
Abstract
Keywords
Key Takeaways
• Radiology residents (RRs) and teleradiologists had similar discrepancy rates when interpreting pediatric trauma computed tomography (CT) imaging. • Radiology residents had a higher discrepancy rate for pediatric trauma than RR interpretations of adult CT scans, indicating more training on interpretation of pediatric trauma studies is needed.
Introduction
Computed tomography (CT) imaging serves as a critical diagnostic tool, particularly in pediatric trauma patients (PTPs), who account for nearly 9 million Emergency Department (ED) visits annually. 1 The use of CT imaging must be carefully considered due to concerns surrounding radiation exposure in pediatric populations. 2 However, CT imaging is crucial in this population to facilitate management decisions ranging from discharge to need for emergent operation. 2 Delays in CT imaging studies and/or interpretations may put children at risk of increased morbidity and mortality due to delayed diagnosis. 3
The necessity of round-the-clock radiology coverage in trauma centers caring for PTPs is well recognized, but a relative shortage of attending radiologists makes it challenging to provide continuous staff coverage. 4 Consequently, various coverage models have been adopted to address this issue, including the use of nighttime on-call radiology residents (RRs) and attending teleradiologists (ATs). However, there is a paucity of data comparing these models of overnight coverage, and institutions have to balance providing accurate, timely interpretations with radiologist availability and cost-effectiveness.4,5
A previous study involving adult patients demonstrated that RRs exhibited lower overall (7.7% vs 9.0%) and major discrepancy rates (3.8% vs 5.2%), as well as faster turnaround times (51.3 vs 78.8 minutes), than ATs. 6 However, pediatric CT interpretation is inherently more challenging due to embryological and anatomical differences, a paucity of abdominal fat, and the potential for normal variants to appear pathological.7,8 Furthermore, findings that may be similar between adult and pediatric imaging may not represent the same disease or diagnosis in children. To our knowledge, no studies have directly examined RR and AT discrepancy rates specifically for PTPs. Identifying any differences in performance could help inform staffing model decisions for trauma centers. Therefore, this study aimed to compare the accuracy of RR and AT interpretations of PTP CT scans, hypothesizing that discrepancy rates and time to interpretation would be similar between the two groups.
Methods
This study involved a retrospective analysis of PTPs presenting to a single American College of Surgeons adult level I and pediatric level II trauma center between March 2019 and May 2020. University of California Irvine Institutional Review Board approval was obtained, and a waiver of informed consent was granted. All PTPs (ages 0-17 years old) undergoing CT imaging were included. Pediatric trauma patients that did not have CT scans with both RR and AT interpretations were excluded. Evaluated CT types consisted of CT head, CT maxillofacial, CT cervical spine, CT angiogram (CTA) of the neck, CT thoracic/lumbar spine, CTA chest, CT abdomen and pelvis with intravenous contrast, and CT extremity.
An adult cohort was also analyzed in comparison to the pediatric cohort. This cohort included all adult trauma patients 18 years and older who presented to the same trauma center from March 2019 to May 2020. Only patient records containing both a resident and teleradiology CT interpretation were included.
At the study institution, on-call RRs provide imaging interpretations from 22:00 to 08:00 the following morning, with teleradiology services supplementing resident reads. Twelve postgraduate year (PGY)-3 RRs were on overnight call during the study period. Residents were physically present at the study institution for the duration of their overnight call. Upon completion of a CT scan, the technologist electronically transmitted images to both the institutional servers for RR interpretation and the teleradiology server for AT review. Radiology resident interpretations were directly uploaded to the electronic medical record, while AT interpretations were printed, scanned, and uploaded to the imaging server. Teleradiology impressions were timestamped when signed by the AT, and this timestamp was used to determine time to interpretation (not the later time when the report is uploaded to the imaging server). Notably, ATs did not have access to the RR report, but RRs could view AT interpretations if they were completed and uploaded first. Both RR and AT interpretations were accessible to the trauma team and were of comparable length. Final faculty attending radiologist reads were available the following morning.
Interpretation Scoring
Radiology resident and AT interpretations were compared with the final attending faculty interpretation and graded using the RADPEER scoring system, which is widely used for comparing imaging interpretations.9,10 Scores were assigned as follows: (1) no discrepancy; (2) discrepancy in interpretation, not ordinarily expected to be made (“understandable miss”); (3) discrepancy in interpretation, should be made most of the time. The addition of “a” indicates that the discrepancy is unlikely to be clinically significant and “b” indicates that the discrepancy is likely to be clinically significant. RADPEER scores of 2b, 3a, and 3b were considered major discrepancies, consistent with previous studies in both the adult and pediatric literature.10–13 Discrepancies were further categorized as traumatic injuries vs incidental findings and missed diagnoses vs overcalls. Traumatic injuries were defined as an injury that could have resulted from the trauma, such as intracranial hemorrhage, fractures, and solid organ injuries. Incidental findings were any diagnoses not explained by trauma, such as pulmonary nodules, thyroid nodules, and abdominal masses. Missed diagnoses were findings present on imaging but not reported by the interpreter. Overcalls were defined as diagnoses made by the interpreter that were not present in the imaging based on the final faculty attending radiologist CT interpretation.
Statistical Analysis
The primary outcome was discrepancy rate between interpreter (RR or AT) and final attending radiologist report. The secondary outcome was time to interpretation, defined as the time from imaging completion to report signing. Additional outcomes included discrepancy rates by CT type and clinical implications of overcalls. In addition, discrepancy rates of the combination of both RR and AT were collected. The combination of RR and AT interpretations was then compared with RR and AT interpretations individually. Finally, RR and AT discrepancies were each individually compared with previously studied discrepancy rates in an adult cohort by RRs and ATs, respectively, at the same institution, over the same time period. 6 Chi-square tests were used to compare categorical variables, and student’s t test was used to compare continuous variables between RR and AT interpretations. P-values <.05 were considered statistically significant. Statistical analysis was performed with IBM SPSS Statistics for Windows (version 24, IBM Corp., Armonk, NY).
Results
A total of 270 interpretations (135 RR interpretations and 135 AT interpretations) from 42 PTPs were included for analysis. The adult cohort consisted of 1053 patients with a total of 8226 interpretations (4113 RR interpretations and 4113 AT interpretations).
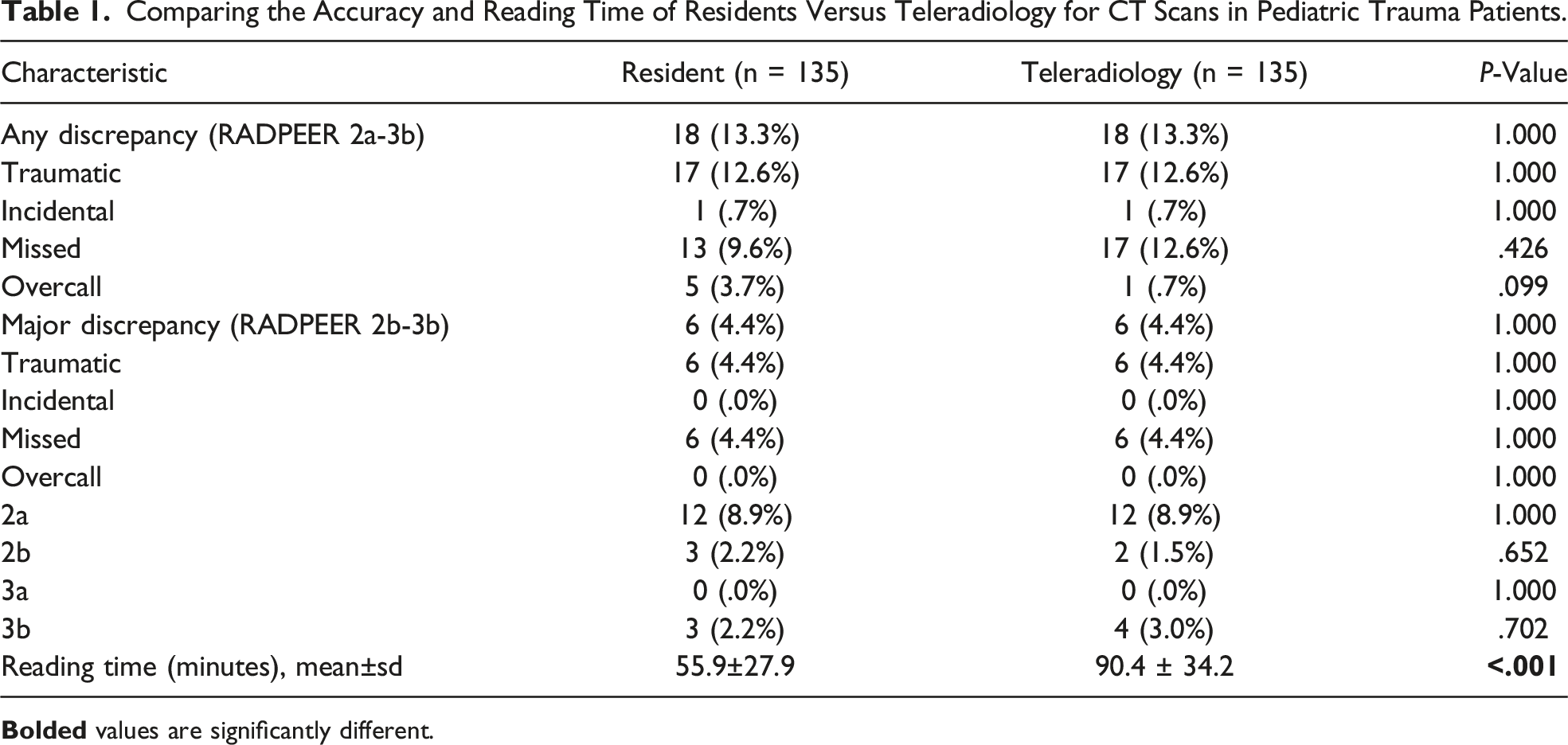
Discrepancy Rates and Time to Interpretation
Comparing the Accuracy and Reading Time of Residents Versus Teleradiology for CT Scans in Pediatric Trauma Patients.
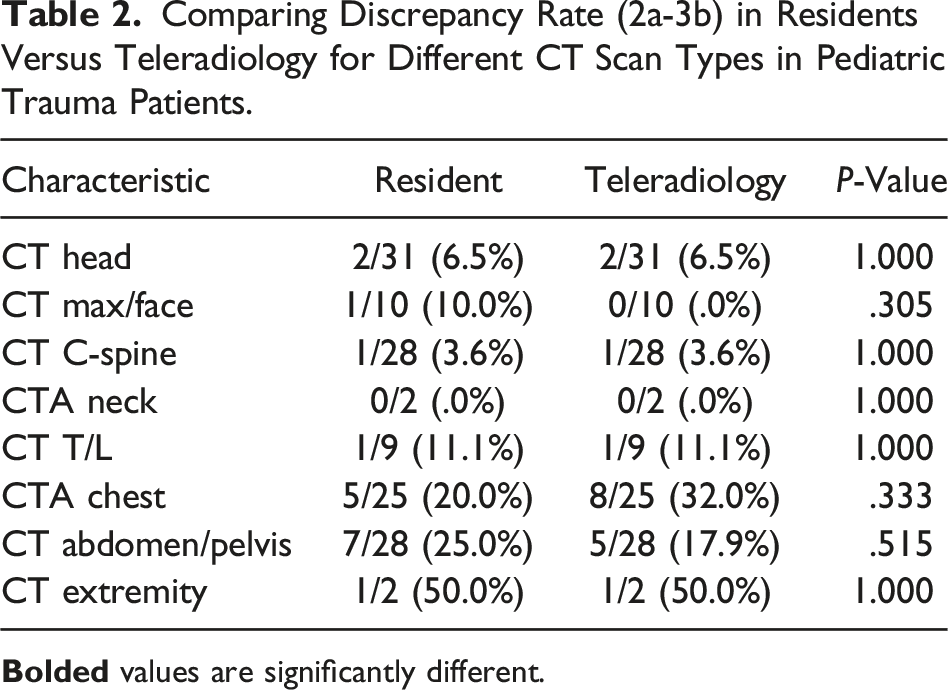
Discrepancy Rates by CT Scan Type
Comparing Discrepancy Rate (2a-3b) in Residents Versus Teleradiology for Different CT Scan Types in Pediatric Trauma Patients.
Discrepancy Rates for RRs and ATs Compared to Prior Adult Trauma Discrepancy Rates
Radiology residents had a significantly higher discrepancy rate for PTPs than adult trauma patients (13.3% vs 7.5%, P = .012). Attending teleradiologists had similar discrepancy rates for the two groups (13.3% and 8.9%, respectively, P = .077).
Discussion
Trauma remains a significant cause of morbidity and mortality in PTPs, with firearm violence and motor vehicle collisions being the first and second most common causes of life loss in children, respectively. 14 As CT imaging remains a mainstay of trauma care to diagnose clinically important injuries15,16 and given that significant trauma has a temporal relationship occurring after daytime hours, 17 overnight radiology coverage is crucial for PTPs and their care. However, pediatric trauma occurs relatively infrequently, even at most trauma centers, and there is limited data to determine the optimal radiology staffing model for accurate interpretations for PTPs. This single-center study found no difference between overall or major discrepancy rates when comparing RR and AT interpretations of CT scans for PTPs. However, RRs provided reports 35 minutes faster than ATs, though they had higher discrepancy rates than a prior adult trauma study. 6
Discrepancy rates for RRs have previously been reported in all populations to range from .3% to 10%,10,18 but these rates are not specific to PTPs. One study by Dinh et al specifically examined RR discrepancy rates in a large pediatric hospital and found major discrepancy (RADPEER 3 or 4) rates to be 1.8% for pediatric CT scans, 10 lower than our study’s rate of 4.4%. However, our study considered major discrepancies to be RADPEER scores of 2b-3b, which may account for the higher rate. Furthermore, RRs in the Dinh study were at a large standalone pediatric center and included non-trauma patients, as opposed to RRs in our study who were reading a combination of mostly adult imaging studies with only occasional pediatric imaging studies mixed in. The constant exposure to pediatric studies may account for the lower discrepancy rate in the Dinh study, but our RR major discrepancy rate is still well within reported discrepancy rates for RRs and similar to ATs.
For ATs, major discrepancy rates have been previously reported to be in the range of 1.7%-3.2% for adult patients. 19 There is limited literature regarding discrepancy rates of AT for pediatric imaging, but one study by Pfeifer et al demonstrated an overall discrepancy rate of 14.4% for all imaging studies and an actionable discrepancy rate of 1.6%. 3 This was similar to our study, which reported a 13.3% overall discrepancy rate. However, it is difficult to directly compare actionable discrepancy as reported in the Pfeifer study to our major discrepancy rate of 4.4% because the Pfeifer study did not utilize RADPEER scores. “Actionable discrepancy” was defined as a discrepancy that would change the management of the patient. 3 This may be comparable to RADPEER 2b and 3b scores, which made up the entirety of our major discrepancies for ATs.
To our knowledge, this is the first study to compare RRs and ATs discrepancies in PTPs. A previous study at this institution found that RRs had lower discrepancy rates than ATs (3.8 vs 5.2% for major discrepancies) as well as shorter time to interpretation for CT scans in adult trauma patients. 6 The reason why RRs no longer had an advantage over ATs when interpreting PTP CT imaging may be due to less experience with pediatric imaging compared to adult imaging during their initial residency training, as more pediatric training may occur beyond the third postgraduate year, which is the year the RRs in this study were. Furthermore, the combination of ATs and RRs failed to statistically improve the discrepancy rate for PTPs, unlike adult trauma patients where this combination was found to be beneficial. Future research is needed to ascertain why this may be.
Missed Injuries From Both Radiology Residents and Teleradiologists.
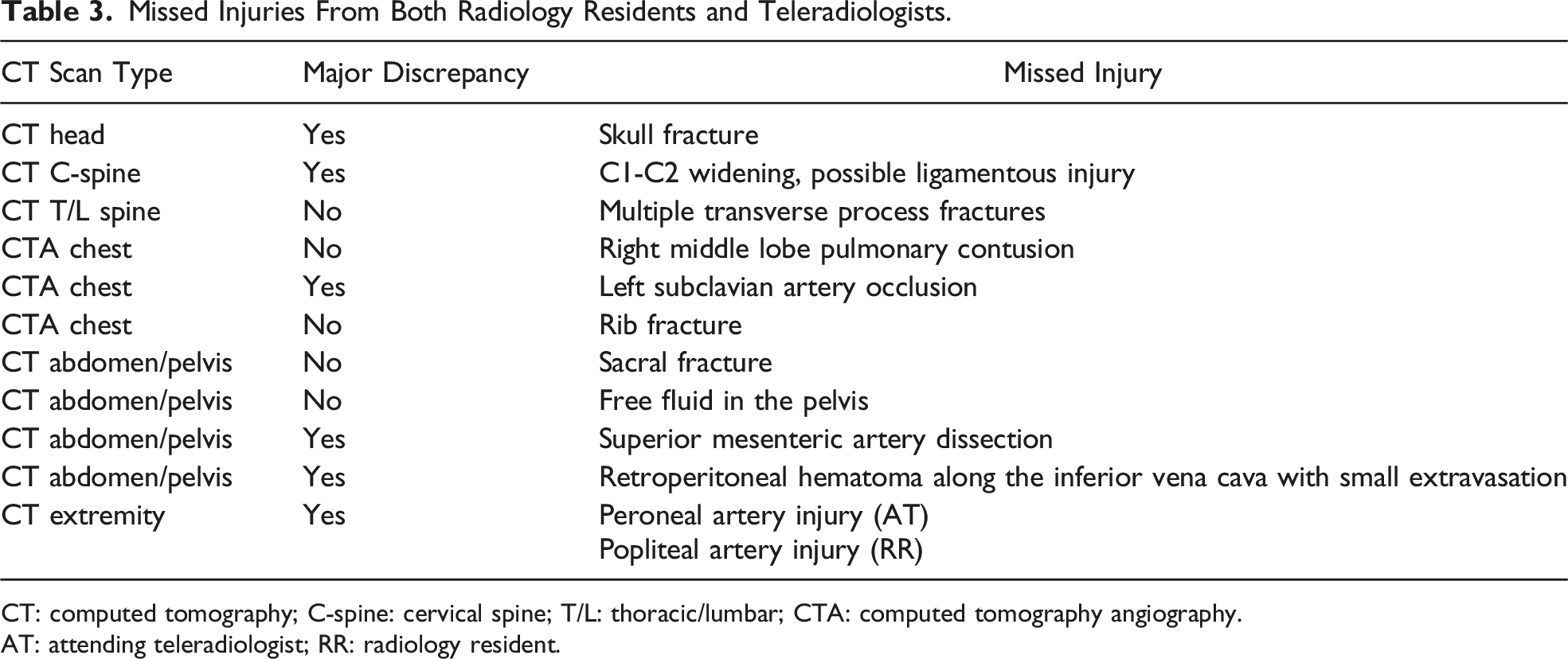
CT: computed tomography; C-spine: cervical spine; T/L: thoracic/lumbar; CTA: computed tomography angiography.
AT: attending teleradiologist; RR: radiology resident.
This study has several limitations. First, the in-house attending radiologist’s read was considered the “correct” interpretation for comparison purposes. Attending radiologists were not all specifically trained in pediatric radiology. It is therefore possible that an in-house attending read was incorrect, but this situation is unlikely as they undergo a significant peer review process by the trauma service and Department of Radiology. Second, the number of CT scans included in this study was relatively small compared to prior non-trauma pediatric studies. This is also due to increased attention toward minimizing radiation exposure for children. Also, the study does not include other imaging modalities, such as plain radiographs, ultrasound, and/or magnetic resonance imaging. Plain film radiographs were not included in this study as radiology residents do not interpret these overnight at our institution. This study was also unable to evaluate differences between RR and AT for blunt vs penetrating trauma as the rate of penetrating pediatric trauma at our center is quite low (10.8%) and many of these patients do not receive CT imaging. In addition, and as previously noted, RRs potentially had access to AT reports, which may have influenced their reads. However, AT reports were available on average 35 minutes after the RR reports were signed, decreasing the likelihood that RR reports were influenced by ATs. Only 5% (15/270) of reports were signed by AT before RR had completed their report. Furthermore, ATs might have taken longer to provide interpretations due to technical challenges, such as slower image transfer speeds. The time when reports were uploaded to the server was not available, and therefore we used the time the report was signed to determine time to interpretation. Our experience and data provided by the teleradiology service suggest that reports are available to the trauma team within approximately one minute from when the report was signed. Lastly, the results of this single-center study may not be generalizable to all radiology residency programs, teleradiology services, or standalone pediatric hospitals.
In conclusion, this study demonstrated no significant difference in overall or major discrepancy rates between RRs and ATs for CT scans of PTPs. However, ATs had longer times to interpretation, which is problematic as timely interpretations are crucial for PTPs who may have life-threatening injuries. Overall, this suggests models utilizing RRs or ATs may be reasonable, but there remains room for improvement in the accuracy of PTP CT interpretations, which may be achieved with focused continuing education on the areas of common discrepancies as outlined in this study. Finally, future multicenter studies are needed to confirm these findings and evaluate if pediatric subspecialty training provides improved accuracy to justify the expense of pediatric-trained ATs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.