
Abstract
The addition of trauma to burn injuries may result in higher morbidity and mortality. The purpose of this study was to evaluate the outcomes of pediatric patients with a combination of burn and trauma injuries, and included all pediatric Burn only, Trauma only, and combined Burn-Trauma patients admitted between 2011 and 2020. Mean length of stay, ICU length of stay, and ventilator days were highest for the Burn-Trauma group. The odds of mortality were almost 13 times higher for the Burn-Trauma group when compared to the Burn only group (P = .1299). After using inverse probability of treatment weighting, the odds of mortality were almost 10 times higher for the Burn-Trauma group in comparison to the Burn only group (P < .0066). Thus, the addition of trauma to burn injuries was associated with increased odds of mortality, as well as longer ICU and overall hospital length of stay in this patient population.
Keywords
The addition of trauma to burn injuries can have a synergistic effect, which may result in higher morbidity and mortality. 1 In 2017, more than 84 000 children under the age of 14 were treated for burns in the United States. 2 The association of burn injury with additional major non-thermal injury is uncommon. The prevalence of combined burn-trauma in the general population has been reported to be from .4% to 5.8%. 3 The purpose of this study was to determine the outcomes of pediatric patients who were admitted to our facility with a combination of burn injuries and other trauma.
This was a single-site, retrospective review using our institutional Burn Center and Trauma registries. The study was approved by our Institutional Review Board (IRB) with a waiver of informed consent (IRB # 20-2331). All statistical analyses were completed using SAS version 9.4 (SAS Inc., Cary, NC). Statistical significance was accepted at P < .05. All Burn only, Trauma only, and combined Burn-Trauma patients younger than 18 years admitted between July 1, 2011 and June 30, 2020 were included. There were 3931 Burn only, 3045 Trauma only, and 28 combined Burn-Trauma pediatric patients in this study. Variables of interest included age, sex, length of stay (LOS), Injury Severity Score (ISS), revised Baux (R-Baux) score, total body surface area (TBSA), inhalation history, intensive care unit length of stay (ICU LOS), and ventilation days. The primary outcome assessed was mortality, while secondary outcomes included number of ventilation days, LOS, and ICU LOS.
We used means and frequencies to describe our study participants. Kruskal–Wallis and Chi-square tests were used to assess any group differences in demographic and clinical characteristics. In addition, we performed two types of outcomes analyses. The first analysis compared non-normalized data between the study groups using multivariate logistic regression models. The goal of this analysis was to assess associations between confounders and outcomes. Of note, due to a low number of observations, mortality estimates were based on unadjusted regression models. To make groups more comparable, we then used a multinomial logistic regression model to generate inverse probability of treatment weighting (IPTW). In this model, the outcome of interest was the analytic group (ie, Burn only, Trauma only, and combined Burn-Trauma) and the independent variables included age, sex, and race/ethnicity. IPTW was included in the final outcomes analysis where we used it to adjust the estimates of odds ratios, relative risks, their 95% confidence intervals (CI), and P-values. The results reported include unweighted and weighted estimates, but conclusions are based on the weighted estimates from the final outcomes models.
Demographics, Clinical Characteristics, and Outcomes Measures for All Patients (n = 7004).
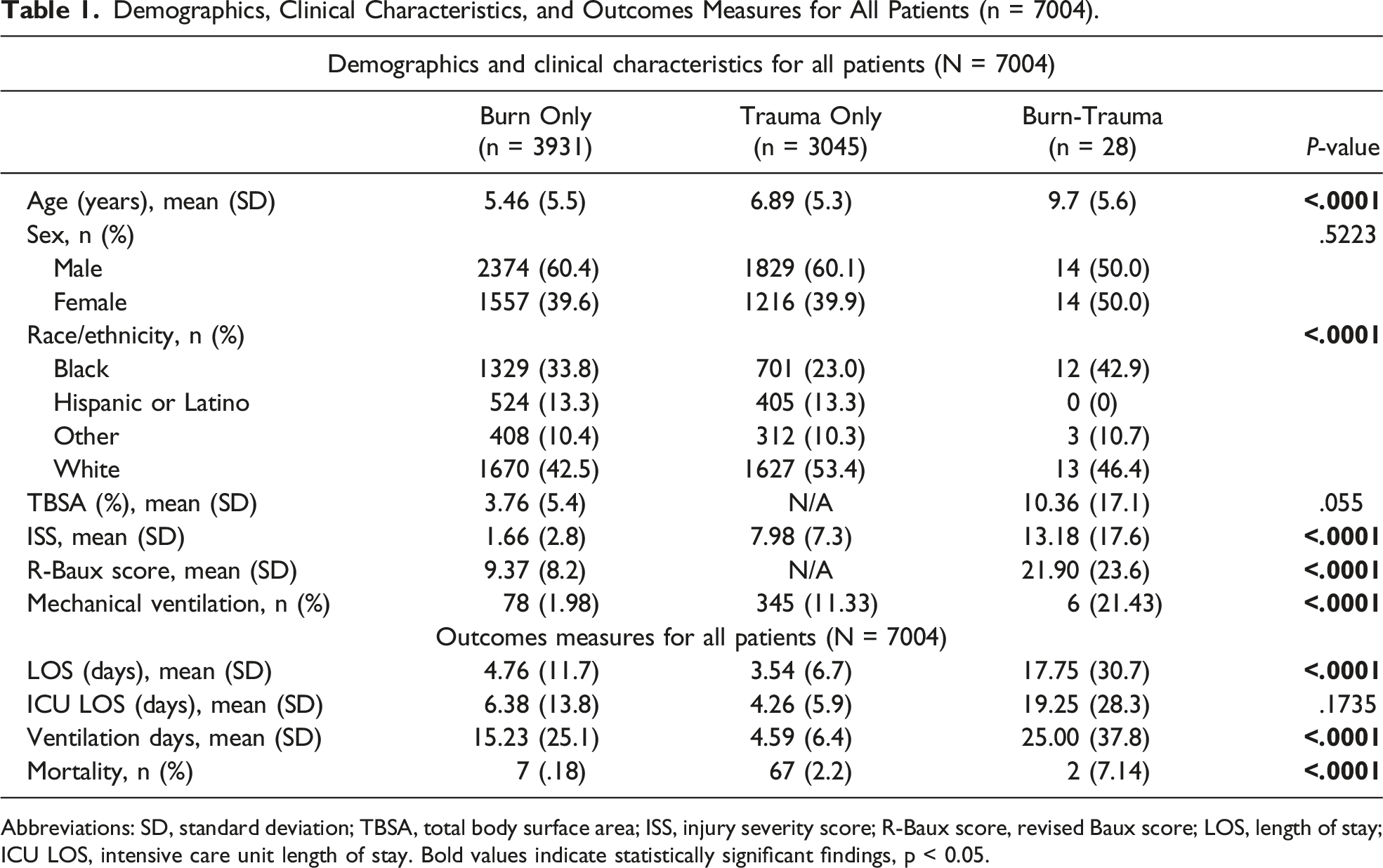
Abbreviations: SD, standard deviation; TBSA, total body surface area; ISS, injury severity score; R-Baux score, revised Baux score; LOS, length of stay; ICU LOS, intensive care unit length of stay. Bold values indicate statistically significant findings, p < 0.05.
The mean TBSA involvement for the Burn only group was 3.76% ± 5.4% and 10.36% ± 17.1% for the combined Burn-Trauma group. The mean R-Baux score for the Burn only group was 9.37 ± 8.2 and 21.9 ± 23.6 for the combined Burn-Trauma group. The mean ISS was 1.66 ± 2.8 for the Burn only group, 7.98 ± 7.3 for the Trauma only group, and 13.18 ± 17.6 for the combined Burn-Trauma group (Table 1). Inhalation injury was present in .97% (n = 38) of Burn only patients and 10.7% (n = 3) of combined Burn-Trauma patients. The overall hospital mortality was .18% (n = 7) in the Burn only group, 2.2% (n = 67) in Trauma only group, and 7.14% (n = 2) in the combined Burn-Trauma group (Table 1). Of note, all the deceased patients in the Burn only and combined Burn-Trauma groups had inhalation injury.
Table 1 also details additional patient outcomes. Patients in the combined Burn-Trauma group had longer LOS (17.75 days vs 4.76 for Burn only and 3.54 for Trauma only, P < .0001) and more days on mechanical ventilation (25.00 days vs 15.23 for Burn only and 4.59 for Trauma only, P < .0001). Patients in the combined Burn-Trauma group also had longer ICU LOS (19.25 days vs 6.38 in Burn only and 4.26 in Trauma only, P = .1735), although this was not statistically significant.
Multivariate Estimates From Unadjusted Regression Models and IPTW.
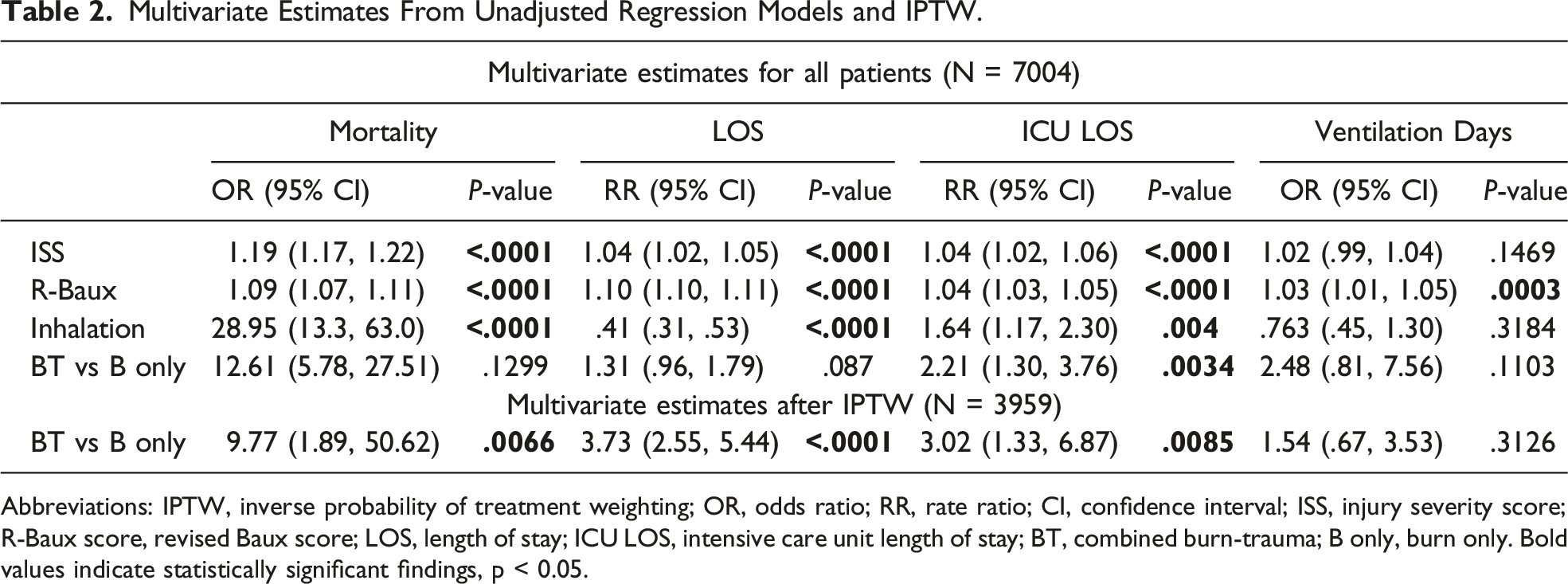
Abbreviations: IPTW, inverse probability of treatment weighting; OR, odds ratio; RR, rate ratio; CI, confidence interval; ISS, injury severity score; R-Baux score, revised Baux score; LOS, length of stay; ICU LOS, intensive care unit length of stay; BT, combined burn-trauma; B only, burn only. Bold values indicate statistically significant findings, p < 0.05.
Burns represent one of the main causes of increased morbidity and mortality in children both in the United States and worldwide. 3 The addition of burn injuries to other major non-thermal injuries is uncommon, but when it does occur, it may result in worse patient outcomes. 1 In our study, we evaluated whether the addition of other traumatic injuries to existing burn injuries would result in prolonged LOS and ICU LOS, as well as increased number of ventilation days and increased mortality. Among the study groups, those included in the combined Burn-Trauma group were found to have longer LOS and more ventilation days. Overall ICU LOS was also prolonged in the combined Burn-Trauma group; however, this finding was not statistically significant. When comparing patients in the combined Burn-Trauma group to those in the Burn only group, our study demonstrated higher odds of mortality; however, these results were significantly limited by the small number of patients available for the comparison. Therefore, we cannot conclude with certainty that the addition of other trauma to burn injuries will result in higher odds of mortality. A similar study published by Krasnoff et al demonstrated increased LOS among trauma patients with concurrent burn injuries, but no increase in mortality. They also did not find any difference in ICU LOS, ventilator days, complications, or disposition between pediatric burn-trauma and trauma only patients. 4 One interesting finding in our study, however, was that all the deceased patients in the Burn only and combined Burn-Trauma groups had inhalation injury. Therefore, it is imperative to point out that the addition of inhalation injury to other burn or traumatic injuries did result in worse outcomes for our study population. These findings highlight the continued need for future collaborative research, which can help identify best practices and ultimately improve outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.