anteriorly so it is not given the opportunity to retract (Figure 1(B)). The patient is maintained in the hospital between operations. Novel operative technique for BKA stump salvage. (A) In the first operation, the infected stump is opened widely, cultures taken, and aggressive debridement of necrotic and infected tissue performed. (B) Negative pressure wound therapy is applied to open stump to help keep the posterior myocutaneous flap from retracting. (C) Once the wound is clear of infected tissue, the first stage of re-formalization takes place, cutting back anterior soft tissue and bone ∼2 cm and resecting the deep posterior compartment. (D) In a subsequent operation, definitive closure is performed. (E) If there is insufficient skin/subcutaneous tissue coverage, placement of a dermal matrix followed by eventual split thickness skin grafting can be performed.
In 48-72 h, a second operation is planned. If there is any concern about the integrity of the tissue, further debridement ensues as in the first operation, with re-culturing, and repeat NPWT placement. If the wound appears healthy, reconstruction begins. As the existing posterior flap is generally insufficient to achieve definitive tibial coverage, and to ensure we are working with healthy tissue, our approach involves a “re-formalization” which involves excising 1-2 cm of proximal tibia and overlying skin and subcutaneous tissue. The majority of our initial BKAs are created with a tibial length of 10-12 cm below the tibial tuberosity. Thus, in this re-formalization, the anticipated tibial transection will be 8-10 cm below the tibial tuberosity. We have even gone up to 6 cm if necessary for source control or adequate muscular closure over the stump. We consistently use the gastrocnemius soleus complex and overlying skin as our posterior myocutaneous flap, excising the deep posterior compartment. The deep posterior musculature adds bulk to an already challenging short stump, without providing necessary tibial coverage. Once this first portion of the re-formalization is complete (Figure 1(C)), NPWT is applied as described previously.
In another 48-72 h, a final surgery of delayed primary closure is performed. The tibial bone is beveled and smoothed at its cut edge. The posterior myocutaneous flap is brought forward and trimmed appropriately. The fascia, dermal layer, and skin are closed in layers (Figure 1(D)). Of note, there have been several instances where skin was excised in the infectious debridement. In these cases, muscle only was closed over the stump and dermal matrix was used followed by skin grafting to salvage the stump (Figure 1(E)).
Statistical Analysis
Continuous variables are shown as means with standard deviations and were analyzed using independent student’s t tests. Categorical variables are shown as percentages and were analyzed using Chi-squared tests or Fisher exact tests. Statistical significance was defined as P-value <.05. All statistical analyses were performed using IBM Statistical Product and Service Solutions (SPSS).
Results
Over the 6-year study period, 126 patients underwent two-stage non-traumatic below-knee amputation. Forty-seven (37.3%) patients had surgical site complications; stump infections occurred in 29 and non-healing wounds or dehiscence in 18. 35 of the 47 patients required reoperation due to the severity of the complication. 3 of the 35 were lost to follow-up and excluded in the study.
Demographics of Patients With Major Stump Complications After Below-Knee Amputation (BKA).
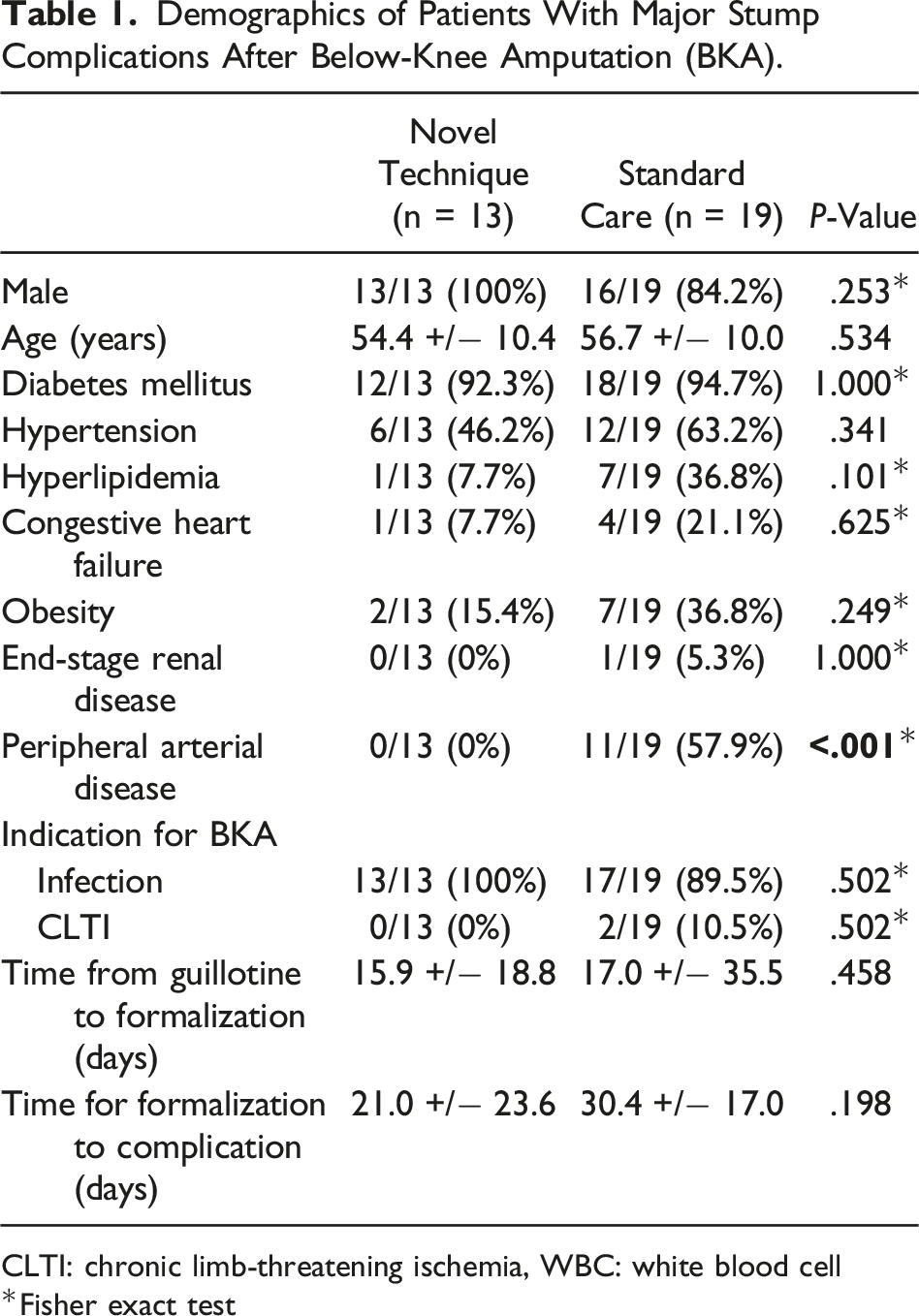
CLTI: chronic limb-threatening ischemia, WBC: white blood cell
*Fisher exact test
Stump Complication Data and Outcomes for Novel Operative Treatment Vs Standard Care.
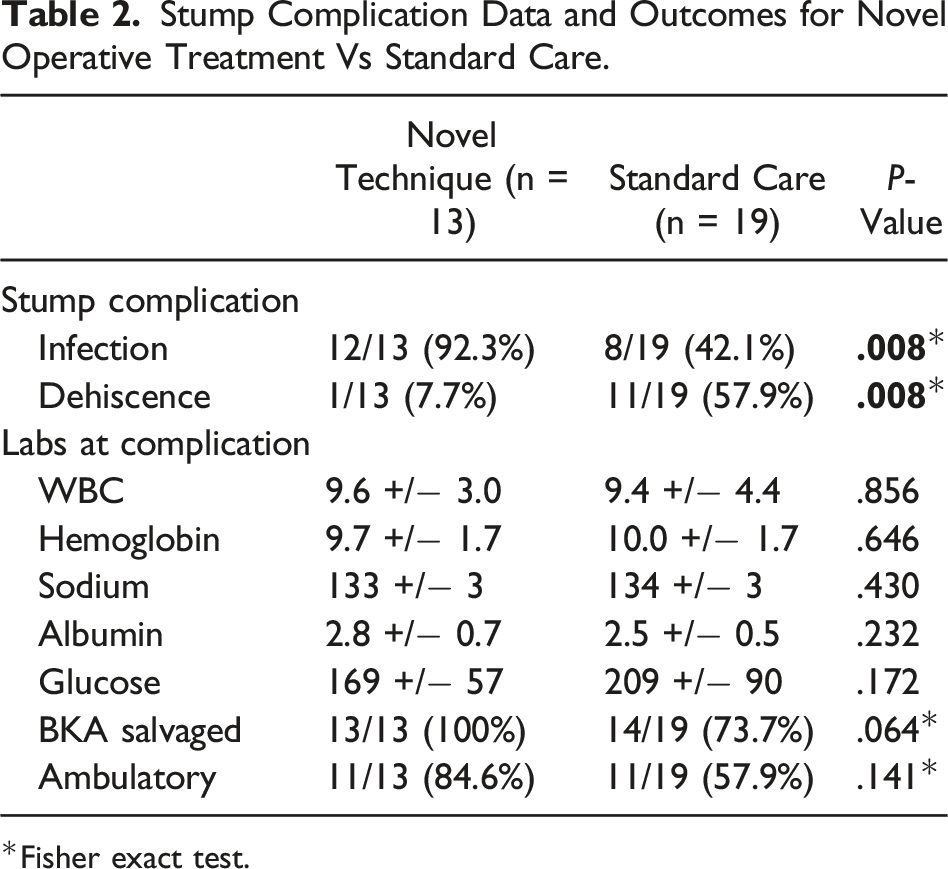
*Fisher exact test.
Demographics and Outcomes of Novel Operative Technique Vs Standard Care in Patients Whose BKA Stumps Were Salvaged.
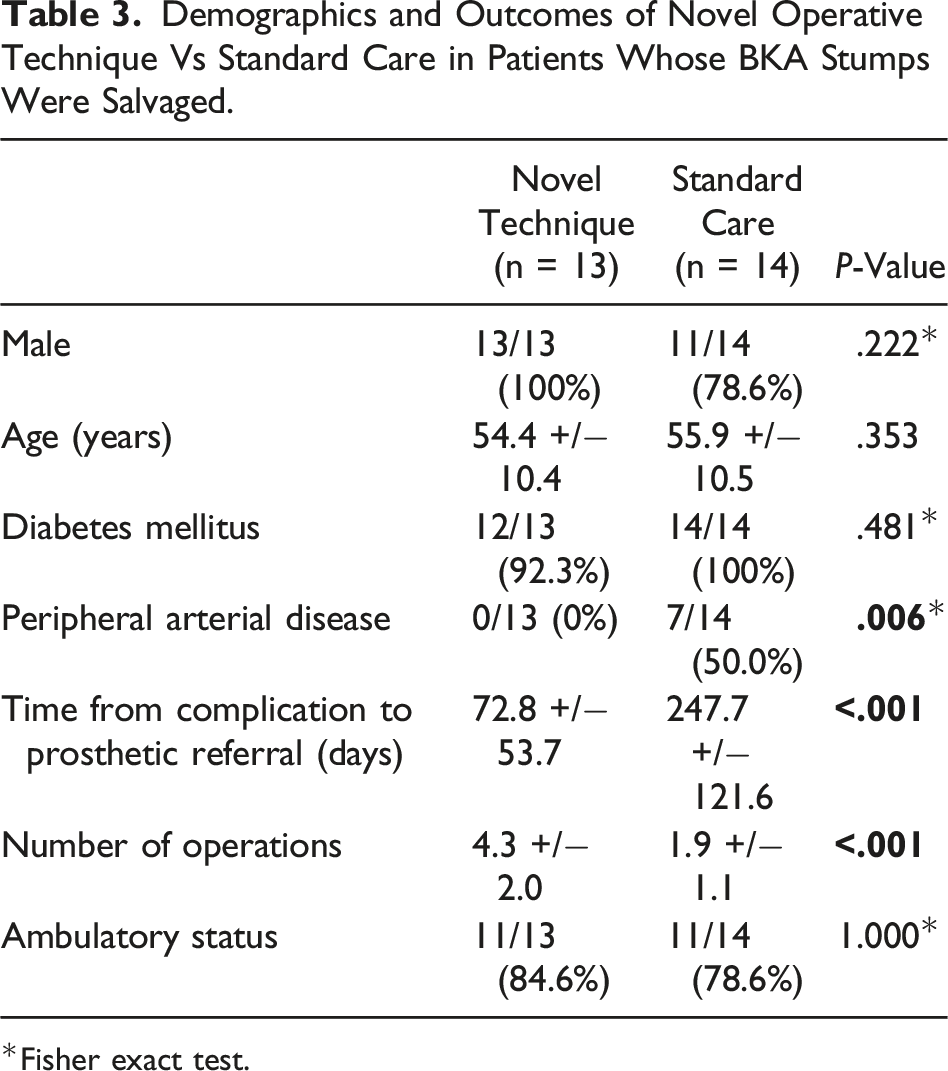
*Fisher exact test.
Discussion
Successfully managing major BKA stump complications is imperative in preventing more proximal amputation and restoring ambulatory status for patients. In this study, a novel operative approach to sterilize the wound bed and re-formalize the stump not only had a 100% success rate with stump salvage, but it also allowed for faster stump healing and prosthetic referral.
This study adds to the existing body of literature on BKA stump complications. In our study cohort, both the 37.3% BKA stump complication rate and 27.7% reoperation rate on stump complications were higher than what have been previously reported.3,4 Our study is unique in that over 90% of our patients were diabetic, and we exclusively studied patients undergoing two-stage BKA, a group predisposed to having a higher rate of infection. Most of the existing literature on BKA complications has focused on patients with peripheral arterial disease (PAD) who more often undergo single-stage amputations. Furthermore, most studies only report complications within 30 days, yet we extended our study to 60 days. A separate single-institution study found that 38% of BKAs were reoperated on with a median of 54 days postoperatively, suggesting that our complication rates are reflective of expected outcomes. 8
The optimal management of stump complications has not been studied, but some authors report if there is an infection of a stump, almost all patients require revision to a more proximal level. 2 In our study, we report a technique for infected BKA stumps that resulted in 100% salvage at the below-knee level. This is in contradiction to the literature stating that between 12 and 51% of patients with stump complications will progress to AKA.2-4,6 In fact, in our standard surgical arm, five patients (26%) progressed to AKA, consistent with aforementioned studies.
So, the real crux of this discussion is why certain patients underwent the novel approach and why others received standard surgical care. Our acute care surgery group manages relatively young (on average 10 y younger than in other amputation series), ambulatory, diabetic patients who undergo BKA for infection. When these patients return with stump infections, many times simple incision and drainage will not suffice. The idea of young patients progressing to an AKA, understanding that the majority of patients who fail stump salvage also do not regain ambulatory status and have an associated higher 1-year mortality, 9 felt unfathomable. It is for these reasons that we created an aggressive management strategy, obtaining source control and redoing the formalization to see if we could salvage the stump.
Our comparator group was less severe infections managed within our own surgical group and BKA complications managed by our vascular colleagues. Importantly, none of the patients who underwent our novel technique had PAD, and all the patients who progressed to AKA did. What we can conclude is that the novel surgical therapy is successful in a diabetic patient population without PAD. A major limitation (or actually uncertainty) is the applicability of this technique to patients with PAD. We feel next steps would be to try this strategy in patients with PAD who had a stump complication in which ischemia did not warrant AKA. Another single institution study reported an 86% healing and ambulatory rate for revising 14 non-healing BKAs; 13 of the patients had a palpable popliteal pulse and the authors conclude that a popliteal pulse is an important consideration in surgical planning. 7 Clearly, the degree and level of PAD have a critical role in wound healing; we offer this technique as something to try in patients who surgeons feel have perfused tissue.
When we excluded patients who progressed to AKA and compared patients who had BKA salvage, our novel surgical therapy resulted in a significantly decreased time to prosthetic referral compared to standard surgical care (72.8 ± 53.7 days vs 247 ± 121.6 days), though overall ambulatory status was not different. This could have major benefits to younger patients who need to return to work. Alternatively, patients in the novel technique group underwent significantly more surgeries, 4.3 ± 2.0 vs 1.9 ± 1.1, than patients having standard operative therapy. While we did not have any perioperative mortalities, we acknowledge that anesthetic risks are not inconsequential and the risks and benefits of embarking on BKA salvage should be weighed carefully.
Another limitation of this study is we do not analyze hospital length of stay or costs. For our under-resourced (and often uninsured) patient population, length of stay is consistently inaccurate due to a multitude of barriers to discharge, so it is not reported. We do appreciate that performing more operations is more costly and results in a longer length of stay in most hospital systems. Yet for our patients, achieving definitive wound closure as soon as possible actually hastens and facilitates discharge. Generalizability of this study to all hospital systems is uncertain. Separate analyses between hospital costs vs home health and follow-up costs and quality of life for patients who have earlier definitive wound closure and prosthetic referral would need to be entertained in a different care setting.
The operative technique described in this article may be at odds with traditional surgical thinking where after opening an infected field, wound closure is not performed due to the risk of recurrent infection. Our data suggest that after appropriate source control with concurrent antibiotics, once bony and myofascial spaces have been adequately sterilized, reformalization can be safely performed. This is in no small part due to the use of negative pressure wound therapy (NPWT). Negative pressure wound therapy is a critical wound care adjunct in the management of these patients as it has been shown to have a multitude of beneficial effects on wound healing including removal of exudate, physical wound contracture, and promotion of angiogenesis. 10
Another important consideration of the novel surgery is the impact of higher tibial transection on postoperative functional status. Our standard practice in the initial two-stage BKA is to transect the tibia 10-12 cm from the tibial tuberosity. With the novel technique, stump complications required a revision of tibial length by ∼ 2 cm. Our success with shorter tibial lengths has been corroborated in another case series with patients who undergo BKA with short (10 cm to 8 cm) and ultra-short stumps (5 cm to 7.5 cm), and even stumps where the tibial transection is just below the tibial tuberosity.11,12 These stumps can still undergo prosthetic fitting with excellent ambulatory outcomes. Regardless of stump length, however, the ambulatory rate in our cohort of patients who underwent BKA salvage is higher than the 73.9% rate found in the literature. 13
Conclusion
An aggressive, staged surgical management technique of major BKA stump complications can yield an excellent rate of stump salvage, faster time to prosthetic referral, and high rate of postoperative ambulatory status. It should be considered an option for BKA stump complications in diabetic patients. Its utility in patients with peripheral vascular disease remains untested.
Footnotes
Author Contributions
NB: study design, literature search, data collection and interpretation, and writing. XQ: study design and data collection. JK: study design, writing, and critical revision. AN: study design, literature search, data interpretation, writing, and critical revision
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.