
Abstract
Laparoscopic sleeve gastrectomy (LSG) is an effective weight-loss operation. Portomesenteric vein thrombosis (PMVT) is an important complication of LSG. We identified four cases of PMVT after LSG at our institution in women aged 36-47 with BMIs ranging from 44-48 kg/m2. All presented 8-19 days postoperatively. Common symptoms were nausea, vomiting, and abdominal pain. Thrombotic risk factors were previous deep vein thrombosis and oral contraceptive use. Management included therapeutic anti-coagulation, directed thrombolysis, and surgery. Complications were readmission, bowel resection, and bleeding. Discharge recommendations ranged from 3-6 months of anticoagulation using various anticoagulants. No consensus was reached on post-treatment hypercoagulable work up or imaging. All cases required multi-disciplinary approach with Surgery, Interventional Radiology, and Hematology. As PMVT is a rare but potentially morbid complication of LSG, further development of tools that quantify preoperative thrombotic risk and clear guidance regarding use of anticoagulants are needed for prevention and treatment of PMVT following LSG.
Introduction
Obesity in the United States is increasing, and nearly half of adults may be obese by 2030. 1 Laparoscopic sleeve gastrectomy (LSG) is an effective long-term weight-loss strategy that reduces obesity-related comorbidities. 2
While LSG improves quality of life, portomesenteric vein thrombosis (PMVT) is a complication of LSG that may be associated with significant morbidity. PMVT is defined as partial or complete occlusion of the portal and/or mesenteric veins. The incidence of PMVT following LSG is .3-1%. 2 Risk factors for post-LSG PMVT include venous stasis from increased intra-abdominal pressure during pneumoperitoneum, manipulation of splanchnic vessels, patient hypercoagulability due to obesity and associated metabolic syndromes, and oral contraceptive pill (OCP) use.2,3 PMVT can have serious consequences, including ascites, esophageal varices, gastroesophageal bleeding and bowel infarction. 3 Because of the morbidity associated with post-LSG PMVT, bariatric surgeons must consider this complication for patients not progressing as expected postoperatively to facilitate early, directed care. Extended postoperative venous thromboprophylaxis has been proposed to help reduce the risk of post-LSG PMVT, yet it is not currently the standard of care for patients with no other indications for such therapy. Herein, we detail our experience with four cases of post-LSG PMVT with emphasis on the multi-disciplinary approach to the diagnosis and treatment of these patients.
Methods
We conducted a chart review of all PMVT cases after LSG at the University of North Carolina from 2016 to 2020. All cases were discussed retrospectively by an interprofessional team from bariatric surgery, hematology, and interventional radiology (IR).
Results
Case characteristics.
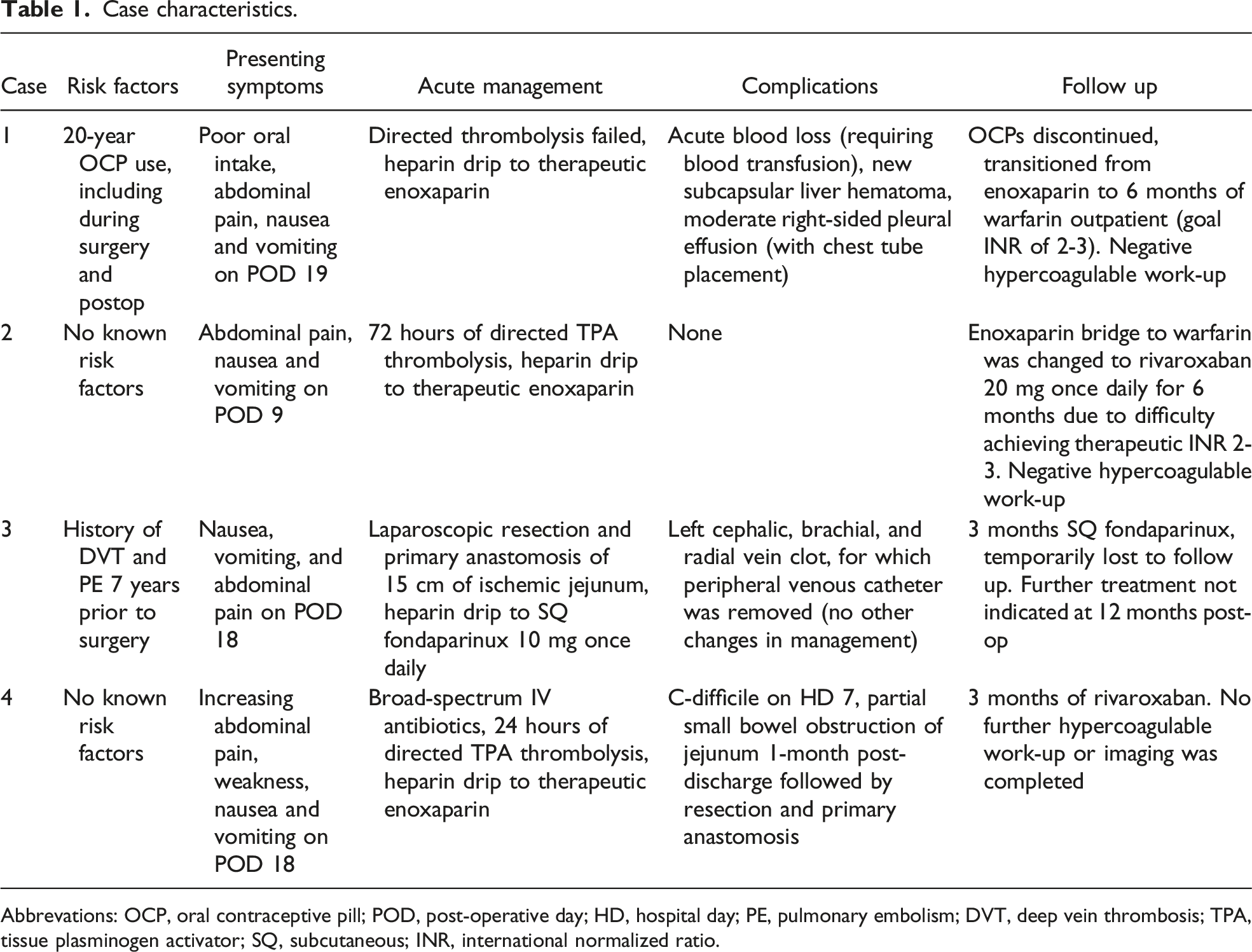
Abbrevations: OCP, oral contraceptive pill; POD, post-operative day; HD, hospital day; PE, pulmonary embolism; DVT, deep vein thrombosis; TPA, tissue plasminogen activator; SQ, subcutaneous; INR, international normalized ratio.
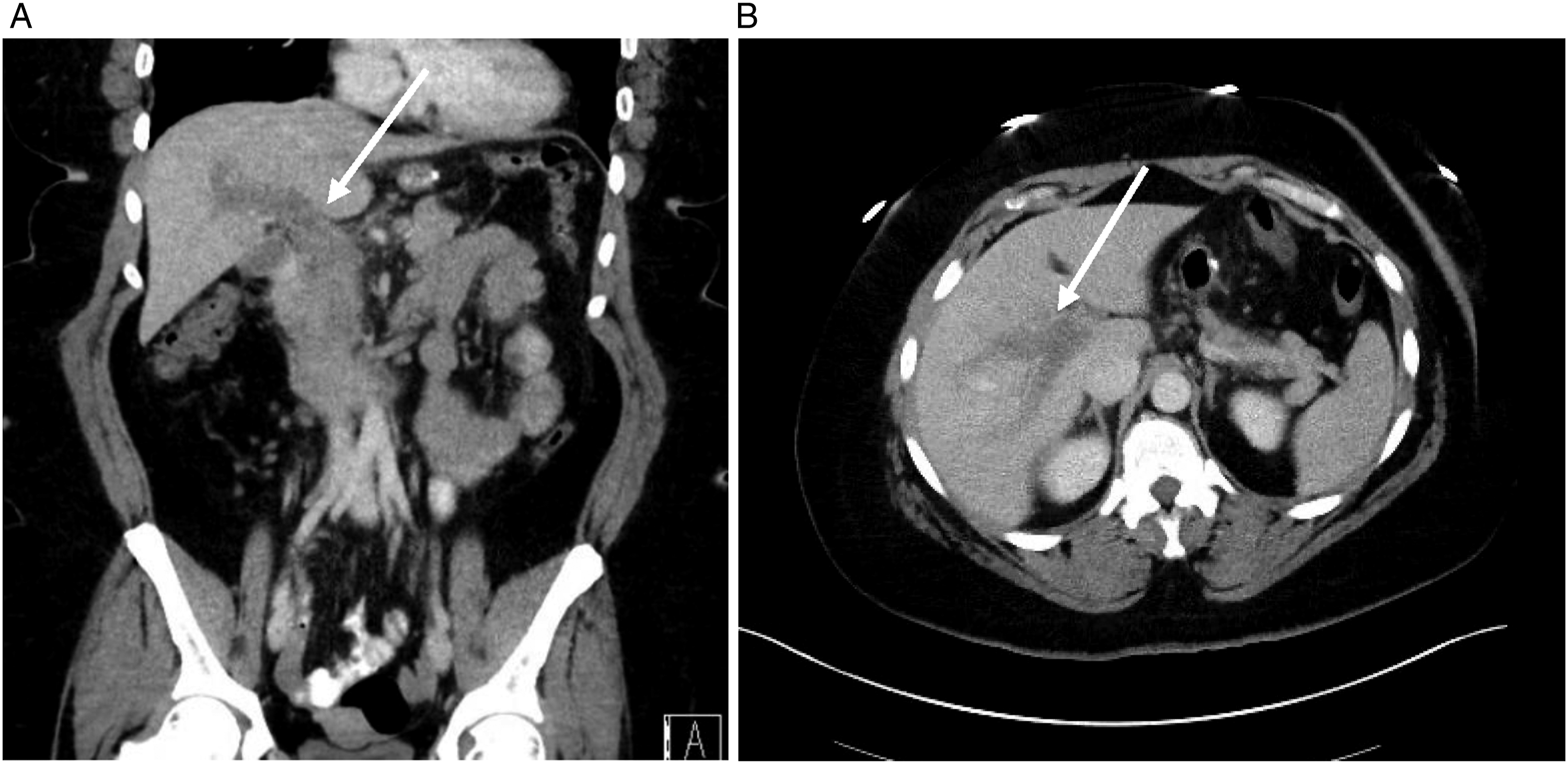
Example of coronal (A) and axial (B) CT imaging with contrast depicting PMVT demonstrated in Case 2 (arrows). PMVT, portomesenteric vein thrombosis; CT, Computed tomography.
Discussion
Overby et al found that patients undergoing bariatric surgery have significantly higher rates of both acquired and inherited thrombophilias relative to the general population. 4 Due to cost and lack of evidence-based guidelines, preoperative thrombophilia testing is not routinely recommended. However, preoperative focus on modifiable risk factors for patients undergoing bariatric surgery is warranted, such as timely discontinuation (several weeks before surgery) of estrogen-containing contraceptives. Additionally, the risk-benefit ratio of postoperative bleeding versus venous thromboembolism (VTE) prevention, particularly the length of postoperative VTE prophylaxis, must be considered and tailored to individual patients. We utilize a risk-calculator created by Aminian and colleagues at the Cleveland Clinic. 5 The model, validated using the 2013 American College of Surgeons-National Surgical Quality Improvement Program dataset, assesses 10 categorical variables to determine post-operative risk of VTE after discharge. Those with VTE risk >.4% are determined high-risk, for whom post-discharge pharmacoprophylaxis is recommended. As in our study, Aminian et al found that most VTE occurs within two weeks after discharge. Thus, correctly screening to identify high-risk patients for close follow up within the first two weeks after surgery is critical.
Regarding therapy choice, there is no consensus on optimal anticoagulant, dosing, or duration of thromboprophylaxis. Rodríguez and colleagues found that thromboprophylaxis for the entire 2-3 day hospital stay after LSG with LMWH followed by rivaroxaban 10 mg daily for 10 days reduced cases of PMVT without increasing bleeding complications. 6 Other studies have found enoxaparin (Lovenox, Sanofi-Aventis) 40 mg twice daily for 10-14 days to be effective, with a bleeding and mortality rates of 0% after three months. 7 Further evaluation is warranted to determine the effectiveness of available anticoagulation medications and to establish clear guidelines for extended thromboprophylaxis in patients undergoing bariatric surgery.
Importantly, there is also no current consensus regarding duration and mechanism of therapy for those who ultimately develop PMVT post LSG. Our approach is multi-disciplinary, including input from Surgery, Hematology, and IR. In acutely symptomatic patients with high clot burden, or in patients who do not improve following inpatient anticoagulation, IR is consulted for potential thrombolytic intervention. The data are sparse regarding when and how to initiate endovascular therapies in the setting of PMVT. It has been shown that transcatheter thrombolysis can decrease patient death, resolve thrombus, improve symptoms and avoid bowel resection, but at the cost of a high complication rate of up to 60%. 8 Decisions regarding when and how to initiate endovascular therapies will continue to be based on local expertise, availability of evolving endovascular tools and careful interdisciplinary patient selection.
Hematology is then consulted regarding anticoagulant drug choice and length of therapy, and typically recommend 2-3 weeks of LMWH or fondaparinux followed by 3-6 months of a direct-acting oral anticoagulant (DOAC), such as rivaroxaban (Xarelto, Johnson & Johnson) or apixaban (Eliquis, Bristol-Myers Squibb), or warfarin (Coumadin, Bristol-Myers Squibb), per patient preference. Our multidisciplinary approach has been critical to achieving clot resolution and positive patient outcomes in all patients discussed at 6- and 12-month postoperative follow up.
PMVT is a serious but potentially preventable complication of LSG. Further development of prophylactic tools that quantify risk of VTE status post-bariatric surgery will help reduce morbidity and mortality related to PMVT. However, there is a lack of clear guidance regarding prophylactic and therapeutic anticoagulation in those undergoing bariatric procedures. We advise discontinuation of estrogen-containing therapies several weeks before LSG and use of extended post-surgical thromboprophylaxis for bariatric patients judged to be higher risk on a bariatric-specific VTE risk calculator, or when patient-specific history or clinical assessment raises concerns. Preventing PMVT relies on identifying individual VTE and bleeding risk factors. Further studies such as retrospective case series or prospective registry analyses of the prevalence of PMVT and surgical and patient-specific VTE risk factors will inform development of guidelines for VTE and bleeding risk-stratification. Regarding optimal treatment of PMVT, acute management is best done with a multi-disciplinary approach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.