
Abstract
Introduction
Insurance status (IS) is known to be associated with length of stay (LOS). The impact of IS on excess LOS (ELOS), days between medical readiness and discharge date, has not been explored.
Methods
We conducted a retrospective study of patients with pelvic fractures at a level I trauma center. Outcomes included ELOS (primary), discharge disposition (secondary), and ELOS-associated complications (secondary).
Results
185 patients were included. Uninsured patients were the youngest and had the least baseline comorbidities (31.3 years (median), Charlson Comorbidity Index (CCI) .1) while publicly insured patients were the oldest and had the most baseline comorbidities (58.4 years (median), CCI 2.32). Excess LOS and associated complications did not differ among groups. After regression analysis, UIPs had longer LOS than PRPs (2.07 days, 95% CI .28-3.85). UIPs were recommended to go to inpatient rehabilitation 51.6% of the time but were discharged home 93.6% of the time; 81.0% of these changes were attributed to insufficient financial resources.
Conclusions
Excess LOS and complications associated with ELOS were not associated with IS. Although UIPs were younger and had fewer baseline comorbidities, they had longer LOS after regression analysis. While discharge recommendations differed based on insurance status, UIPs had limited access to rehabilitation due to financial disparities. Despite initial treatment team recommendations, UIPs had to be sent home as their lack of insurance precluded inpatient rehabilitation placement.
Key Takeaways
Excess length of stay, the days between “medical readiness” and discharge, were not associated with insurance status. Although uninsured patients were the youngest and had the least baseline comorbidities, they had the longest length of stay after regression analysis. Uninsured patients with pelvic fractures were recommended to go to inpatient rehabilitation facilities 51.6% of the time but went home 93.6% of the time with 81% of these changes being attributed to insufficient financial resources.
Introduction
Insurance status (IS) is known to impact the delivery of health care in the United States in innumerable ways, including its effects on length of stay (LOS). Prior studies in burn and trauma have demonstrated that uninsured patients with similar injuries often have shorter lengths of stay compared to privately and publicly insured patients, with publicly insured patients frequently experiencing the longest LOS.1,2 While data exists characterizing the relationship of LOS with IS, excess length of stay (ELOS), defined as time spent in the hospital after a patient is deemed medically ready for discharge, has not been explored and there is insufficient data characterizing the impact of IS on discharge disposition in trauma patients.
Many factors can delay discharge, causing ELOS in trauma patients. From difficulty with placement in rehabilitation facilities to the lack of a safe discharge plan, many patients spend excess days in the hospital following a traumatic injury. Longer length of stay has been associated with increased incidence of health care-associated complications by 5% per additional day spent in the hospital. 3 Complications such as catheter-associated urinary tract infections (CAUTIs) and hospital-acquired pneumonia (PNA) increase hospital costs, with a CAUTI contributing $4,694-$29,743 excess costs to an already costly hospitalization. 4 The complications increase patient morbidity and mortality, and, as such, these delays in discharge are not benign but pose a significant risk to our patients while placing unnecessary strain on the health care system.
The purpose of this study is to examine the association between insurance status and excess length of stay in adult patients with pelvic fractures. We hypothesized that insurance status is associated with excess length of stay and that patients without insurance will experience complications related to their excess length of stay.
Methods
IRB Approval
This study was evaluated by the institutional review board and approved (IRB # 220825).
Study Design
We performed a retrospective observational cohort study analyzing the relationships between insurance status and length of stay in adult trauma patients with pelvic fractures at a level I trauma center. Adult patients who were admitted to our academic level 1 trauma center between January 1, 2017, and December 31, 2021, were included. Patients who were pregnant, incarcerated, died, or tested positive for COVID-19 during their admission were excluded.
Patients were classified as privately insured (PRPs), including private insurance and worker’s compensation, publicly insured (PUPs), including Medicaid, Medicare, and other governmental insurance, and uninsured (UIPs), determined by the coverage status at the end of the hospitalization. Length of stay was calculated from emergency department arrival date to discharge date. Excess LOS was determined by comparing the discharge date to the time the patient was deemed to be medically ready by the case manager’s notes. This data was corroborated with cross-reference to a plateau in charges from financial data. Medical readiness was determined based on clinical factors, including but not limited to oxygen requirement, recency of last bowel movement, and need for restraints. Distance from the hospital was determined from the center point of the injury zip code to the hospital. Median household income was determined from 2019 US Census Bureau data. Complications analyzed included falls, urinary tract infections, bloodstream infections, pneumonia, delirium, thrombosis, and thromboembolism and the need for restraints. Additional data included the Charlson Comorbidity Index (CCI), number of ICU days, zip code, injury severity score (ISS), mechanism of injury, time and date of initial operation, and complications occurring after medical readiness. The primary outcome of this study was ELOS. Secondary outcomes included discharge disposition and ELOS-associated complications.
Statistical Analysis
Analysis was performed using STATA 15 (StataCorp. 2017. Stata Statistical Software: Release 15. College Station, TX: StataCorp LLC). Univariate analysis was performed with chi-squared and t test for categorical and continuous data, respectively. Multivariable linear regression was performed, controlling for variables that had a clinically significant difference in univariate analysis.
Results
Demographic Data.
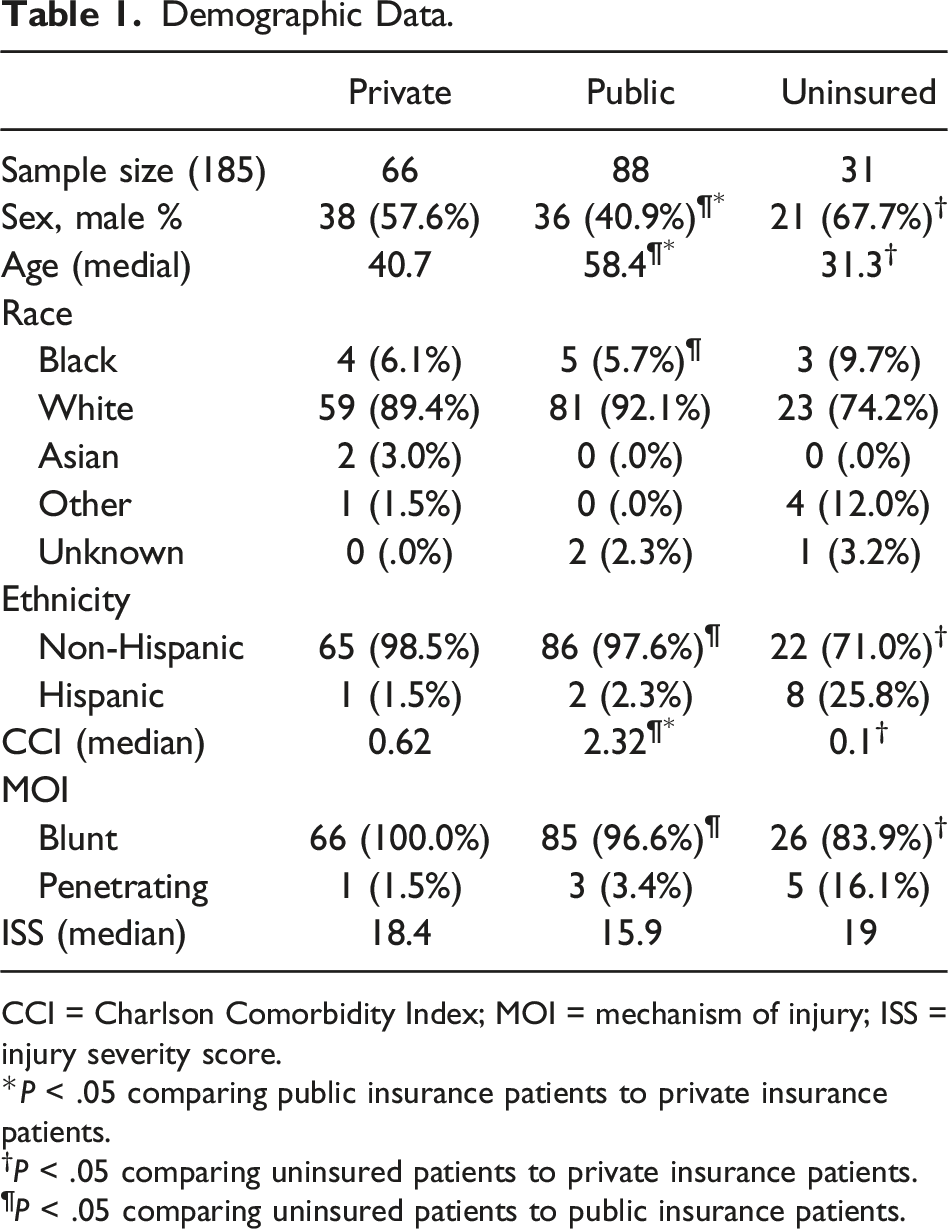
CCI = Charlson Comorbidity Index; MOI = mechanism of injury; ISS = injury severity score.
*P < .05 comparing public insurance patients to private insurance patients.
†P < .05 comparing uninsured patients to private insurance patients.
¶P < .05 comparing uninsured patients to public insurance patients.
Results.
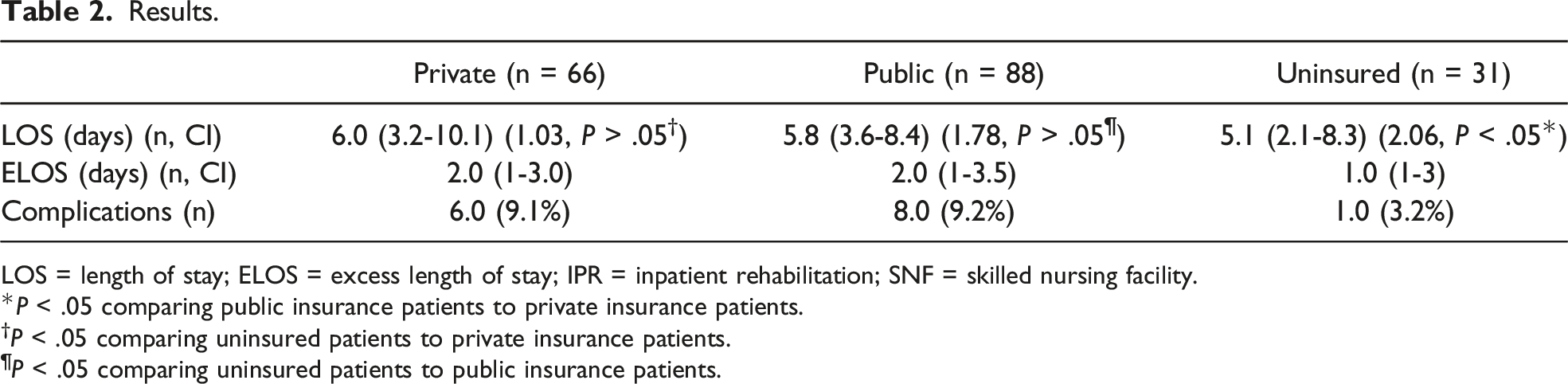
LOS = length of stay; ELOS = excess length of stay; IPR = inpatient rehabilitation; SNF = skilled nursing facility.
*P < .05 comparing public insurance patients to private insurance patients.
†P < .05 comparing uninsured patients to private insurance patients.
¶P < .05 comparing uninsured patients to public insurance patients.
Discussion
Neither ELOS nor ELOS-associated complications were impacted by insurance status. In contrast with prior data reporting that UIPs often have the shortest LOS, we found that UIPs, despite being the youngest with the fewest baseline comorbidities, had longer LOS by 2 days after regression analysis. The reasons for this longer LOS are likely multifactorial, and we hypothesize that limited baseline access to health care and the anticipation of difficult discharge may influence when patients are deemed to be medically ready for discharge. Further, UIPs had limited access to rehabilitation centers for similarly severe pelvic fractures. Despite being recommended to go to rehabilitation facilities more than half of the time, few patients were able to be discharged to one, and most of these changes in discharge location were due to insufficient funding. The sequelae of insufficiently rehabilitated pelvic fractures are predictable: disability, loss of income, chronic pain, and resulting substance use disorders, and all have the potential to plague patients who need but cannot afford rehabilitation.
There are several limitations to this study. As this is a retrospective study, we are limited by the information that is available to us in the EHR, complicating our ability to define medical readiness in a standardized way. We controlled for the variations in clinical judgment by cross-referencing documented medical ready time with a plateau in charges. Further, socioeconomic factors beyond insurance status impact discharge decisions and capabilities—insecure housing, rurality of home location, distance from the hospital, and the presence of stairs in one’s home can complicate discharge. Another limitation is that our study period included the COVID-19 pandemic, and while we excluded patients diagnosed with COVID-19 during their hospital admission, the pandemic placed a strain on the health care system that may likely have affected the disposition of the patients in our study. Finally, our sample size is limited due to the number of qualifying patients with pelvic fractures.
We conclude that ELOS is not impacted by insurance status but that the criteria for medical readiness, a subjective measure, may lengthen LOS for UIPs, a patient population with limited access to health care, including indicated rehabilitation, after leaving the hospital. We look forward to future studies identifying the health care costs associated with insufficiently rehabilitated pelvic fractures, promoting investment into rehabilitation for underinsured patients and movements to forge social programs to offset the inequities of resources for traumatic injuries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.