
Abstract
Practices in surgical repair of uncomplicated gastroschisis are varied. Data regarding hospital volume, surgical technique, clinical outcomes, and costs remain limited. Neonatal patients with uncomplicated gastroschisis were identified using the 2015-2019 National Readmissions Database. Hospital volume tertiles were determined, and sutureless or fascial repair techniques were enumerated. High volume centers (HVC) comprised the top tertile. Hospital-level variability in surgical technique was determined. Adjusted multivariable analysis was performed to compare clinical outcomes and costs among HVC and lower-volume centers and among repair techniques. Of an estimated 2903 hospitalizations meeting inclusion criteria, 23.5% occurred at HVC. There was 42.4% variation among sutureless and fascial repair techniques across all hospitals. Among HVC and lower-volume centers, there were no significant differences in rates of 30-day readmission or complication; however, HVC were associated with greater cost and length of stay. Those with codes for fascial repair technique experienced greater lengths of stay, costs, and rates of complication. Codes for surgical repair technique for uncomplicated gastroschisis vary widely, while outcomes are equivalent across strata of hospital volume. Those with codes for sutureless technique were associated with favorable clinical outcomes, irrespective of hospital volume. Guidelines for management of uncomplicated gastroschisis should account for hospital volume, variation in technique, outcomes, and resource utilization.
Introduction
Gastroschisis affects an estimated 4.9 per 10 000 births in the US, and its incidence is increasing.1,2 Gastroschisis requires urgent postnatal surgical evaluation to minimize complications such as fluid and heat loss, infection, and bowel ischemia or necrosis.3,4 Although operative repair of the fascia remains a standard treatment, surgeons are more frequently performing a sutureless technique comprised of reducing abdominal contents, folding the umbilical stalk over the defect, and covering with a water-tight dressing.3,5 Despite advantages of the sutureless technique, it is performed inconsistently across a variety of pediatric surgical centers.6,7
Hospital volume is frequently cited as a factor in surgical outcomes.8,9 Data are lacking regarding hospital variation in surgical technique in uncomplicated gastroschisis. Factors underlying this variation have not been examined at the national level. The association of hospital variability and selection of technique for the repair of gastroschisis may inform the adoption of less invasive approaches. In the present study, we used a national database to characterize variations in technique codes for repair of uncomplicated gastroschisis, and clinical outcomes by technique and hospital volume. We analyzed readmission rates, complications, length of stay, and costs of care by hospital volume and surgical technique. We hypothesized that centers with high-volume would have reduced rates of readmission and complication.
Methods
All neonatal patients with a diagnosis code for gastroschisis were identified using the 2015-2019 National Readmissions Database (NRD), a nationally representative, all-payer database maintained by the Healthcare Cost and Utilization Project. 10 We classified clinical and operative factors of interest using the International Classification of Disease Tenth Revision (ICD-10) diagnosis code “Q793” for gastroschisis. Uncomplicated gastroschisis was defined to exclude patients with respiratory distress, volvulus, intestinal atresia, perforation, or necrotizing enterocolitis.11,12 Patient groups included those repaired via surgical fascial dissection and closure or sutureless technique to the extent coded within the NRD. Hospitals were classified as low- (LVC), medium- (MVC), or high-volume centers (HVC) according to tertiles of annual gastroschisis case volume. Outcomes of interest included inter-hospital variations in surgical technique. Hospital volume tertiles were delineated and mean annual operations for uncomplicated gastroschisis were calculated for each stratum of hospital volume. The intraclass correlation coefficient (ICC) was calculated to determine the proportion of total observed variation in operative approach that was explained by inter-hospital differences. 13
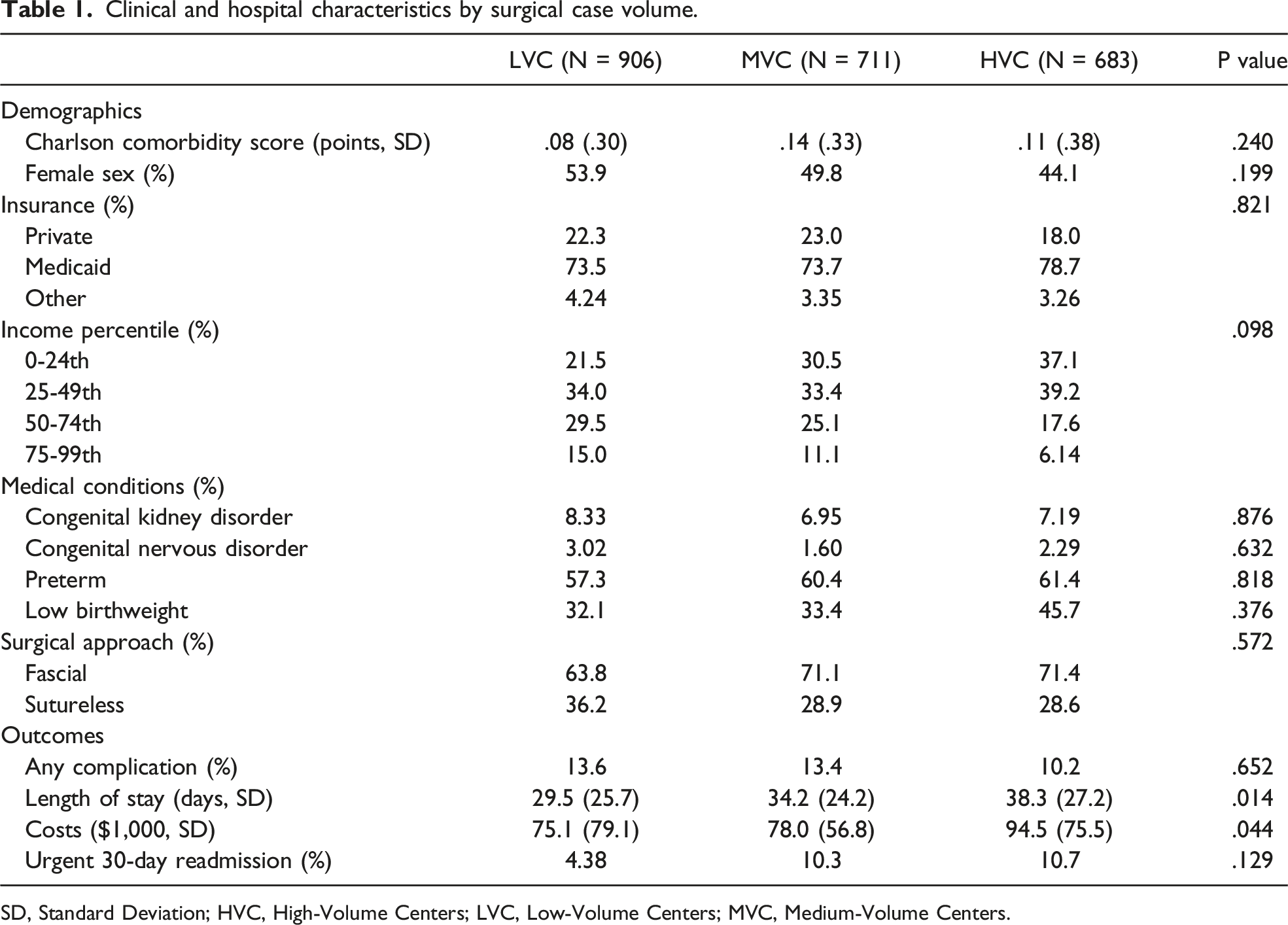
Demographic and clinical factors by volume tertile were tabulated. Additional outcomes of interest included postoperative complications, 30-day non-elective readmission, hospital length of stay, and costs of inpatient care. Total hospitalization costs (incurred by the hospital per admission) were calculated using hospital-specific NRD cost-to-charge ratios and were normalized to the 2019 Personal Health Care Index. For analysis, postoperative complications included cardiac, renal, respiratory, thromboembolic, infectious, and intraoperative categories such as hemorrhage and bowel perforation. Rates of the most common complications were calculated.
Multivariable linear and logistic regression models were developed to evaluate independent differences in rates of readmission, complication, costs, and lengths of stay among hospital volume tertiles. Secondary analysis was performed to identify independent associations of operative technique with the above outcome measures. These models adjusted for birthweight, preterm delivery, congenital anomalies, gender, surgical approach, volume, Charlson score, insurance status, patient family income, and year. Individual characteristics such as defect size, bowel edema or matting, and extent of organs extruded are not represented in the NRD dataset and were not included in this analysis. Hospital variation was assessed using random effects modeling. The risk-adjusted association of covariates with specified outcomes are reported as adjusted odds ratios (AOR) for dichotomous outcomes or beta coefficients (β) for continuous variables, with 95% confidence intervals (CI) for each. All analyses were performed using Stata 16.1. This study was deemed exempt from full review by the Institutional Review Board of the University of California, Los Angeles.
Results
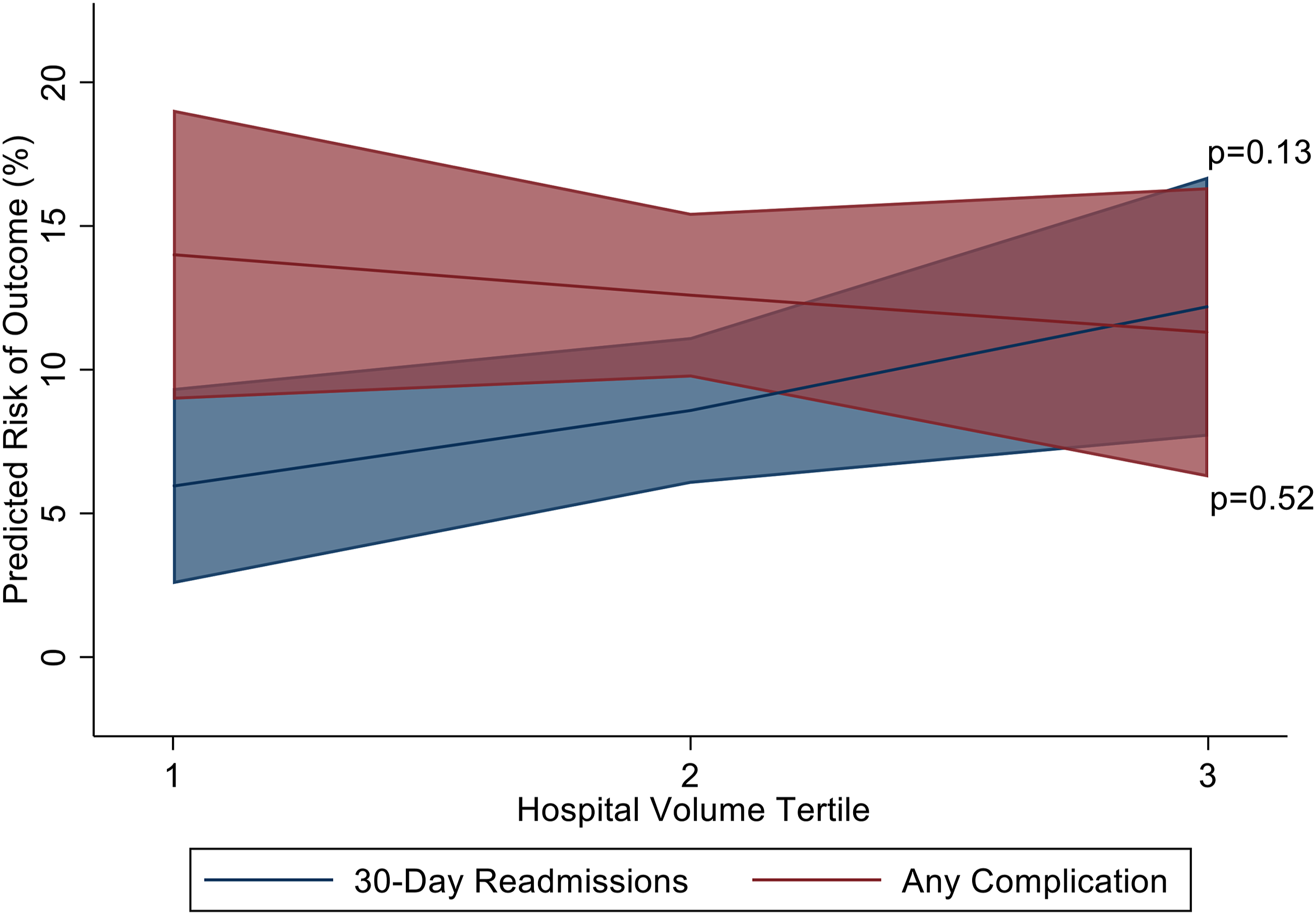
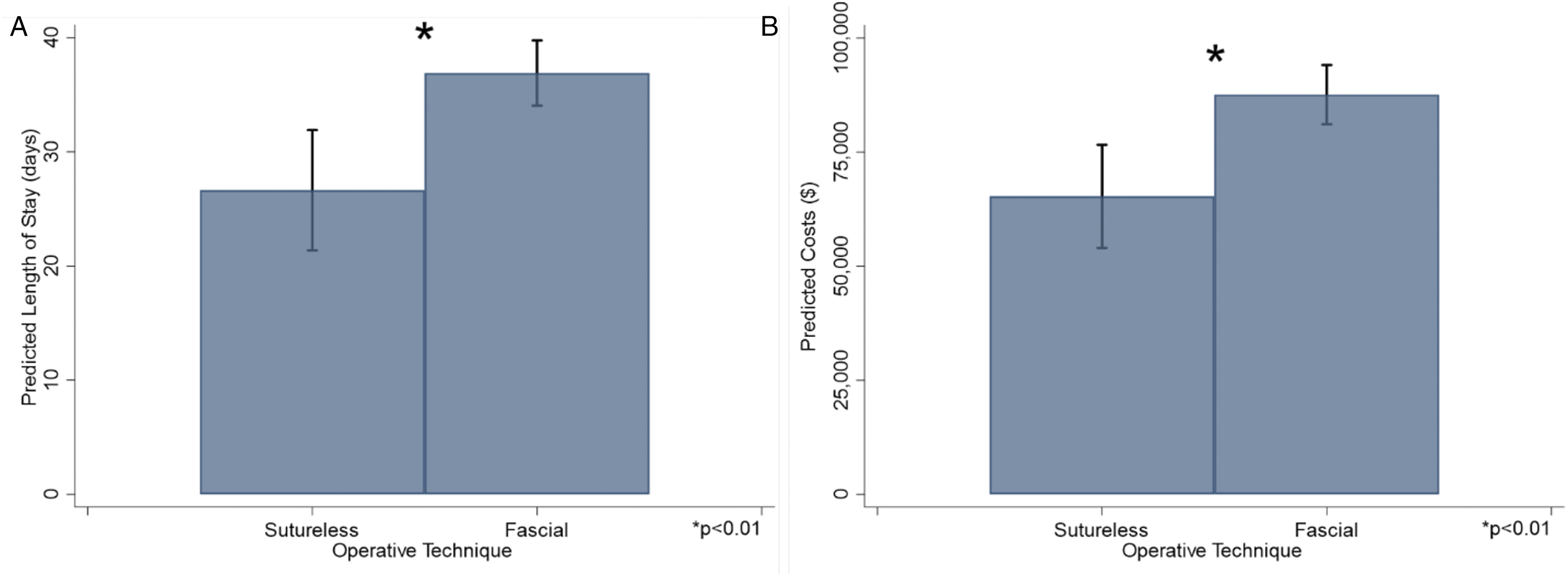
An estimated 2903 hospitalizations met inclusion criteria at 218 unique centers. Among them, 683 hospitalizations (23.5%) occurred at HVC. Mean annual operations for uncomplicated gastroschisis was 11.8 at HVC and 4.9 at LVC. While fascial repair codes were logged with similar frequency across volume strata, there was wide variation among the two technique codes across all hospitals, as indicated by an ICC of 42.4% (Figure 1). Those with codes for sutureless technique were performed earlier in the hospitalization (1.6 vs 3.3 days; P = .01). Table 1 shows demographic and clinical factors by volume tertile. On unadjusted analysis, compared with MVC and LVC, HVC had similar rates of complications and readmissions but longer lengths of stay and higher costs. The most common recorded complications included respiratory distress (8.4%) and infections (4.1%). On multivariable adjusted analysis, differences among HVC and LVC in 30-day readmission rates (AOR: 2.38, 95% CI: .78-7.26) and odds of complications (AOR: .75, 95% CI: .20-1.83, Figure 2) were not statistically significant. Adjusted costs were higher for HVC as compared to LVC (β: + $20,264, 95% CI: 204-40 323), as was length of stay (β: +8.27 days, 95% CI: 1.62-14.9). Compared with sutureless technique, those with codes for fascial technique had greater lengths of hospital stay (Figure 3A) and costs of care (Figure 3B) after multivariable adjustment. Fascial technique code was associated with an increased odds of complications (AOR: 3.18, 95% CI: 1.43-7.09), but not with readmissions (AOR: 1.27, 95% CI: .43-3.73). Upon adjusting for length of stay, HVC no longer significantly differed in costs from MVC and LVC (β: + $2,191, 95% CI: −13 413 to +17 668). Likewise, costs were not significantly different among those with codes for fascial and sutureless techniques (β: + $1,109, 95% CI: −7336 to 9554). Hospital variation in gastroschisis repair technique. ICC: intraclass correlation coefficient. Clinical and hospital characteristics by surgical case volume. SD, Standard Deviation; HVC, High-Volume Centers; LVC, Low-Volume Centers; MVC, Medium-Volume Centers. Adjusted associations of hospital volumes and risks of readmission and complications. Adjusted length of stay and predicted costs by operative technique. (A) Predicted length of stay. (B) Predicted costs.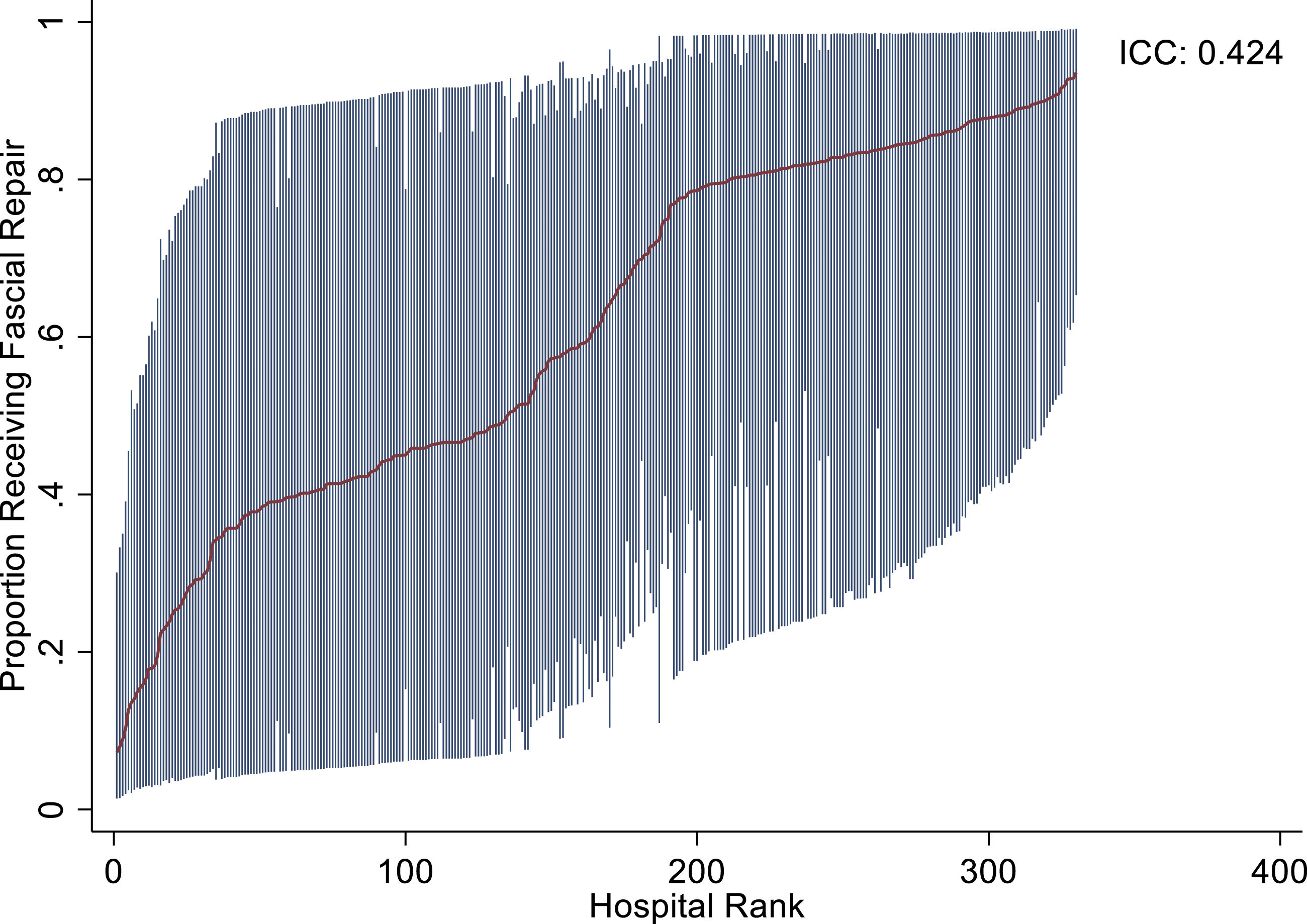
Discussion
In this retrospective cohort study, we evaluated associations of hospital volume and surgical technique codes with clinical and financial outcomes of repair of uncomplicated gastroschisis. Despite growing adoption of sutureless repairs, our data indicates a wide variety in coding practices of repair techniques by hospital, with nearly half of those codes explained by hospital factors alone. Contrary to our hypothesis, we found no association of surgical volume with variation in technique codes nor clinical outcomes; however, we did find resource utilization was increased in HVC. Furthermore, we found those logged with sutureless technique codes were associated with reduced odds of complication, length of stay, and cost when compared with those with fascial technique codes.
A recent study by Viglianti and colleagues showed that, after adjustment for patient factors, hospital-level variation in care affects outcomes such as mortality and critical illness in adults in intensive care units. 13 In that study, variation represented a metric of quality of care for each center. In our study, the variability in techniques we discovered is unlikely to reflect hospital performance, but rather a lack of consensus guidelines on techniques, venues, and coding practices in the repair of uncomplicated gastroschisis, some of which is suggested by Aldrink and associates. 14 In 2021, Joharifard and colleagues observed that the initiation of a protocol increased rates of sutureless repair without concomitant increases in postoperative complications. 15 Consistent with those findings, ours further support that creation of standard guidelines for management of uncomplicated gastroschisis, independently of variations in case volumes across hospitals.
Surgical volume is often cited as a predictor of clinical outcomes in pediatric 8 and adult surgical settings. 9 While many have supported the centralization of surgical care, 16 a lack of data exists to support such practices for those with uncomplicated gastroschisis. In 2017, Dubrovsky and associates showed that surgical volume was not associated with mortality in a national sample of patients with gastroschisis. 17 Similarly, in 2019 these results were recapitulated in a study by Hong and colleagues. 18 Importantly, these studies examined samples of patients with any classification of gastroschisis complexity. In the present study, we found no differences by hospital volume in odds of complications or 30-day urgent readmissions following repair of uncomplicated gastroschisis. Additionally, we discovered that costs and lengths of stay were increased at HVC relative to MVC and LVC, similar to other studies. 19 Our findings suggest that HVC may incur greater expense without a clear clinical benefit in treating uncomplicated gastroschisis as compared with lower-volume centers with pediatric surgical capabilities.
Debates are ongoing regarding the risks and benefits of fascial and sutureless techniques. Recent studies have demonstrated fascial technique is associated with increased duration of mechanical ventilation and administration of analgesics, and decreased risk of post-repair umbilical hernia. 20 Gurien and colleagues in 2017 found that early closures, including those performed with sutureless technique, were associated with increases in requirements for mechanical ventilation and nutritional support. 21 More recently, sutureless technique has become more popular. 3 In our study, those with a procedure code for fascial technique experienced greater odds of complication and resource utilization when compared to those with sutureless technique codes. This may in part be due to a longer time to intervention among those with fascial repair codes; however, we determined that coding practices vary widely across hospital settings. We are unable to speculate based upon our analysis the superiority of one technique over another; however, our findings do suggest the presence of an as-yet undefined factor that leads to differential coding practices at the hospitals. This study emphasizes the need for standardized coding to allow for accurate categorization of sutureless and fascial techniques. Standard codes will be crucial to the future study of cost-effectiveness and hospital volumes by repair technique for uncomplicated gastroschisis.
This retrospective study has several limitations. The NRD is dependent upon ICD coding, which as discussed above, varies widely across participating centers. Those coded as fascial versus sutureless techniques may be misrepresented secondary to these inconsistencies. When conducting an internal audit at our institution, we determined that a substantial proportion of sutureless closures were coded as fascial repairs. We are therefore unable to draw conclusions regarding surgical techniques performed, but rather only regarding codes logged. Additionally, the NRD does not represent anatomic or physiologic information specific to each individual’s gastroschisis defect, save for of diagnostic codes of complications. These factors may have associations with selection or coding of repair techniques. Despite these limitations, NRD comprises the largest available readmissions database to assess the clinical and financial outcomes for patients with uncomplicated gastroschisis.
In conclusion, in a nationally representative dataset, our analysis resulted in discovery of wide variability of hospital practices without variations in rates of complications across strata of hospital volume. Treatment at lower-volume centers may offer a value-based alternative to treatment at HVC. Guidelines for the management of uncomplicated gastroschisis should account for hospital volume, variation in techniques, hospital coding practices, outcomes, and resource utilization.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.