
Abstract
Introduction
Appendicitis is one of the most common surgical diagnoses in the pediatric population. 1 According to the Kid’s Inpatient Database in 2016, appendectomies were the most common surgical procedure performed based on ICD codes. 2 This procedure is within the scope of practice of general surgeons (GS) and pediatric surgeons (PS). We have previously demonstrated that both surgeon subgroups perform the significant proportion of appendectomies on pediatric patients, with PS performing 44.6% and GS performing 32.5% of these operations in North Carolina. 3 Appendectomies performed by GS on pediatric patients in NC were also associated with higher charges when compared to PS. 3 Given their high volume, appendectomies serve as a great model for analyzing intersurgeon differences in postoperative outcomes and perioperative resource utilization.
Surgical technique preferences have adapted over time, with minimally invasive surgery becoming routine practice. 4 Changes to other components of perioperative care have also occurred as a result of access to innovative technologies medications. Clinical practice guidelines can be used to standardize the use of perioperative resources such as imaging studies, antibiotics, and opioid medications. Analyzing patient outcomes using these various resources can be used to inform clinical practice. Decreasing variations between PS and GS in the use of perioperative resources and patient outcomes allows for quality improvement while maintaining the value of care being delivered to this patient population.
Previous systematic reviews5-7 have analyzed outcomes between GS and PS but have not included other outcomes such as use of antibiotics and opioid medication. Additional studies have been published on this topic that have not been included in previous reviews. The goal of this systematic review and meta-analysis is to assess the influence of surgeon specialty on the post-operative outcomes and perioperative resource utilization for pediatric appendectomies. Based on our previous findings, we hypothesize that there will be a difference in outcomes and higher resource utilization for GS compared to PS.
Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement. 8
Eligibility Criteria
Eligibility criteria were established a priori with respect to populations, exposures, comparators, outcomes, timing, setting, and study design (Supplementary Table 1). Studies including patients less than 18 years of age undergoing appendectomies were considered eligible. Eligible studies had to include clear measures of at least one of the outcomes for general surgeons (GS) and pediatric surgeons (PS). General surgeons included general surgery residents and trauma and acute care surgeons. Eligible outcomes were broadly defined to include all potentially relevant studies including hospital length of stay (LOS), negative appendectomy rate, and wound infections/surgical site infections (WI/SSI). A full list of eligible outcomes is provided in Table (1). Observational and randomized controlled studies occurring in inpatient hospital settings published since 1990 were included (Supplementary Table 1).
Data Sources and Searches
PubMed online database was searched from January 1, 1990, to March 7, 2022. Search terms were related to pediatric patients and appendectomies. The full search strategy can be found in Supplementary Table 2. Additionally, any systematic reviews identified using this search strategy were reviewed for additional articles that met the eligibility criteria but were not identified during the original search.
Study Selection
All eligible studies were extracted and organized using Covidence systematic review management software. A single reviewer screened all titles and abstracts for inclusion using the eligibility criteria previously described. A full text review was then conducted of all eligible studies with justification for exclusion recorded for each study. The study selection procedure is described in the PRISMA Flow Diagram in Supplementary Figure 1.
Data Collection Process and Data Items
Information was extracted from each study using an electronic spreadsheet. Data extracted included the following variables: publication information (authors and year), source population, study design and duration, outcomes reported (LOS, negative appendectomy rate, readmission rate), and main results. The outcomes included in the meta-analysis included negative appendectomy rate, readmission within 30 days, wound infection/surgical site infection, and use of preoperative imaging (including ultrasound (US), computerized tomography (CT), and magnetic resonance imaging (MRI)). Definitions of each of these outcomes were specified in each manuscript. Data was pooled to determine risk ratios for treatment by general surgeons compared to pediatric surgeons. Heterogeneity was assessed using the I2 statistic, with higher values signifying increased heterogeneity in the data. Risk ratios were reported with 95% confidence intervals (CIs) and P-values < .05 were considered significant. Statistical analyses were conducted using Stata v16.0 (StataCorp, College Station, Texas).
Risk of Bias Analysis
The National Institute of Health (NIH) Quality Assessment Tool for Observation Cohort Studies 9 was used to assess the quality of the individual studies included in this analysis. The full table of assessment criteria can be found in Supplementary Table 5.
Results
Results of Literature Searches
The initial search strategy in PubMed yielded 4798 articles. One additional record was identified through hand-searching systematic reviews identified in the search strategy for articles not captured. Duplicate records (14 total) were removed, resulting in 4785 articles for screening. Eligibility criteria (outlined in Supplementary Table 1) were used to evaluate titles and abstracts and 4741 articles were determined to be irrelevant. The remaining 44 articles were screened with a full text review and 16 articles met full eligibility criteria. The most common reasons for exclusion were ineligible comparator and ineligible outcomes. The PRISMA Flow diagram for the article screening process, including reasons for full text exclusion are shown in Supplementary Figure 1.
Study Characteristics
Number of Studies Reporting Each Outcome.
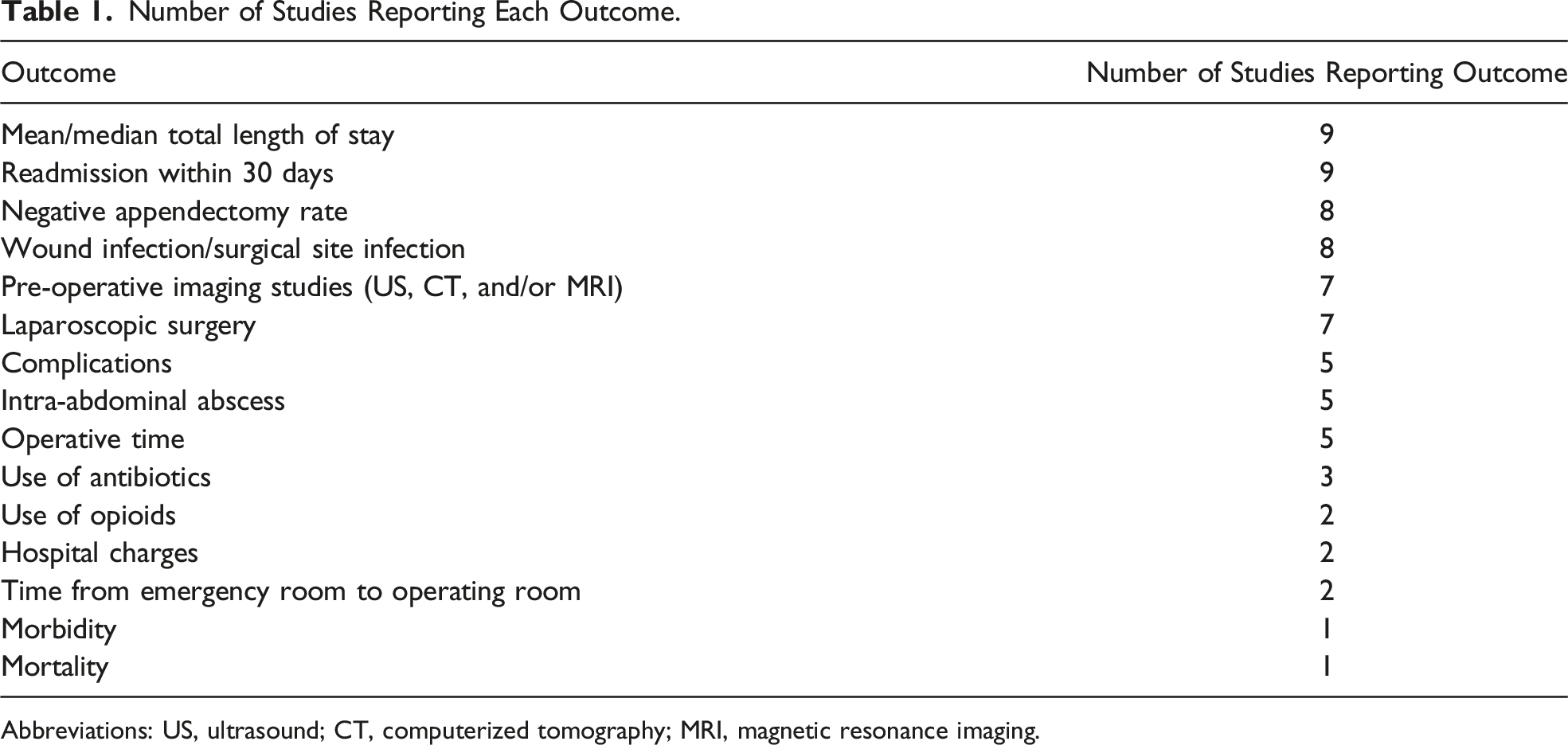
Abbreviations: US, ultrasound; CT, computerized tomography; MRI, magnetic resonance imaging.
Risk of Bias Analysis
Studies in this analysis were assessed as poor, fair, or good quality based on eligibility criteria, outcomes measured, and controlling for covariates. Most of the studies included in this analysis were considered of good quality. The full table of assessment criteria can be found in Supplementary Table 5.
Summary of Results
Nine studies10-14,17,20,22,23 reported on readmission rate within 30 days. There were 144 readmissions in the 4557 patients treated by GS and 85 readmissions in the 2300 patients treated by PS. The pooled risk ratio (RR) for this outcome was 1.61 (95% CI .66, 2.55). There was considerable heterogeneity between these studies with an I2 of 88.79% (Supplementary Figure 2)
Nine studies10-12,14,20-24 reported length of stay as an outcome. There was variation in reporting in this outcome with some studies providing values for overall patients in both groups, some reporting LOS for simple vs complicated appendicitis, and one reporting median length of stay. Average length of stay for simple appendicitis ranged from 1.70 to 3.5 days for GS and 1.82-4.1 days for PS. Average length of stay for complicated appendicitis ranged from 4.68 to 8.7 days for GS and 4.4-5.4 days for PS.
Eight studies10-12,17,18,20,22,24 reported the negative appendectomy rate. There were 4632 normal appendixes in the 51,115 patients treated by GS and 913 in the 14,824 patients treated by PS. The pooled RR for this outcome was 1.47 (95% CI 1.10, 1.84). There was considerable heterogeneity between these studies with an I2 of 91.85% (Supplementary Figure 3). (Figure 1). Forrest plot of relative risk (RR) of negative appendectomy comparing general surgeons to pediatric surgeons. Red line indicates RR = 1.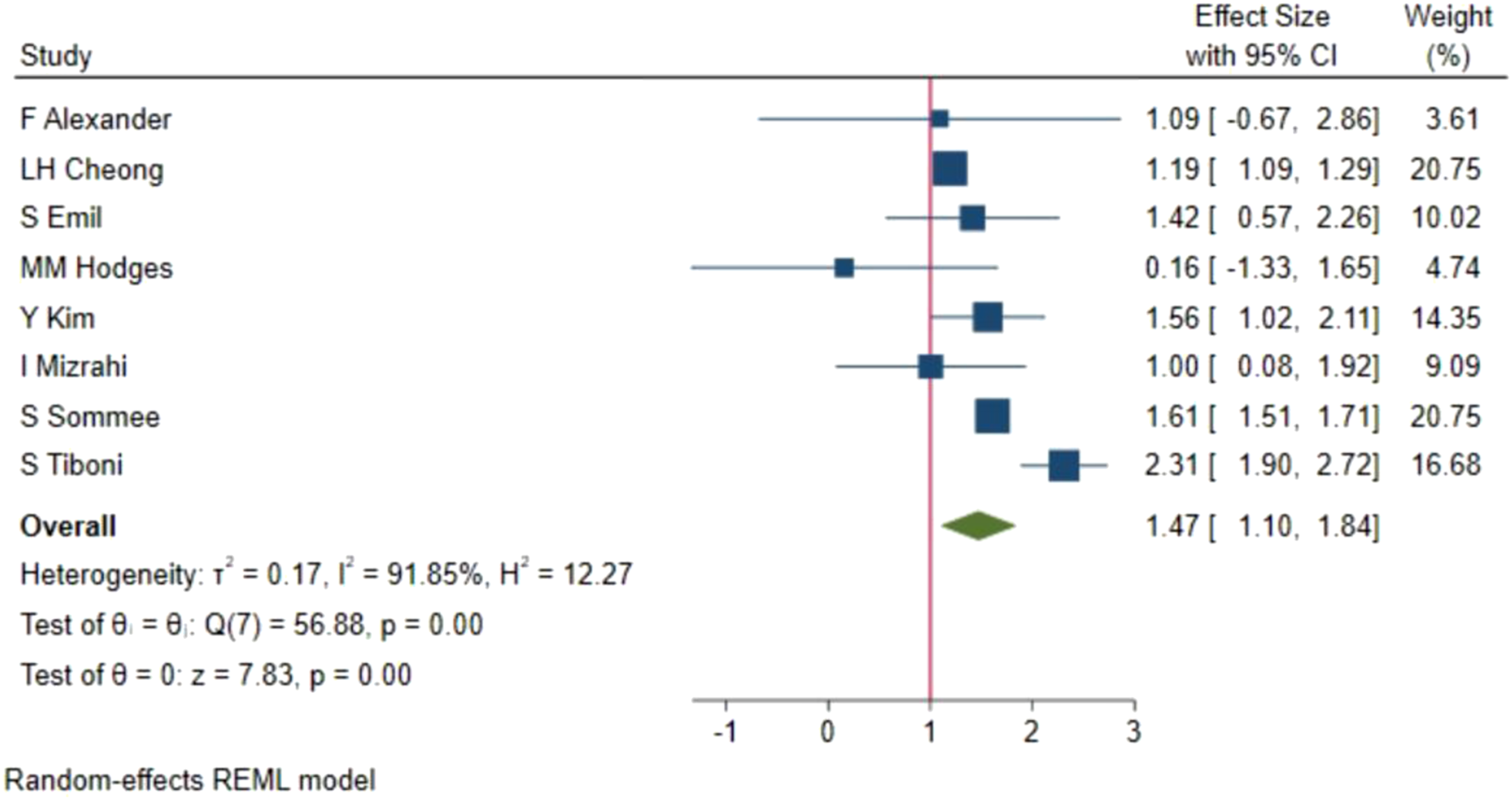
Eight studies10,11,13,14,17,20,22,24 reported rate of wound infection or surgical site infection.
This outcome was identified in 317 of the 21 117 patients treated by GS and 130 of the 5473 patients treated by PS. The pooled RR for this outcome was 1.07 (95% CI .55–1.60). There was substantial heterogeneity between these studies with an I2 of 55.66% (Supplementary Figure 3).
Seven studies10,11,14,20,22,23,26 reported use of preoperative imaging (including US, CT, and/or MRI studies). These imaging techniques were used on 3311 in the 3940 patients treated by GS and 1516 of the 1814 patients treated by PS. The pooled RR for this outcome was .98 (95% CI .90, 1.05). There was considerable heterogeneity between these studies with an I2 of 83.16% (Supplementary Figure 4).
Seven studies10-13,15,20,23 reported the use of laparoscopic surgery as an outcome. This technique was used in 19,357 of the 137,531 operations by GS and 11,012 of the 36,976 operations by PS. The pooled RR for this outcome was 1.87 (95% CI .21, 3.53). There was substantial heterogeneity between these studies with an I2 of 99.95% (Supplementary Figure 5)
Five studies10,12,14,20,22 reported complication rates. This outcome was identified in 57 of the 805 patients treated by GS and 42 of the 778 patients treated by PS. The pooled RR was 1.40 (95% CI .83, 1.97). There was moderate heterogeneity between these studies with an I2 of 46.10% (Supplementary Figure 6)
Five studies10,11,14,17,22 reported the rate of intra-abdominal abscesses. One study (Da silva) was excluded from the meta-analysis as 0 events were reported in the PS group. This outcome was identified in 24 of the 992 patients treated by GS and 27 of the 839 patients treated by PS. The pooled RR was .80 (95% CI .03, 1.58). The heterogeneity between the studies might not be important with an I2 of 28.36% (Supplementary Figure 7).
Five studies12-14,20,22 reported operative time as an outcome. Average operative time ranged from 40 to 83.92 minutes for GS and 43.2-83.86 minutes for PS. One study 20 reported median operative time to be 49 minutes (IQR 39-61) for GS and 49 minutes (IQR 38-69) for PS.
Three studies reported the use of antibiotics as an outcome, but the measurement of this outcome varied between studies. One study 14 reported the median length of antibiotic treatment to be 2 days (IQR 2-4) for GS and 4 days (IQR 3-7 for PS). One study 11 reported the percentage of patients receiving antibiotics, with 77% of GS patients and 55% of PS patients receiving them post-op and 15% of GS and 4% of PS discharged on oral antibiotics. Another study 22 also reported the percentage of patients receiving antibiotics, with 53% of GS and 20% of PS patients receiving broad-spectrum antibiotics, 30% of GS and 13% of PS patients continuing antibiotics at home, and the average length of home antibiotics 3.1 ± .3 days for GS and .6 ± 1 day for PS.
Two studies included the use of opioids as an outcome. One study 19 reported the average oral morphine equivalents (OME) to be 90 for GS patients and 59 for PS patients. One study 25 reported that 72% of GS patients and 57% of PS patients were prescribed opioids, with the mean duration of opioids prescribed to be 4.25 days for GS and 3.12 days for PS.
Two studies reported hospital charges as an outcome. One study 16 reported an increase of $942 (95% CI $862–1021) Canadian dollars when the patient was treated by PS. One study 11 reported median hospital charges for simple appendicitis patients were $11,613 (IQR $9525- $14,698) for GS and $10,735 (IQR $8161-$12,510) for PS. For patients with complicated appendicitis, median hospital charges were $18,351 (IQR $14,435-$23,888) for GS and $19,125 (IQR $15,448-$23,211) for PS.
Two studies reported the time from the emergency room to the operating room as an outcome. With one study 20 finding the median time to be 8.7 hours (IQR 6.9-10.9) for GS and 7 hours (IQR 5-10 hours) for PS. The other study 22 found the average time to be 419 ± 14 minutes for GS and 529 ± 24 min for PS.
Mortality was reported by one study 24 with 0 events in both groups. One study 16 reported all-cause morbidity, with 1567 patients out of 29,876 in the GS group and 1097 patients out of 11,636 in the PS group.
Discussion
This review found that there was no significant difference between GS and PS for the rate of 30-day readmission, rate of WI/SSI, use of perioperative imaging, laparoscopic surgery, rate of complications, and rate of abscesses. There was a significant difference in the rate of negative appendectomies with a pooled RR of 1.47 (95% CI 1.10, 1.84) when comparing GS to PS.
This review was limited by the heterogeneity in the definition of the outcomes such as complication rate. Additionally, some studies11,24 only reported outcomes as percentages and did not include overall sample sizes. There was also heterogeneity in the reporting of outcomes, with some studies providing overall events and others having additional subgroups for simple and complicated patients. All but one of the studies included in this analysis were retrospective data collection which can lead to bias. Eight of the included studies used databases for data collection which can have inaccuracies in their reporting. Another factor that could influence outcomes is the severity of disease presentation, with several studies11,17,21,23,24 reporting that PS treated more patients with severe disease. Included studies came from a variety of countries including the United States, Canada, and the United Kingdom. Differences in these populations may be due to a variety of factors such as different health care system structures.
Conclusion
In summary, these studies provide evidence that the negative appendectomy rate for pediatric appendectomies differs between GS and PS. Other outcomes such as rate of readmission, use of perioperative imaging studies, and rate of complications did not differ between these groups. Additional prospective studies are warranted to study these various outcomes and use of resources. This could enable a gain in understanding of how surgeon specialization impacts the quality of care delivered to pediatric patients. With a significant proportion of pediatric surgical care delivered by GS and PS, it is critical to understand where clinical practice and outcomes may differ between these groups to identify targets for quality improvement.
Supplemental Material
Supplemental Material - Difference in Postoperative Outcomes and Perioperative Resource Utilization Between General Surgeons and Pediatric Surgeons: A Systematic Review
Supplemental Material for Difference in Postoperative Outcomes and Perioperative Resource Utilization Between General Surgeons and Pediatric Surgeons: A Systematic Review by Ali M. Eakes, Laura Burkbauer, Laura N. Purcell, Adesola C. Akinkuotu, Sean E. McLean, Anthony G. Charles, and Michael R. Phillips in The American Surgeon
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.