
Abstract
Background
Motor vehicle collision (MVC) is a leading cause of accidental death in children. Despite effective forms of child safety restraint (eg, car seat and booster seat), studies demonstrate poor compliance with guidelines. The goal of this study was to delineate injury patterns, imaging usage, and potential demographic disparities associated with child restraint use following MVC.
Methods
A retrospective review of the North Carolina Trauma Registry was performed to determine demographic factors and outcomes associated with improper restraint of children (0-8 years) involved in MVC from 2013 to 2018. Bivariate analysis was performed by the appropriateness of restraint. Multivariable Poisson regression identified demographic factors for the relative risk of inappropriate restraint.
Results
Inappropriately restrained patients were older (5.1 years v. 3.6 yrs, P < .001) and weighed more (44.1 lbs v. 35.3 lbs, P < .001). A higher proportion of African American (56.9% v. 39.3%, P < .001) and Medicaid (52.2% v. 39.0%, P < .001) patients were inappropriately restrained. Multivariable Poisson regression showed that African American patients (RR 1.43), Asian patients (RR 1.51), and Medicaid payor status (RR 1.25) were associated with a higher risk of inappropriate restraint. Inappropriately restrained patients had a longer length of stay, but injury severity score and mortality were no different.
Discussion
African American children, Asian children, and Medicaid insurance payor status patients had an increased risk of inappropriate restraint use in MVC. This study describes unequal restraint patterns in children, which suggests opportunity for targeted patient education and necessitates research to further delineate the underlying etiology of these differences.
• Inappropriate restraint of children involved in motor vehicle collisions remains a significant public health issue. • This study describes unequal restraint patterns in children by age, race, and insurance payor status. • There is a need for bolstering of pediatric trauma databases to include more nuanced socioeconomic variables.Key Takeaways
Introduction
Despite improvement in recent years, motor vehicle collision (MVC) remains a leading cause of death in children in the United States.1–4 Specifically, MVC is the second most common cause of accidental death among children 0 to 4 years of age and the leading cause of accidental death among children 5 to 9 years of age.5,6 To reduce morbidity and mortality of children involved in MVCs, children under 8 years of age should be positioned in the rear seat and secured using a supplemental restraint such as a car seat or a booster seat. 7 There is evidence that supplemental restraint use decreases mortality of children involved in MVC.8–10 Furthermore, car and booster seat use reduces injury severity following MVC.11,12
Unfortunately, studies have demonstrated relatively poor compliance with established restraint guidelines for children. 13 In addition, studies have identified demographic disparities in appropriate restraint use in children.13–17 There are limited data evaluating the relationship between socioeconomic factors and impact on the likelihood of appropriate restraint in children. To date, studies have shown that African American children, Hispanic children, and patients with Medicaid payor status may be at the highest risk for inappropriate restraint.16,17 However, there are significant gaps in the literature regarding socioeconomic risk factors for inappropriate restraint use in children. For example, there is only one study that controls for insurance payor status when determining race as a risk factor for inappropriate restraint. 17 There are potential confounding socioeconomic variables that have not been considered by prior studies. A more nuanced review of available data is needed.
The primary objective of this study was to delineate potential demographic disparities in restraint use by children following MVC. The secondary objectives of this study were to assess the impact of restraint status on injury severity, patterns of imaging and procedures, and patient outcomes including mortality.
Methods
A retrospective review of the North Carolina Trauma Registry was performed to determine demographic factors and outcomes of children involved in MVC. The registry includes data from 17 trauma centers across the state, comprising 6 level I, 3 level II, and 8 level III trauma centers.
Appropriate Restraint Type by Age and Weight.
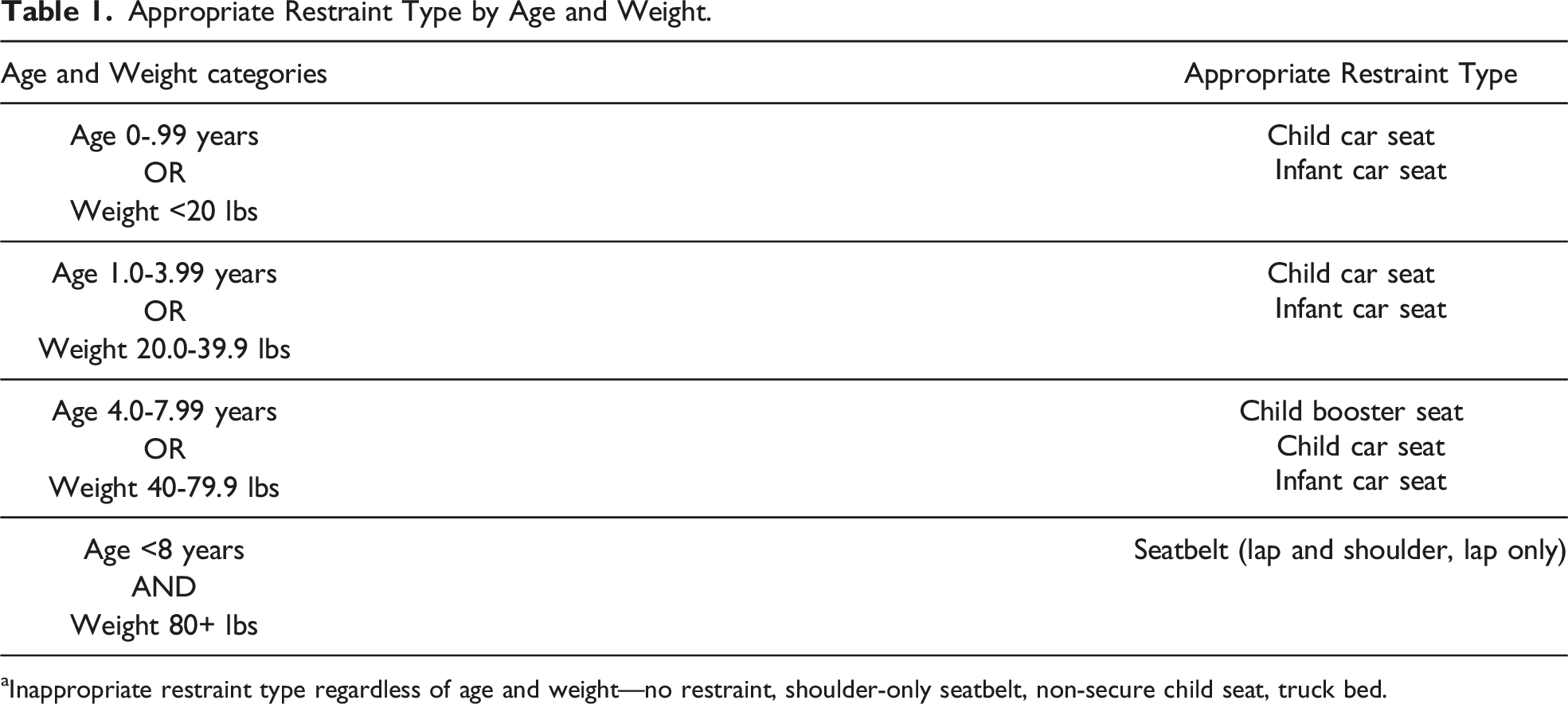
aInappropriate restraint type regardless of age and weight—no restraint, shoulder-only seatbelt, non-secure child seat, truck bed.
The database was queried for demographic characteristics including patient age, weight, sex, race, ethnicity, and payor status. Race was categorized as White, African American, Asian, and other. Ethnicity was categorized as Hispanic/Latinx or non-Hispanic/Latinx. Payor status was categorized as private, Medicaid, self-pay, CHAMPUS (Civilian Health and Medical Program of the Uniformed Services), or auto.
The database was also queried for outcomes including injury severity score (ISS), Glasgow Coma Scale (GCS) on arrival, the necessity of cardiopulmonary support, transfusion requirement during hospitalization, length of stay (LOS), and mortality. Imaging patterns, including the use of X-ray, ultrasound, computed tomography (CT), and magnetic resonance imaging (MRI), were also assessed. Finally, patients’ procedural requirements were assessed by procedure location, including those performed on the head, face, neck, chest, abdomen, extremity, spine, and skin.
Statistical Analysis
Univariate analysis was performed to evaluate data distribution and missing values in the database. The registry had less than 7% data missing in all included variables. Bivariate analysis was performed by the appropriateness of restraint, utilizing χ2 for categorical variables and Kruskal-Wallis for non-normally distributed continuous variables.
Multivariate Poisson regression was performed to determine the patient characteristics affecting the relative risk of being inappropriately restrained. A priori, race, ethnicity, and insurance status were included in the model. All patient demographics and characteristics were included a priori or not significant on bivariate analysis. No other covariates were included in the model after bivariate analysis. A backward elimination approach was utilized to reduce error and improve precision (narrowing of confidence intervals) in the model. No independent variables were removed.
This study was approved by the institutional review board at the University of North Carolina School of Medicine, Chapel Hill, North Carolina.
Results
Patient Demographics and Characteristics by Appropriateness of Restraint.
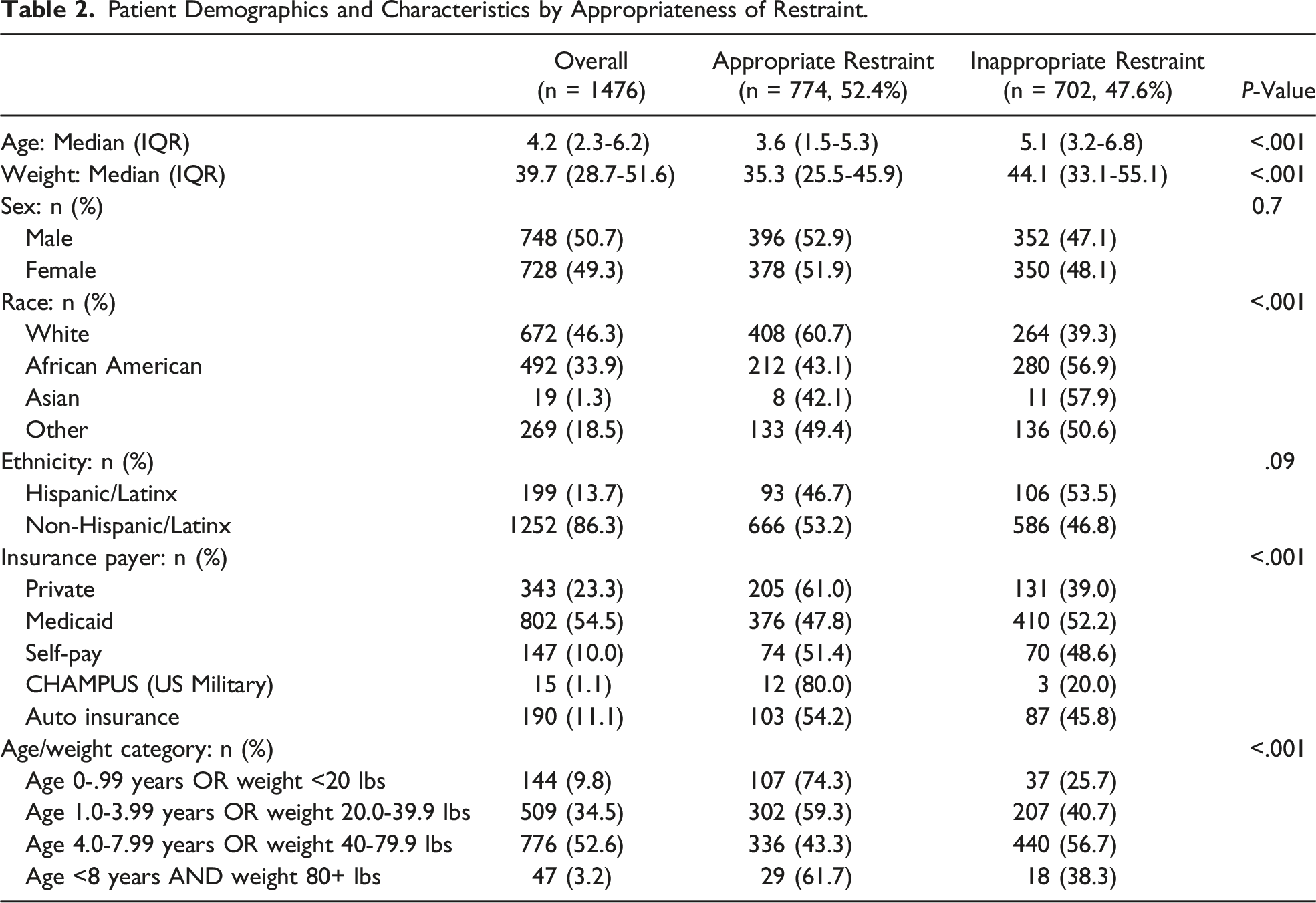
There was no difference in proportion of males and females who were appropriately restrained (n = 396, 52.9% v. n = 378, 51.9%, P = .7). However, there was a difference based on age and weight. Inappropriately restrained patients were older (5.1 yrs, IQR 3.2-6.8 v. 3.6 yrs, IQR 1.5-5.3, P < .001) and weighed more (44.1 lbs, IQR 33.1-55.1 v. 35.3 lbs, IQR 25.5-45.9, P < .001). A higher proportion of African American children were inappropriately restrained than White children (n = 280, 56.9% v. n = 264, 39.3%, P < .001). In addition, a higher proportion of patients with Medicaid insurance were inappropriately restrained than patients with private insurance (n = 410, 52.2% v. n = 131, 39.0%, P < .001). A similar proportion of Hispanic/Latinx and non-Hispanic/Latinx patients were appropriately restrained (n = 93, 46.7% v. n = 666, 53.2%, P = .09) (Table 2).
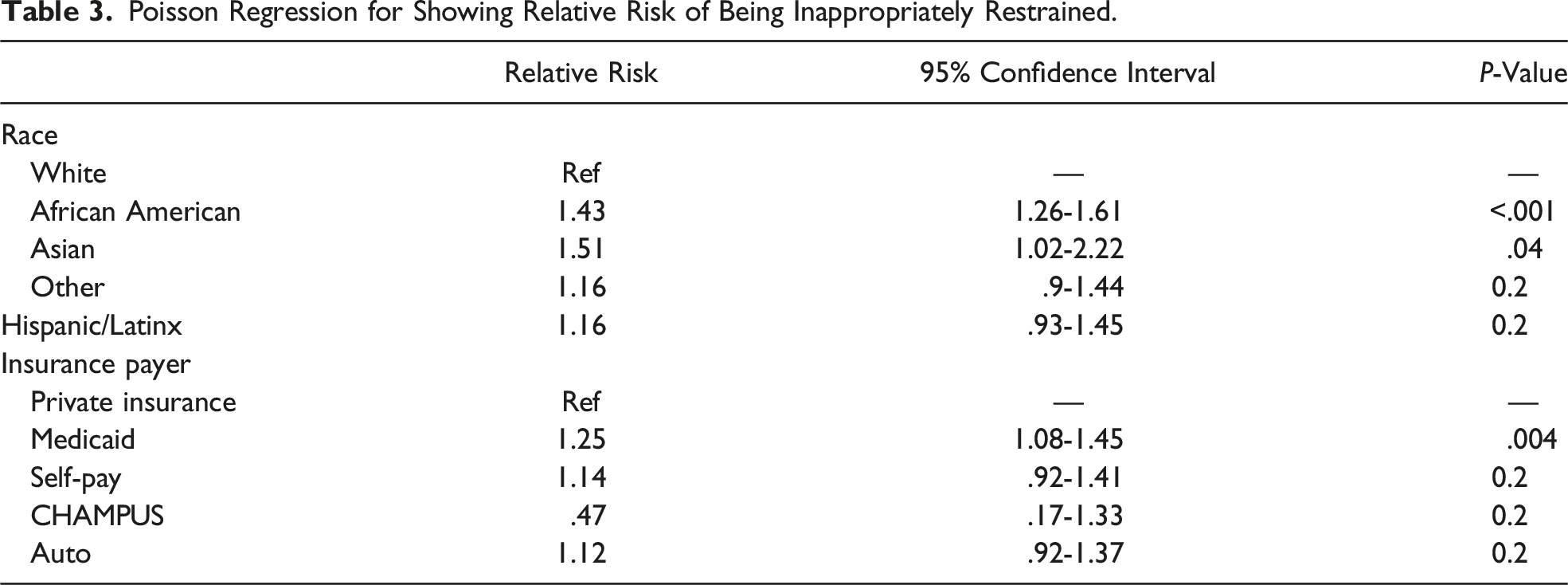
Poisson Regression for Showing Relative Risk of Being Inappropriately Restrained.
Patient Outcomes, Imaging Patterns, and Procedure Requirements by Appropriate and Inappropriate Restraint.
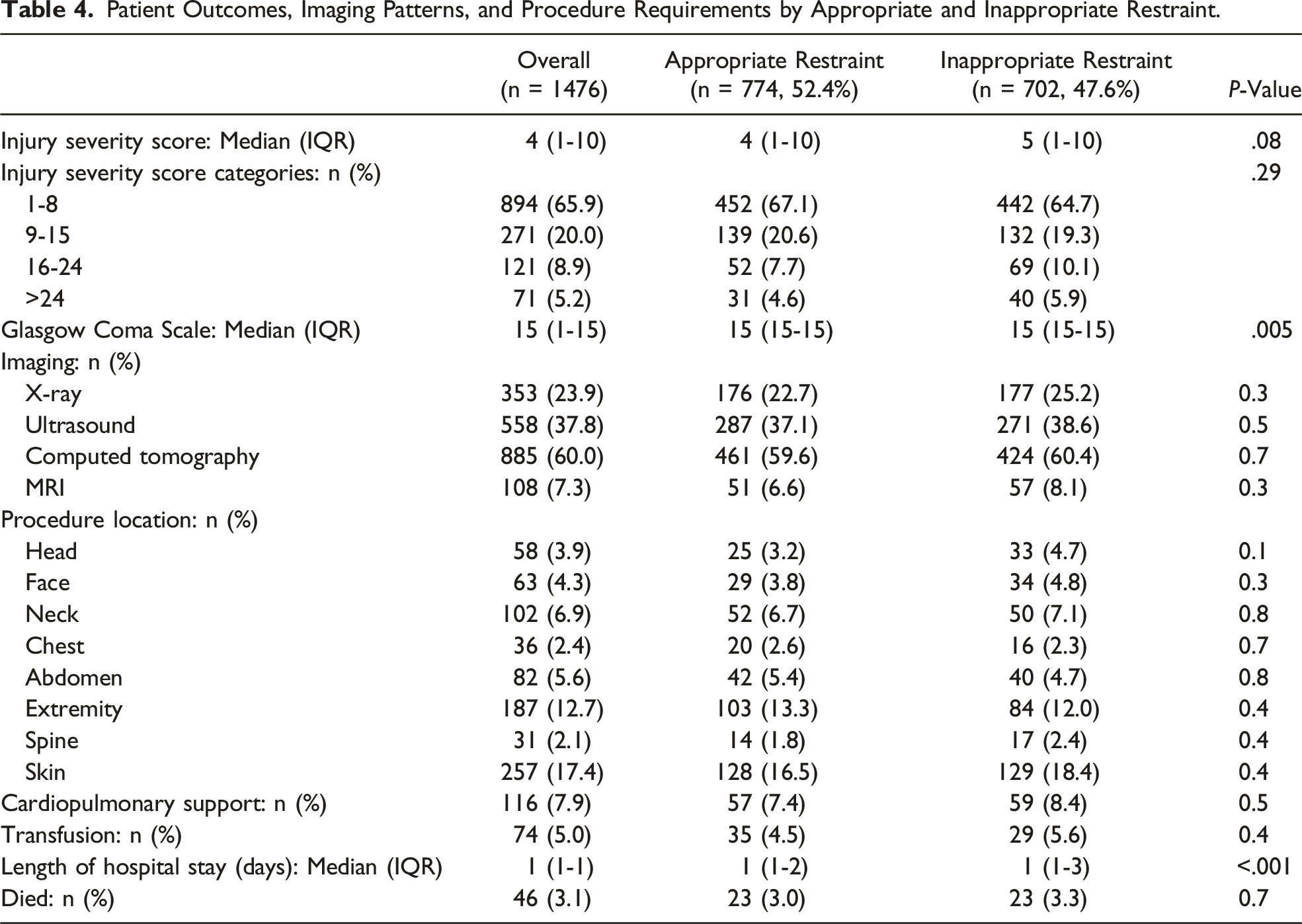
Finally, imaging patterns and procedure requirements were compared between patient groups. Overall, 353 (23.9%) children underwent at least one X-ray, 558 (37.8%) underwent an ultrasound, 885 (60.0%) underwent a CT scan, and 108 (7.3%) underwent MRI. Imaging patterns were not different between appropriately restrained and inappropriately restrained children. A similar proportion of appropriately and inappropriately restrained children underwent X-ray (n = 176, 22.7% v. n = 177, 25.2%, n = .3), ultrasound (n = 287, 37.1% v. n = 271, 38.6%, n = .5), CT scan (n = 461, 59.6% v. n = 424, 60.4%, P = .7), and MRI (n = 51, 6.6% v. n = 57, 8.1%, P = .3). Procedure requirements by location were also similar between groups. Overall, 58 (3.9%) children underwent at least one procedure for a head injury, 36 (2.4%) for chest injury, 82 (5.6%) for abdominal injury, 187 (12.7%) for extremity injury, and 31 (2.1%) for spinal injury. There was no statistically significant difference between the groups in procedures required by location (Table 4).
Discussion
This study demonstrates that only 52% of pediatric patients aged 0-8 years who presented to the emergency room following MVC were appropriately restrained. This is consistent with recently reported frequencies of restraint use among pediatric patients presenting to care following MVC.11,16 It is alarming that only 52% of patients under 8 years of age who presented to care were appropriately restrained. Inappropriate restraint of children in motor vehicles remains a significant public health issue.
In terms of patient characteristics, a lower proportion of older children and heavier children were appropriately restrained. Of the considered age cohorts, children between the ages of 4 and 8 were most likely to be inappropriately restrained. This group of children should typically be secured using a booster seat. It has been demonstrated that children of this age cohort are at particularly high risk for inappropriate restraint, and our study supports these data. 13 This finding is likely due to the underutilization of child booster seats and premature transition from booster seat to three-point restraint among this age group. The findings support that this age group continues to be an important subset of children for which targeted caretaker education is needed.
Socioeconomic factors including race, ethnicity, and insurance payor status were considered to delineate potential differences in restraint use. Regression analysis demonstrates that African American children, Asian children, and Medicaid insurance payor status patients had an increased risk of inappropriate restraint use. This study does not demonstrate increased risk of inappropriate restraint in Hispanic/Latinx children, which may dispute prior research identifying Hispanic children at increased risk for inappropriate restraint. 14
These findings are notable for a variety of reasons. Firstly, prior studies have evaluated restraint use by demographic characteristics and found African American and Hispanic children to be inappropriately restrained at higher frequencies than White children.13,14 However, only one study (Rangel et al) has controlled for payor status when determining race or ethnicity as a risk factor for inappropriate restraint. 17 This represents a significant knowledge gap regarding restraint use in children as insurance payor status may confound the effect of race on restraint use. The results of this study more thoroughly characterize these differences than prior studies. Secondly, the authors do not propose that race, ethnicity, and payor status alone explain observed differences in restraint use in children. The authors strongly suspect that there are other variables that also impact restraint use that are not included in publicly available databases. These may include household income, education level, primary language of caretaker, urban or rural residence, and access to regular pediatric well-care. Interestingly, a recently published study that interviewed women with children aged 4 to 7 used mediation analysis to determine that self-reported (caregiver) seat belt use, marital status, and education level may partially explain the effect of race on child restraint use. 18 However, these factors are yet to be systematically evaluated in large-scale observational studies. Thirdly, the findings of this study emphasize the need for further research and more robust data collection on the topic of child restraint use. The authors suggest that variables such as household income and education level of caretaker be added to trauma databases as these are unstudied variables that may impact current understanding of the impact of race and ethnicity on restraint use.
To the authors’ knowledge, this study is the first to compare imaging patterns between appropriately and inappropriately restrained children. There was no difference in proportion of children who received at least one X-ray, ultrasound, CT scan, or MRI between groups. Notably, only 24% of children received an X-ray while 60% of children received CT scan. The infrequent use of X-ray was surprising given the emphasis of X-ray as a first-line diagnostic modality in pediatric trauma algorithms, particularly for chest trauma.19,20 These findings suggest that restraint status does not impact imaging utilization in children following MVC. The authors suspect that factors such as loss of consciousness, physical exam findings, vital sign abnormalities, and overall acuity of patient (as reflected by ISS) are more likely to dictate a provider’s use of imaging in the trauma setting.
We hypothesized that appropriately retrained patients would have decreased mortality and ISS, as previous studies have demonstrated decreased mortality, ISS, and LOS with appropriate restraint use.8,9,11,14,16 However, ISS and mortality were not different between appropriately and inappropriately restrained children. Length of stay was shorter for appropriately restrained patients. In terms of ISS, most patients included in this study suffered only mild injury with a median ISS of 4. Only 6 of the 17 hospitals included were level I pediatric trauma centers, so the acuity of patients in the cohort will likely be lower than studies performed at level I trauma centers alone. It is possible that our study is underpowered to detect differences in ISS based on the appropriateness of restraint given the relatively small proportion of severely injured patients. Our study also detected no difference in mortality. A study utilizing the National Trauma Database detected no difference in mortality between appropriately and inappropriately restrained children. Their findings suggest that restraint use is most protective at the scene. 14 The data utilized for our study do not include patients who died at the scene of the accident, and thus the findings may not detect the full protective benefit of restraint use.
There are several limitations to the study. The NCTR does not report rear-facing vs forward-facing car seats but instead reports infant car seat and child car seat. Thus, patients who require a car seat (age 0 to 3.99 years or weight <40 lbs) were considered appropriately restrained if any car seat (whether infant or child car seat) was noted. It was not possible to determine if a patient was rear or forward facing, which is an important component of appropriate restraint status for young children. Although this work does expand on what is currently known regarding demographic risk factors for inappropriate restraint in children, the database did not collect certain variables which could confound findings. For example, this study does not control for household income, education level, primary language of the caretaker, urban or rural residence, and access to regular pediatric well-care. It is possible that these unmeasured variables also impact risk for inappropriate restraint in children. In addition, the study population is generated from patients presenting to the emergency department for evaluation. Thus, the findings may underestimate overall restraint use and overestimate the degree of injury severity to children involved in motor vehicle collisions. Further, it is possible that unrestrained passengers are more frequently transported to the emergency room simply because they were unrestrained and not due to their observed injuries. Finally, the study does not include patients who died at the scene of the accident and may underestimate the protective benefit of restraint use.
This study demonstrates poor compliance to established restraint guidelines for children presenting to care following MVC. African American children, Asian children, and children with Medicaid insurance are at an increased risk for inappropriate restraint. Length of hospital stay was longer for inappropriately restrained patients, but mortality was not different. There is a need for additional large-scale observational studies and bolstering of current pediatric databases to include socioeconomic variables such as household income, education level and primary language of caretaker, and access to regular pediatric well-care.
Footnotes
Acknowledgments
The authors would like to thank the North Carolina Trauma Registry (NCTR) for the use of their database, which made this project possible.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.