
Abstract
Background
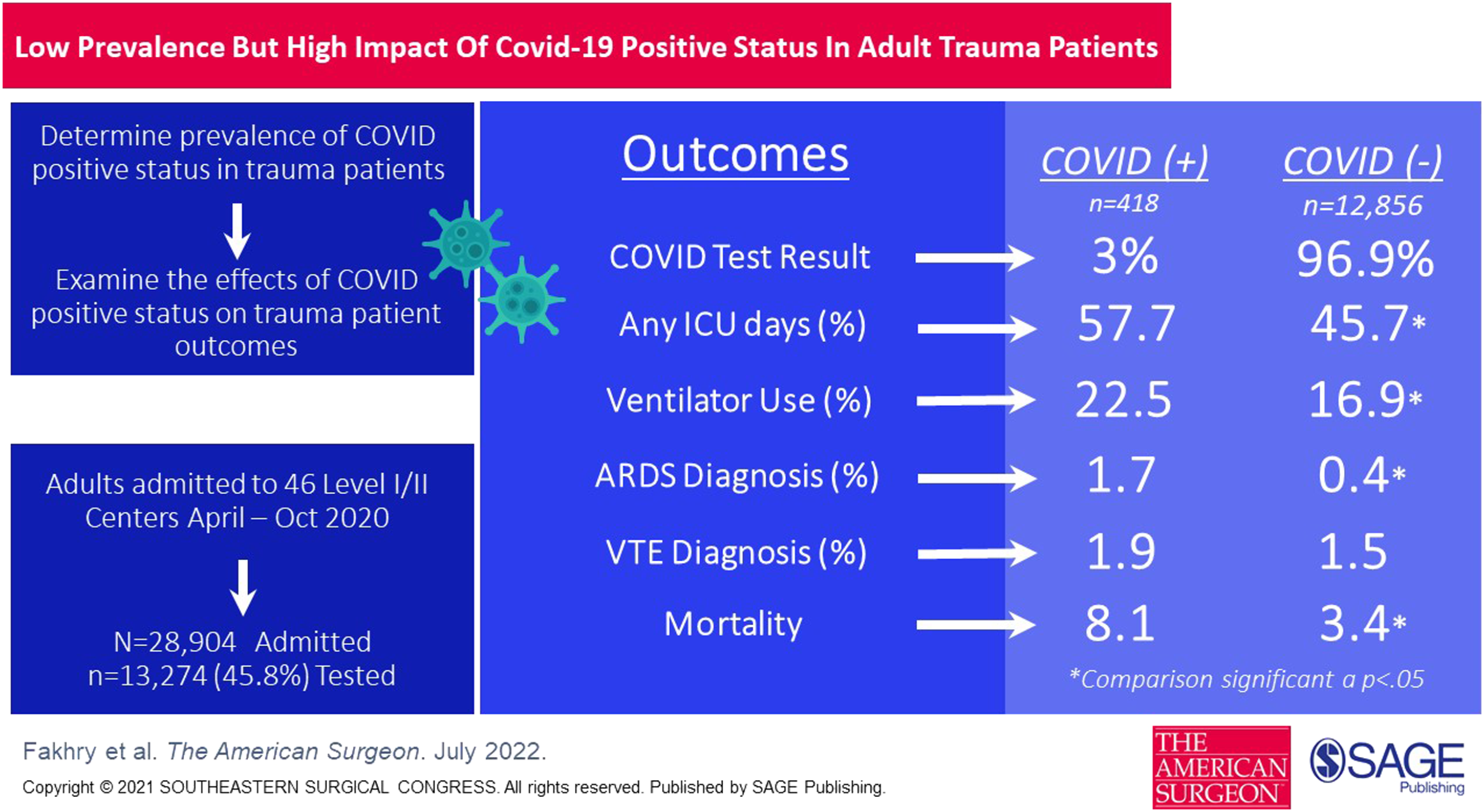
Few large investigations have addressed the prevalence of COVID-19 infection among trauma patients and impact on providers. The purpose of this study was to quantify the prevalence of COVID-19 infection among trauma patients by timing of diagnosis, assess nosocomial exposure risk, and evaluate the impact of COVID-19 positive status on morbidity and mortality.
Methods
Registry data from adults admitted 4/1/2020-10/31/2020 from 46 level I/II trauma centers were grouped by: timing of first positive status (Day 1, Day 2-6, or Day ≥ 7); overall Positive/Negative status; or Unknown if test results were unavailable. Groups were compared on outcomes (Trauma Quality Improvement Program complications) and mortality using univariate analysis and adjusted logistic regression.
Results
There were 28 904 patients (60.7% male, mean age: 56.4, mean injury severity score: 10.5). Of 13 274 (46%) patients with known COVID-19 status, 266 (2%) were Positive Day 1, 119 (1%) Days 2-6, 33 (.2%) Day ≥ 7, and 12 856 (97%) tested Negative. COVID-19 Positive patients had significantly worse outcomes compared to Negative; unadjusted comparisons showed longer hospital length of stay (10.98 vs 7.47;P < .05), higher rates of intensive care unit (57.7% vs 45.7%; P < .05) and ventilation use (22.5% vs 16.9%; P < .05). Adjusted comparisons showed higher rates of acute respiratory distress syndrome (1.7% vs .4%; P < .05) and death (8.1% vs 3.4%; P < .05).
Conclusions
This multicenter study conducted during the early pandemic period revealed few trauma patients tested COVID-19 positive, suggesting relatively low exposure risk to care providers. COVID-19 positive status was associated with significantly higher mortality and specific morbidity. Further analysis is needed with consideration for care guidelines specific to COVID-19 positive trauma patients as the pandemic continues.
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.