
Abstract
Introduction
Breast surveillance in patients with BRCA mutations include mammography (MMG) and MRI. Patients may elect to undergo risk-reducing bilateral prophylactic mastectomies (BPM). Sentinel lymph node biopsies (SLNB) are frequently performed and associated with increased morbidity. This study sought to determine the correlation between preoperative imaging and the final pathology and evaluate the role of SLNB in these high-risk patients.
Methods
A prospective database identified BRCA patients who underwent BPM between 2006 and 2022. Imaging, pathology, and operative reports were reviewed.
Results
170 patients with BRCA 1/2 mutations were identified. 162 (95.3%) had imaging within one year of BPM. Of these, 28 (17.3%) patients had a MMG/ultrasound, 53 (32.7%) had an MRI, and 81 (50%) had both; 21/162 (13.0%) patients had abnormal imaging. Bilateral SLNB were performed in 31 (18.2%) patients, of which 7 had abnormal imaging; unilateral SLNB were performed in 4 (2.4%) patients, of which 3 had abnormal imaging. 11/170 (6.4%) patients had a malignancy and only one (9%) of these patients had imaging abnormalities. 1/170 (0.6%) patient had an invasive carcinoma requiring an axillary lymph node dissection (ALND), and 10/170 (5.9%) patients had ductal carcinoma in situ (DCIS). 25/170 (14.7%) had ADH/ALH. Only 7/170 (4.1%) patients had imaging abnormalities and abnormal pathology. All SLNB and ALND performed demonstrated no metastatic disease.
Discussion
There is a high rate of discordance between preoperative imaging prior to surgery in BRCA patients undergoing prophylactic mastectomies and final pathology. This study does not support routine SLNB at the time of BPM.
• The rate of occult malignancy in patients with a BRCA mutation at the time of bilateral prophylactic mastectomy (BPM) is low. • Preoperative imaging done prior to surgery poorly predicted final pathology. • There were no patients with a BRCA mutation who benefited from SLNB at the time of BPM.Key Takeaways
Introduction
BRCA1 and BRCA2 deleterious mutations carry a significant risk of future breast cancer development. The estimated risk of developing breast cancer by age 80 in patients that carry these mutations are 72% and 69%, respectively. 1 Risk-reduction strategies include semi-annual imaging surveillance with MRI and mammogram (MMG), prophylactic mastectomy, prophylactic salpingo-oophorectomy, and chemoprevention. 2 With increasing public awareness and acceptance, bilateral prophylactic mastectomies (BPM) are being increasingly performed and provide a 90% to 95% risk reduction in BRCA mutation carriers. 3
The current recommendation for surveillance in BRCA1/2 patients is an annual breast MRI between the ages of 25 and 29 and an additional annual MMG between the ages of 30 and 75. 2 MRI has a higher sensitivity (77% to 94%) in comparison to MMG (22% to 59%) in detecting breast cancer in this high-risk population.2,4,5 However, MRI has a much lower specificity, ranging from 22% to 50% and in patients with BRCA mutations, the rate of a false positive MRI is 80% to 83%.4,6,7
Prior studies have demonstrated that patients with a hereditary predisposition for breast cancer undergoing BPM have a low incidence (<5%) of incidental invasive carcinoma.3,7-14 If the preoperative imaging is abnormal, the patient should undergo a biopsy prior to BPM. There is growing evidence to suggest that there is no need for routine sentinel lymph node biopsies (SLNB) at the time of the mastectomy, especially if the preoperative breast MRI is normal.5,10,13 However, there are no clear guidelines as to whether an SLNB should be performed in the setting of an abnormal MRI. This begs the question as to how accurate preoperative imaging is in detecting breast cancer, specifically in BRCA mutation carriers who tend to be younger and have dense breast tissue.
The argument in favor of performing a SLNB at time of BPM would be to spare patients an axillary lymph node dissection (ALND) if an incidental invasive disease is identified on final pathology. While SLNB do carry less morbidity than ALND, it is not without complications. SLNB are associated with paresthesia, decreased range of motion, and lymphedema in addition to prolonged operating room time and increased costs.7,15 Only 1% to 3.5% of patients undergoing BPM or contralateral prophylactic mastectomies (CPM) have been shown to benefit from SLNB at the time of surgery, sparing them an ALND.5,7 Prior literature evaluating preoperative imaging, incidental cancer, and the role of SLNB in high-risk patients include patients with a history of breast cancer undergoing CPM, as opposed to a breast cancer naïve cohort. We hypothesize that the incidence of occult malignancy in BRCA1/2 mutation carriers undergoing BPM is low, obviating the need for SLNB. This study sought to compare the preoperative imaging with the final pathology of the breast specimen and evaluate the role of SLNB in BRCA 1/2 mutation carriers undergoing BPM without evidence of breast cancer.
Methods
This study was performed after the approval of our Institutional Review Board. A prospectively maintained institution database was used to identify patients with BRCA1 or BRCA2 mutations who underwent BPM between 2006 and 2022. Deep-6 AI natural language processing software (Deep6 AI, Pasadena, CA) was used to include additional patients. The search terms “BRCA1” OR “BRCA2” AND “bilateral prophylactic mastectomy” OR “prophylactic mastectomy” were used. Inclusion criteria included patients >18 years of age with a known BRCA1 or BRCA2 mutation who underwent BPM. Patients with a known personal history of breast cancer, unavailable or undocumented preoperative imaging, or unavailable pathology were excluded. Demographics, type of BRCA mutation, preoperative imaging including MRI, MMG and/or ultrasound (US), type of operation, whether a SLNB was performed, and final surgical pathology were reviewed. The type of operation and decision to perform a SLNB were left to the discretion of the surgeon.
Normal or benign imaging results were defined as Breast Imaging Reporting and Data System (BI-RADS) 1, 2, or 3 and those with BI-RADS 0, 4, or 5 were considered abnormal. Abnormal pathology included atypical lobular hyperplasia (ALH), atypical ductal hyperplasia (ADH), ductal carcinoma in situ (DCIS), or invasive carcinomas. Lobular carcinoma in situ (LCIS) was not considered abnormal, but was noted.
Results
Patient Characteristics.
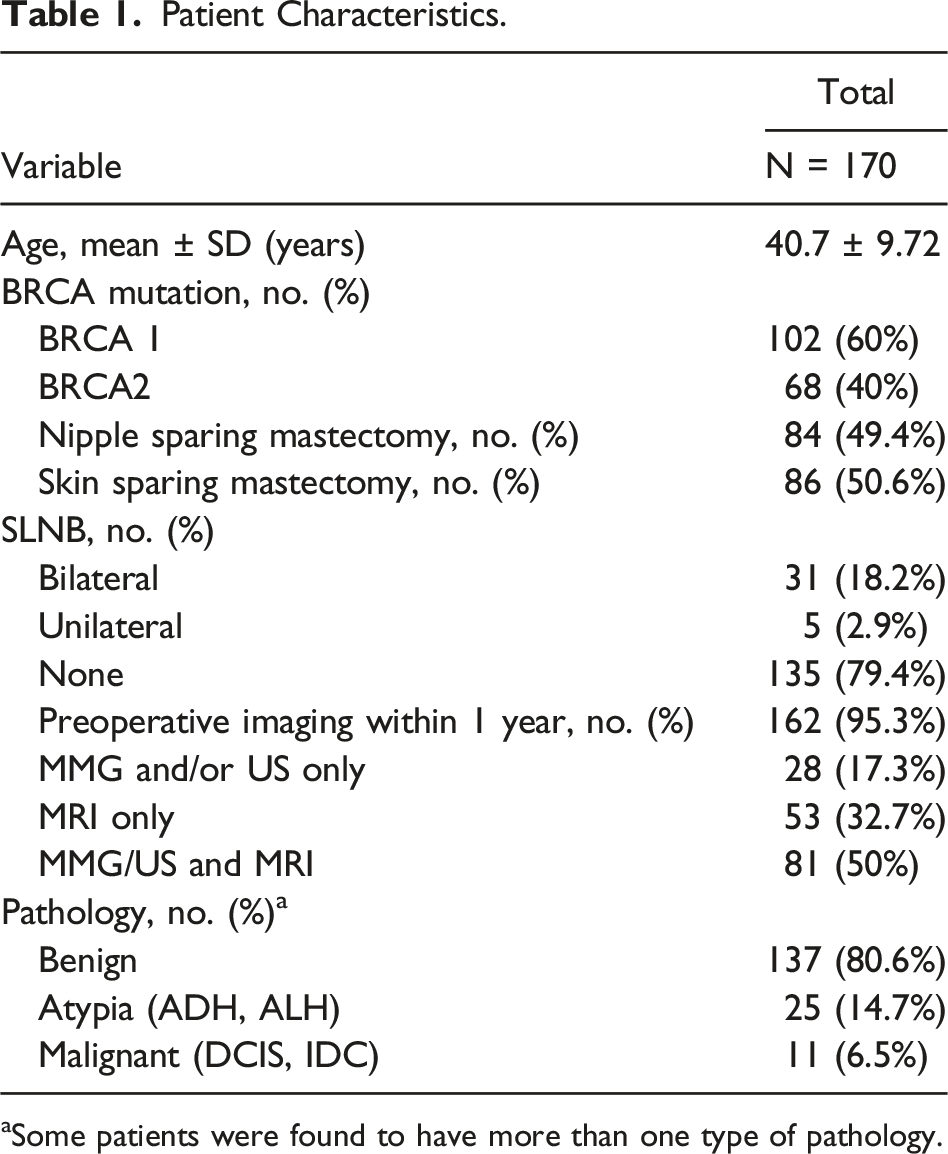
aSome patients were found to have more than one type of pathology.
Normal Preoperative Imaging and BPM
Overall, 149 patients had normal preoperative imaging prior to BPM. Of these, 26 (17.4%) patients were incidentally found to have abnormal pathology: 1 with invasive ductal carcinoma (IDC), 6 with DCIS alone, 12 with atypical disease alone, 4 with concurrent atypia and LCIS, and 3 with concurrent atypia and DCIS (Figure 1). The patient who was found to have IDC had both a normal MMG/US performed within 1 year and a normal MRI performed 3.5 months prior to BPM. Flowchart of final pathology based on preoperative imaging.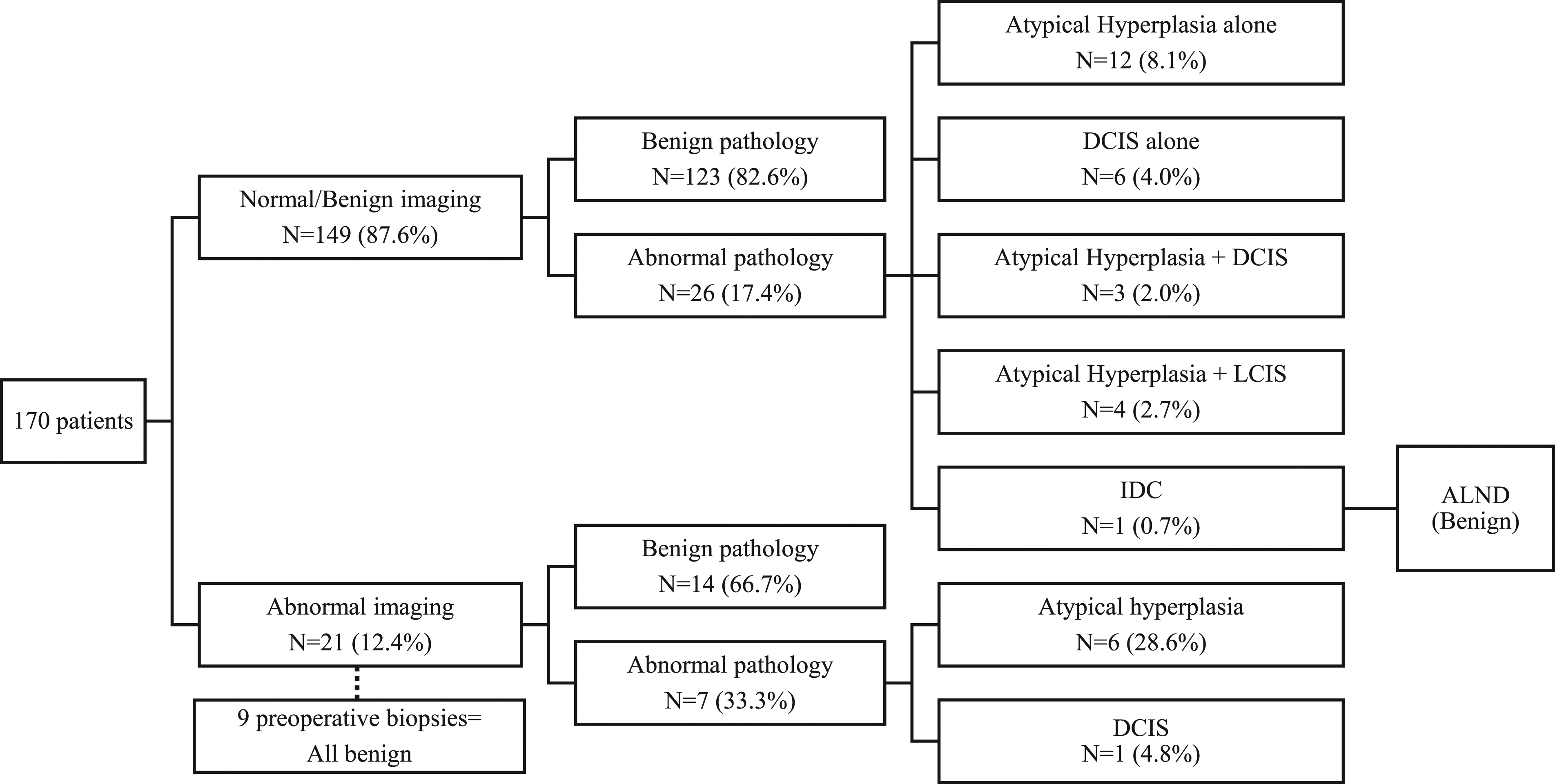
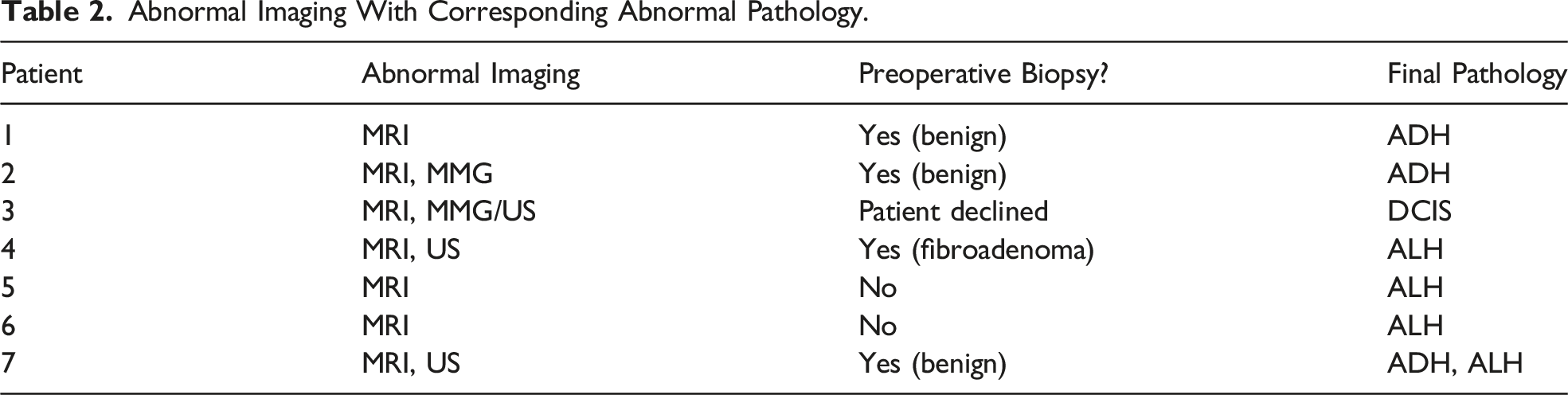
Abnormal Preoperative Imaging and BPM
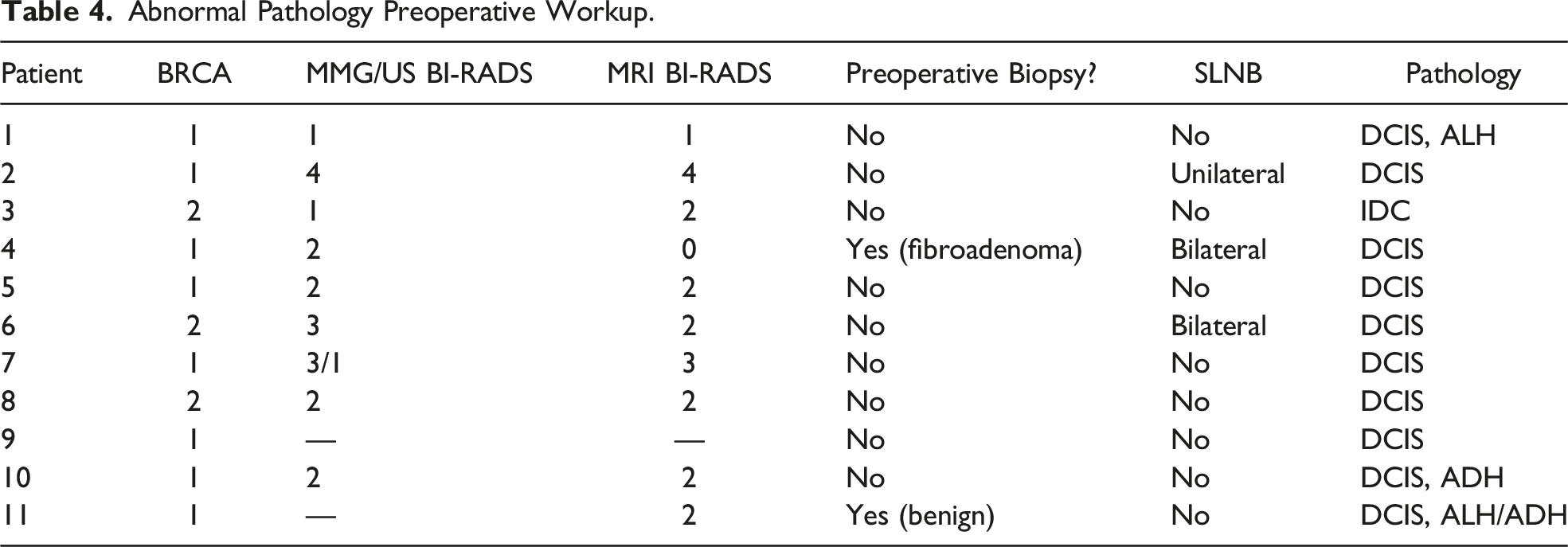
Abnormal Imaging With Corresponding Abnormal Pathology.
SLNB and BPM
A total of 35 (20.6%) patients had SLNB performed: 31 bilateral and 4 unilateral. SLNB were not performed in 135 (79.4%) of patients. Of those who underwent a SLNB, 9 (25.7%) patients had abnormal preoperative imaging: 6 MRI, 1 MMG/US, and 2 with both an abnormal MRI and MMG/US. Of these, 6 (66.7%) underwent bilateral SLNB and 3 (33.3%) underwent unilateral SLNB. The median number of sentinel lymph nodes excised was 3 (range 1 to 10). All sentinel nodes were negative for metastatic disease on final pathology. In total, 9 patients who underwent SLNB were found to have abnormal breast pathology: 6 atypical proliferative lesions and 3 with DCIS. There were no patients in this group who were found to have invasive disease and would have benefited from SLNB.
One patient with normal preoperative imaging underwent a unilateral SLNB. This patient had a fibroadenoma that was excised 12 years prior to BPM. Although the preoperative imaging was normal with multiple benign-appearing tiny enhanced lesions (BI-RADS 3), the patient requested to undergo an ipsilateral SLNB.
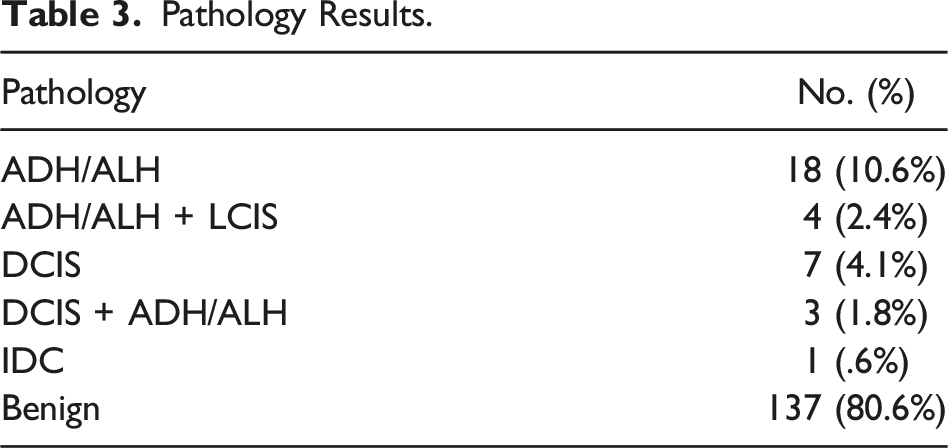
Abnormal Pathology
Pathology Results.
Abnormal Pathology Preoperative Workup.
Discussion
The goal of BPM in patients with a BRCA mutation is to minimize the risk of developing breast cancer. The impact of BPM has been well documented and now with the success of post-mastectomy breast reconstruction, is becoming more appealing to patients. This study demonstrates a low incidental finding of malignancy (6.4%) with an even lower incidence of invasive disease (0.6%). Thompson et al 12 conducted a similar study and evaluated a subgroup of high-risk patients who underwent BPM with a 1.7% rate of occult malignancy, half of which were invasive cancer. 66.7% of patients with an occult malignancy had a normal MRI within 1 year of surgery and 1 patient underwent a core needle biopsy that demonstrated ADH. While they focused on the incidence and factors associated with occult malignancy, this study evaluated the use of preoperative imaging in BRCA patients undergoing BPM and the role of SLNB.
Preoperative imaging findings were not always predictive of the final pathology. Only 4.8% of patients with abnormal imaging were also found to have cancer. McLaughlin et al 5 found that only 6 of 178 (3.4%) patients undergoing prophylactic mastectomies had abnormal preoperative imaging and concordant cancer. In a study by Black et al, 7 5 suspicious MRI findings in high-risk patients undergoing prophylactic mastectomies led to 3 breast US, 1 MMG, 1 CT scan, and 5 SLNB. Although it is unclear if these patients underwent preoperative biopsies, 4 were false-positive findings and only 1 was a true positive finding. In the patient with a true positive finding, IDC was detected on MRI. The false positive rate was 80% and MRI failed to detect 3 of 4 cancers. After a cost analysis, the authors determined that abnormal MRI findings led to an additional average cost of $1,207 per patient. Our study echoes these findings as MRI failed to detect 8 of 10 malignancies.
MRI has a high sensitivity and is a useful tool in breast cancer screening in this population. Although preoperative imaging is not always predictive of final pathology findings, this is not to say that there is no role for surveillance imaging. It is important to note that this study does not account for patients with preoperative imaging that detected malignancies, as they were excluded. However, in patients who have already elected to undergo a BPM, preoperative imaging could potentially lead to unnecessary procedures. Twenty-one patients had abnormal imaging (18 of which were MRI findings) that only corresponded to 6 atypical hyperplasias and 1 DCIS. Therefore, suspicious findings should be biopsied to rule out malignancy, but in the setting of benign preoperative workup findings, a SLNB is not warranted.
Potential complications after undergoing SLNB have been well described. Patients enrolled in the Z0010 trial were found to have complications including: 8.6% axillary paresthesia, 3.8% decreased range of motion, and 7% lymphedema at 6 months.7,15 Additionally, they are exposed to a 0.1% risk of anaphylaxis when isosulfan blue dye is used and 30-day complications including axillary wound infections, hematomas, seromas, 15 and a potential second incision resulting in poor cosmesis. Nagaraja et al 9 performed a meta-analysis of 2,708 patients who underwent SLNB at time of prophylactic mastectomy with an occult cancer rate of 1.8% and positive SLNB in 1.3% of patients. Only 0.96% benefitted from undergoing a SLNB, avoiding subsequent ALND. Due to the increased surgical morbidity and low risk of incidental malignancy in patients undergoing CPM, the American Society of Breast Surgeons recommends against routine SLNB in patients undergoing CPM. 16 Although this consensus was directed toward patients undergoing CPM, this reasoning could also be applied to those undergoing BPM. In a survey of 238 surgeons, 91.9% felt that the rate of encountering a positive SLNB in patients undergoing a prophylactic mastectomy was minimal (<2%). Therefore, 67.1% said that they would never perform an SLNB, 26.3% sometimes perform a SLNB, and only 6.6% always perform an SLNB in the setting of prophylactic mastectomies. 17 None of the patients in our study benefited from undergoing a SLNB. There was only 1 patient found to have invasive disease; however, this patient’s preoperative imaging was normal, thus a biopsy or SLNB was not warranted. While the decision to perform a SLNB should be a discussion between the patient and surgeon, Wong et al 13 found that factors associated with an elevated risk of occult malignancy in high-risk patients included being older than 60 years with a history of breast cancer, BI-RADS 4 findings on MRI within 6 months, or a preoperative biopsy. While these factors should be kept in mind, it is important to note that these findings are not solely based on a breast cancer naïve cohort.
Our study is not without limitations. First, many patients were referred to our center from other institutions with prior workup including preoperative imaging and biopsy results. Therefore, there may have been variation amongst diagnostic imaging and radiology interpretation. In addition, the rate of incidental cancers detected by preoperative imaging could not be determined as patients with cancer confirmed on the preoperative biopsy were excluded.
Alternatively, surgeons may consider utilizing intraoperative pathology, performing a delayed SLNB, or using superparamagnetic iron oxide (SPIO) tracers.14,18-21 SPIO tracers is similar to radioactive tracers or dye, however it can be detected up to 3 weeks after injection. 18 Currently, our institution does not perform delayed SLNB or use SPIO tracers; therefore, patients found to have invasive disease would undergo an ALND for further staging. While our study did not evaluate the role of intraoperative pathology findings, SPIO tracers, or delayed SLNB, these should be considered.
Preoperative imaging is an important part of the workup prior to BPM. However, given the radiologic-pathologic discordance, if further workup including a preoperative biopsy is benign, a SLNB should not be performed. This, in addition to the low rate of incidental invasive malignancies, this study does not support routine SLNB at the time of BPM in BRCA mutation carriers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.