
Abstract
Geriatric patients who fall are among the most common mechanisms of injury presenting to trauma centers. We sought to quantify the impact of various comorbidities on length of stay (LOS) in these patients to identify areas for intervention. A level 1 trauma center’s registry was queried for patients ≥65 years old with fall related injuries admitted with LOS greater than 2 days. Over 7 years, 3714 patients were included. Mean age was 80.9 ± 8.7 years. All patients fell from heights of 6 feet or less. Median total LOS was 5 days, interquartile range [3,8]. Overall mortality rate was 3.3%. The most common comorbidities were cardiovascular (57.1%), musculoskeletal (31.4%), and diabetes (20.8%). Multivariate linear regression modeling LOS identified diabetes, pulmonary, and psychiatric diseases associated with longer lengths of stay (P < .05). As trauma centers refine care for geriatric trauma patients, comorbidity management represents an opportunity for proactive intervention.
Geriatric patients, defined as those 65 years of age or older, represent an increasing proportion of patients presenting to trauma centers. From 2005 to 2015, there was a concurrent increase in the percentage of geriatric trauma patients presenting to trauma centers, with the average age of patients seen at trauma centers in the United States increasing from 39 to 51 years old. 1 The mortality rate associated with injury in the geriatric population is consistently higher than that of younger patients. 1 In particular, ground level falls are the highest frequency mechanisms of injury for geriatric patients presenting to trauma centers, with estimates as high as 1 in 3 geriatric persons sustaining a ground level fall each year. 2 Despite advancements in anticoagulant reversal, fall prevention programs, and inpatient resources, geriatric fall patients continue to show worse outcomes. 3
Society guidelines support the triage of injured patients greater than 65 years with comorbidities to a trauma center. 4 As the population ages and these patients are seen at trauma centers in increasing numbers, their inpatient management will be further scrutinized as a quality metric and cost burden to the healthcare system. 2 Previous work has identified age, injury severity score, and admission Glasgow Coma Scale (GCS) as significant predictors of length of stay (LOS) in trauma patients. 2 We sought to quantify the impact of various comorbidities on LOS in geriatric patients who sustain injuries from falls while controlling for these variables.
Penn State Health Trauma Registry, maintained in accordance with National Trauma Data Bank Standards, was queried for patients ≥65 years old with fall mechanisms who were admitted with LOS greater than 2 days. Statistical analysis was performed with SPSS Statistics version 28.0 (IBM, Armonk, NY, 2021). Univariate analyses were used to summarize trends and identify differences between subgroups. Multivariate linear regression was employed to control for confounders and quantify the impact of comorbidities on LOS. Significance was defined as P-value <.05. The study was approved by Penn State College of Medicine Institutional Review Board.
Between 2013 and 2019, 3714 patients met inclusion criteria. Mean age was 80.9 ± 8.7 years. The study cohort was 45% male. All patients fell from heights of 6 feet or less. There was no difference in average age when data was stratified by year. The number of patients increased each year from 281 in 2013 to 969 in 2019. Transfers from referring facilities represented 1162 (31.2%) of the cohort. Median admission GCS was 15. Mean Injury Severity Score (ISS) was 12.2 ± 7.6. One hundred seventy patients (4.6%) required operative intervention following resuscitation. Median total LOS was 5 days, interquartile range (IQR) [3,8] for all patients. Just under one-third of patients, 1118 (30.1%), spent time in the intensive care unit (ICU), with median ICU LOS 2 days, IQR.1,3 Of these, 234 (6.3%) required ventilatory support, using a median of 3 ventilator days, IQR [1,7]. The overall mortality rate was 3.3% for the study period.
Multivariate Linear Regression of Length of Stay for Geriatric Patients with Fall Related Injuries.
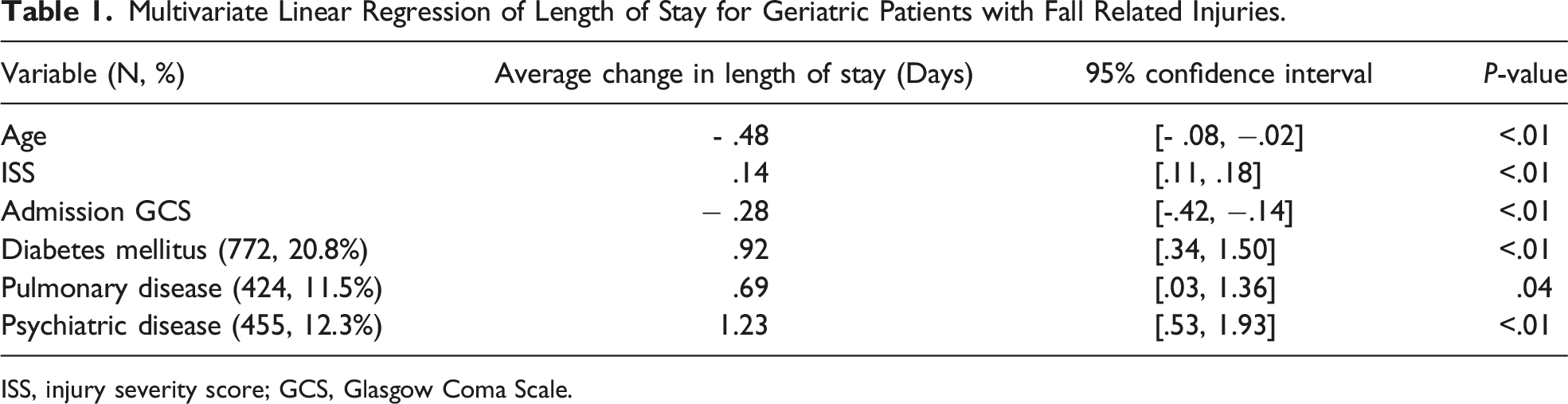
ISS, injury severity score; GCS, Glasgow Coma Scale.
Trauma surgery admitted 1600 (43.1%) patients, with non-surgical services admitting 1265 (34.1%), and other surgical services admitting 849 (22.8%). Patients admitted to trauma surgery had a higher number of comorbidities, median of 3, IQR [2,5], compared to 2, IQR1,4 on other surgical services and 0, IQR [0,3] on non-surgical services (Kruskal-Wallis, P < .01). The median length of stay by service was the same at 5 days, but interquartile range for patients admitted to trauma surgery was significantly larger than that of non-surgical or other surgical services (6 vs 4 vs 4, respectively, Kruskal-Wallis, P < .01). Patients admitted to trauma surgery were also more likely to require at least 1 day in the ICU (900, 56.3%), compared to non-surgical services (50, 4.0%), or other surgical services (168 19.8%), (P<.01).
This report characterizes the significant impact comorbidities play on LOS in geriatric patients who sustain injuries from falls over a 7-year period at a single level 1 trauma center. The average age did not change during the study period, despite the increasing number of patients per year and over 70% of patients having at least 1 comorbidity. While cardiovascular and musculoskeletal diseases were the most common, diabetes, pulmonary, and psychiatric diseases significantly impacted the length of stay in geriatric patients. These comorbidities are particularly exacerbated by injury and often worsen in the post-injury inflammatory state. Psychiatric disease added the most days on average, consistent with previous work supporting dementia and delirium as significant contributors to increased length of stay for geriatric patients.1,2
Most patients in the study cohort were admitted to the trauma surgery service, with more than half of those patients admitted to the ICU for at least 1 day. This reflects underlying practice patterns including a trauma surgeon run surgical ICU that can admit patients directly from the trauma bay, as well as ICU-protocol driven management of common injuries, such as rib fractures or pelvic fractures. For patients with numerous comorbidities, the ICU setting also allowed for resuscitation in the context of stabilization of comorbidities. Crucially, ICU use is associated with higher rates of delirium, which increases overall LOS based on the regression analysis that was performed to model length of stay in this population.
This analysis provides momentum for the incorporation of additional resources for geriatric patients, including geriatricians, early social work involvement, and simultaneous comorbidity optimization in addition to acute care for injuries. As trauma center services are further refined to treat geriatric trauma patients, comorbidity management represents an opportunity for proactive intervention and more efficient disposition planning. Future directions include further integration of comorbidity management into trauma services and geriatric trauma programs, optimization of discharge planning and reimbursement through enhanced understanding of contributors to length of stay, and multi-disciplinary collaboration for comorbidity management in the injured patient.
Footnotes
Author Note
This paper was presented at the Annual Meeting of the Southeastern Surgical Congress in Savannah, GA on February 14, 2023.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.