
Abstract
Background
Prisoners are a vulnerable population, and there are few contemporary studies that consider trauma patient outcomes within the prisoner population. Therefore, we sought to provide a descriptive analysis of prisoners involved in trauma and evaluate whether a healthcare disparity exists. We hypothesized that prisoners and non-prisoners have a similar risk of mortality and in-hospital complications after trauma.
Methods
The Trauma Quality Improvement Program (2015-2016) was queried for trauma patients based upon location inside or outside of prison at the time of injury. A multivariable logistic regression analysis was performed to compare these groups for risk of mortality—the primary outcome.
Results
From 593,818 trauma patients, 1115 were located in prison. Compared to non-prisoners, prisoner trauma patients had no significant difference in mortality (5.1 vs 6.0%, P = .204). However, after adjusting for covariates, prisoners had a shorter length of stay (LOS) (mean days, 6.3 vs 7.8, P < .001), shorter intensive care unit (ICU) LOS (mean days, 5.44 vs 5.89, P = .004), and fewer complications, including lower rates of drug/alcohol withdrawal (.4% vs 1.1%, P = .030), pneumonia (.5 vs 1.6%, P = .004), and urinary tract infections (.0 vs 1.1%, P < .001). Upon performing a multivariable logistic regression model, prisoner trauma patients had a similar associated risk of mortality compared to non-prisoners (OR 1.61, CI .52-4.94, P = .409).
Discussion
Our results suggest that prisoner trauma patients at least receive equivalent treatment in terms of mortality and may have better outcomes when considering some complications. Future prospective studies are needed to confirm these results and explore other factors, which impact prisoner patient outcomes.
Key Takeaways
Prisoner and non-prisoner trauma patients have no differences in rate or associated risk of mortality Prisoner trauma patients may have less in-hospital complications than non-prisoners Prisoner trauma patients have a decreased hospital length of stay compared to non-prisoners
Introduction
The United States (US) has the highest incarceration rate worldwide, with 440 prisoners per 100,000 of the national population, and an estimated 6.6 million US citizens within the correctional system as of 2017.1,2 In fact, this accounts for one quarter of the world’s prison population. Historically, prisoners represented a population that underwent horrific medical research experiments including those performed by the Nazis in World War II and even by the US Army in the 1970s.3-5 At the time, an estimated 90% of all drug research used prisoners, which also included testing chemical warfare agents without the requirement of obtaining informed consent. 6 However, throughout the 1970s to 1990s, increased public awareness ultimately led the US government to respond in the form of the National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research.6,7 Under Subpart C, additional regulations beyond the basic requirement for research with human subjects were set in place, which protected prisoners and ultimately led to a drastic decrease in studies performed on prisoners.6,8,9 For example, it classified prisoners as a vulnerable population similar to children, and prohibits certain forms of research such as medical experimentation, cosmetic research and pharmaceutical testing.6-9
From the 1970s to the mid-2000s, the incarcerated population has grown 5-fold. 6 Prisons have become overcrowded, and thus prisoners’ access to services and healthcare is limited. 10 In addition, many prison systems have come under fire for inadequate treatment of prisoners and are often characterized by high rates of communicable diseases, mental illness, and substance abuse.10,11
Unfortunately, limited contemporary literature regarding outcomes for prisoner trauma patients exists. Although prisoners have a 5-times higher rate of sustaining traumatic injury compared to non-incarcerated patients, the aforementioned constraints on research have made it increasingly difficult to study. Furthermore, researchers sometimes have difficulty obtaining informed consent, such as when a patient has a debilitating condition such as traumatic brain injury where a legally authorized representative is needed for decision-making.12-14 Therefore, we sought to provide a descriptive analysis of prisoner trauma patients and evaluate whether any healthcare disparity exist for this vulnerable population. We hypothesized that prisoner trauma patients have a similar risk of mortality and in-hospital complications compared to non-prisoner trauma patients.
Methods
This study was approved by the University of California, Irvine’s institutional review board (IRB). The IRB approved waiver of consent. We performed a retrospective analysis of the Trauma Quality Improvement Program (TQIP) between January 2015 and December 2016. TQIP began collecting the location where the trauma occurred beginning in 2015. All trauma patients ≥18 years of age sustaining injuries within prisons were identified using location codes listed in Supplemental Table.
The primary outcome studied was mortality. Secondary outcomes included total hospital length of stay (LOS), intensive care unit (ICU) LOS, ventilator days, and in-hospital complications. Variables collected included: age, gender, race, systolic blood pressure (SBP) on arrival, respiratory rate (RR) on arrival, heart rate on arrival, and total Glasgow coma scale (GCS) on arrival. Comorbidities included congestive heart failure (CHF), smoking status, chronic renal failure, cerebrovascular accident (CVA), diabetes (DM), cancer, history of myocardial infarction (MI), peripheral vascular disease (PVD), hypertension (HTN), chronic obstructive pulmonary disease (COPD), steroid use, cirrhosis, dementia, and psychiatric illness. The injury profile included the injury severity score (ISS), abbreviated injury scale (AIS), and injuries to the brain, face, spine, ribs, sternum, pelvis, extremities, intrathoracic organs, intraabdominal organs, crush injuries, and burns. Injuries were identified by the appropriate International Classification of Disease diagnosis codes (version 9).
All variables were coded as present or absent. Descriptive statistics were performed for all variables. A Student’s t-test or Mann-Whitney-U test was used to compare continuous variables and chi-square was used to compare categorical variables for bivariate analysis. Categorical data were reported as percentages, and continuous data were reported as medians with interquartile range. The magnitude of the association between predictor variables and mortality was first measured using a univariable logistic regression model. Covariates were chosen by a discussion among coauthors and review of the literature.15-17 Covariates with statistical significance (P < .20) were included in a hierarchical multivariable logistic regression model and the adjusted risk for mortality was reported with an odds ratio (OR) and 95% confidence intervals (CIs). Covariates included in this model were prison status, GCS, AIS, and documented medical comorbidities. All P-values were two-sided, with a statistical significance level of <.05. All analyses were performed with IBM SPSS Statistics for Windows (version 24, IBM Corp., Armonk, NY).
Results
Patient Characteristics
Baseline Characteristics for Non-Prisoner and Prisoner Patient Populations.
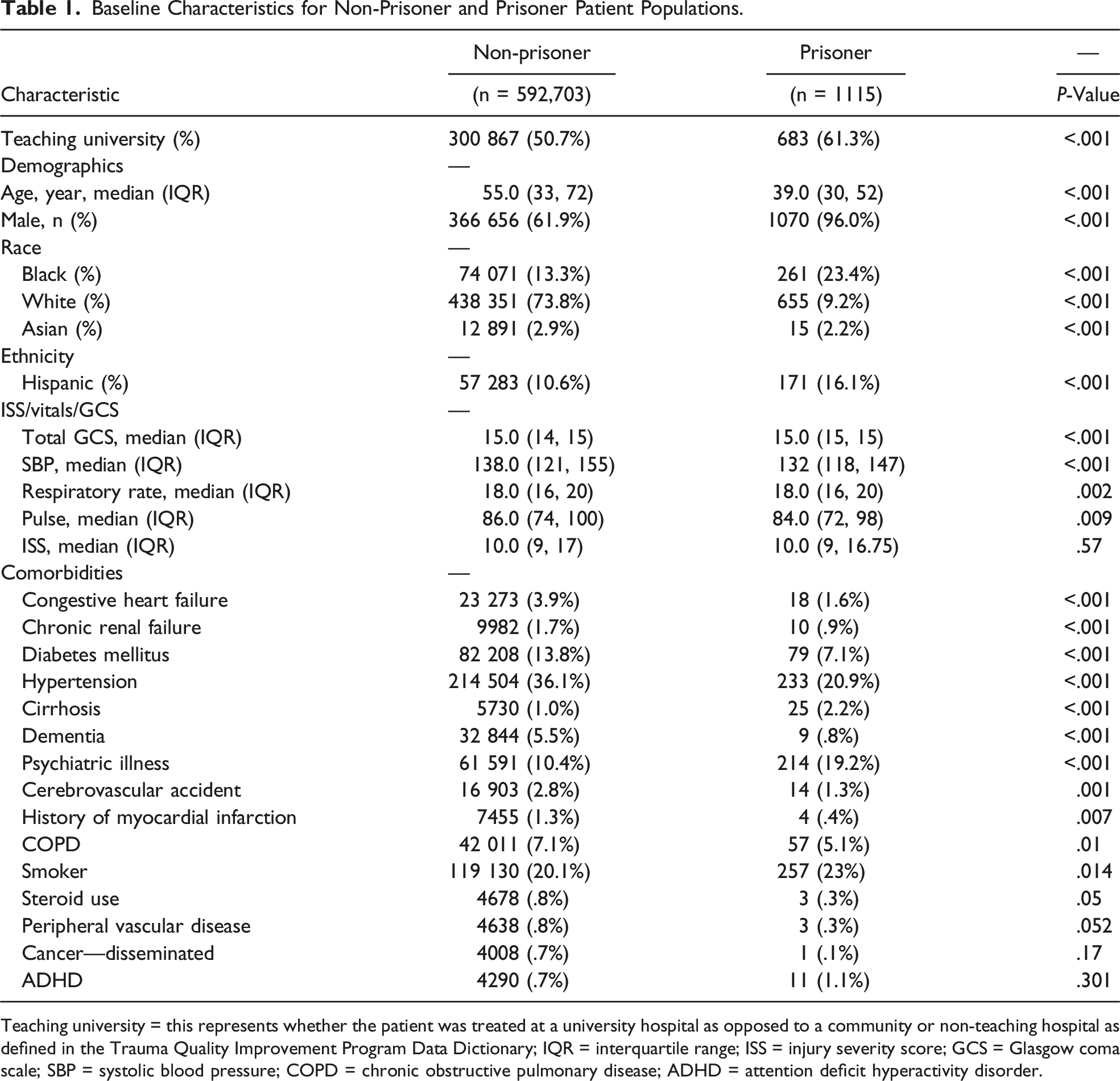
Teaching university = this represents whether the patient was treated at a university hospital as opposed to a community or non-teaching hospital as defined in the Trauma Quality Improvement Program Data Dictionary; IQR = interquartile range; ISS = injury severity score; GCS = Glasgow coma scale; SBP = systolic blood pressure; COPD = chronic obstructive pulmonary disease; ADHD = attention deficit hyperactivity disorder.
Injury Profiles for Non-Prisoner and Prisoner Patient Populations.
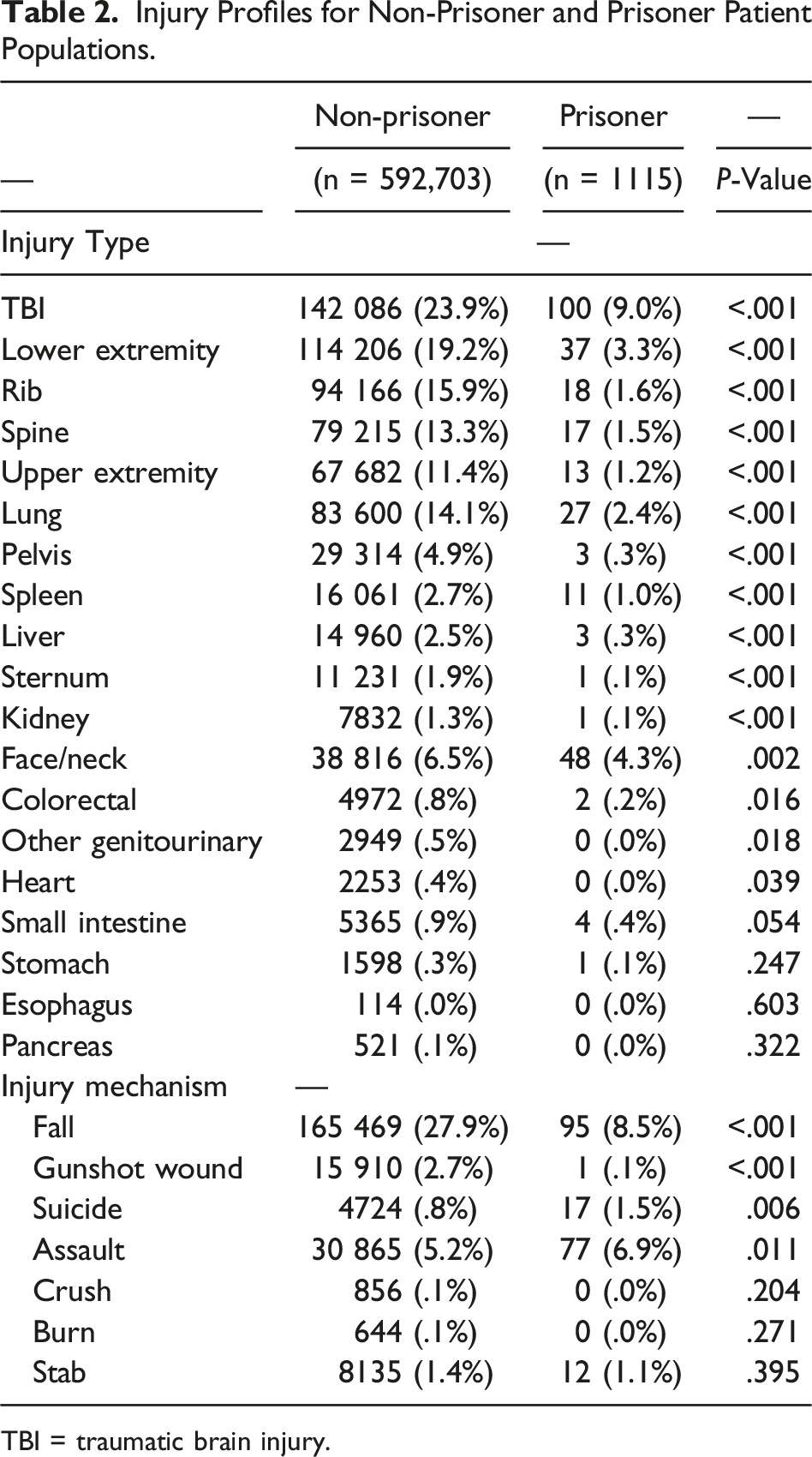
TBI = traumatic brain injury.
Primary and Secondary Outcomes
In-Hospital Complications for Non-Prisoner and Prisoner Patient Populations.
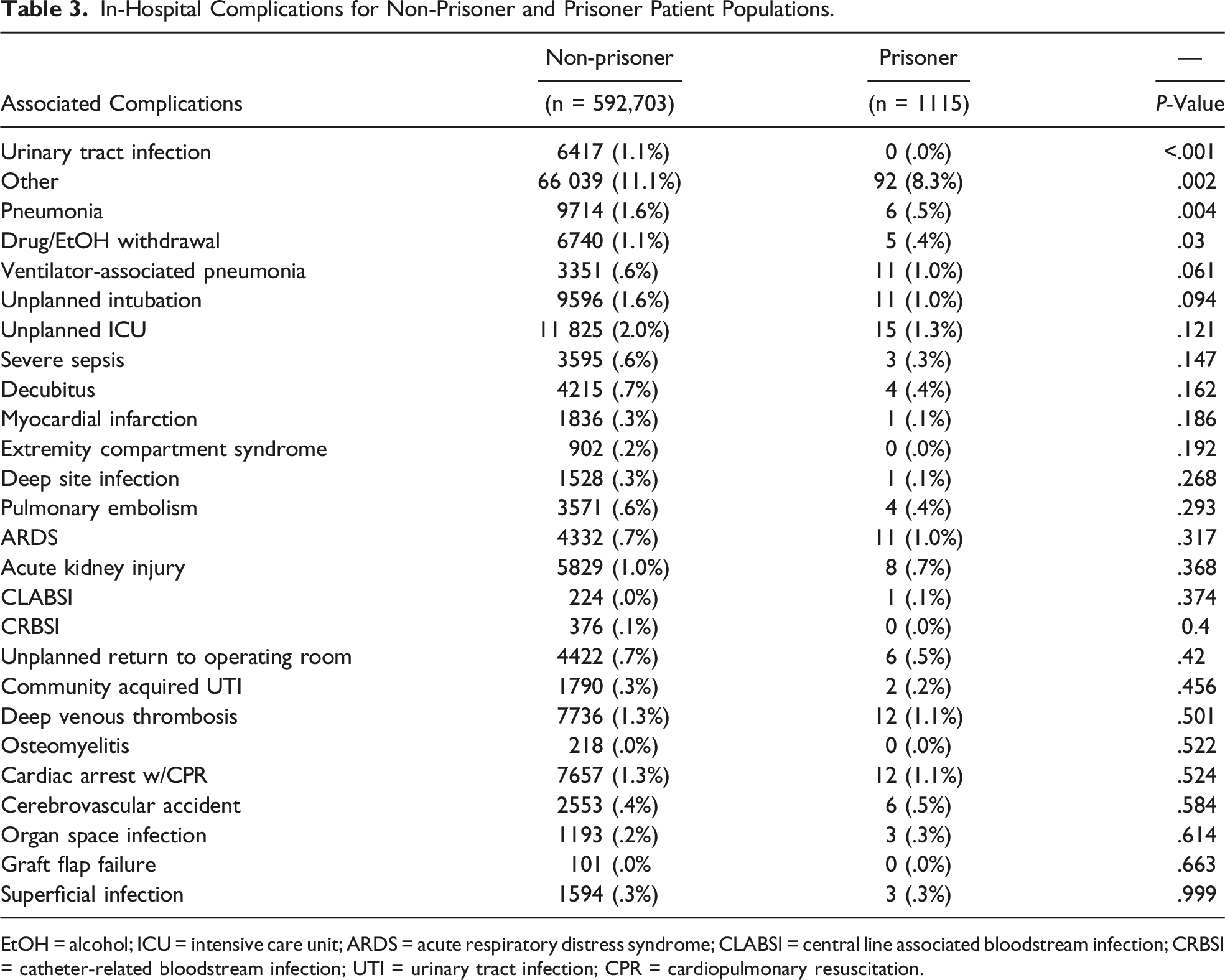
EtOH = alcohol; ICU = intensive care unit; ARDS = acute respiratory distress syndrome; CLABSI = central line associated bloodstream infection; CRBSI = catheter-related bloodstream infection; UTI = urinary tract infection; CPR = cardiopulmonary resuscitation.
Outcomes for Non-Prisoner and Prisoner Patient Populations.
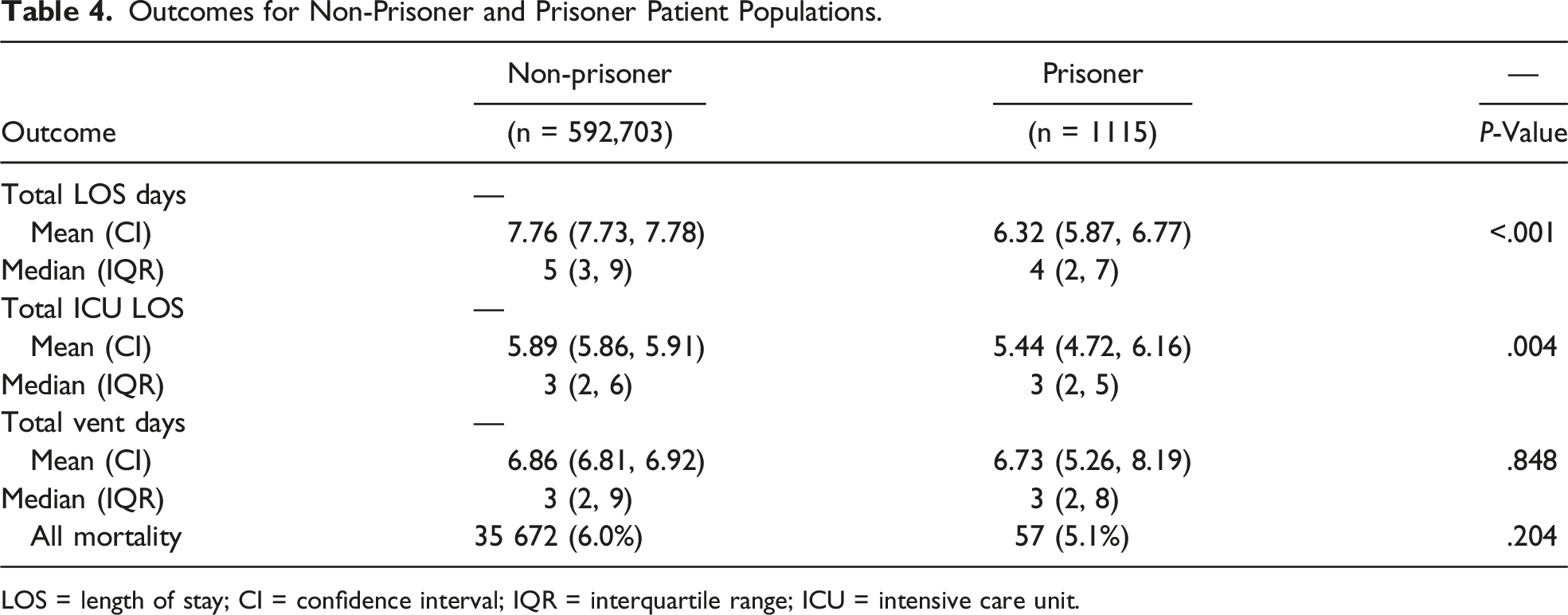
LOS = length of stay; CI = confidence interval; IQR = interquartile range; ICU = intensive care unit.
Risk of Mortality in Trauma Patients Who are Prisoners
Univariate Analysis for Risk of Mortality in Trauma.
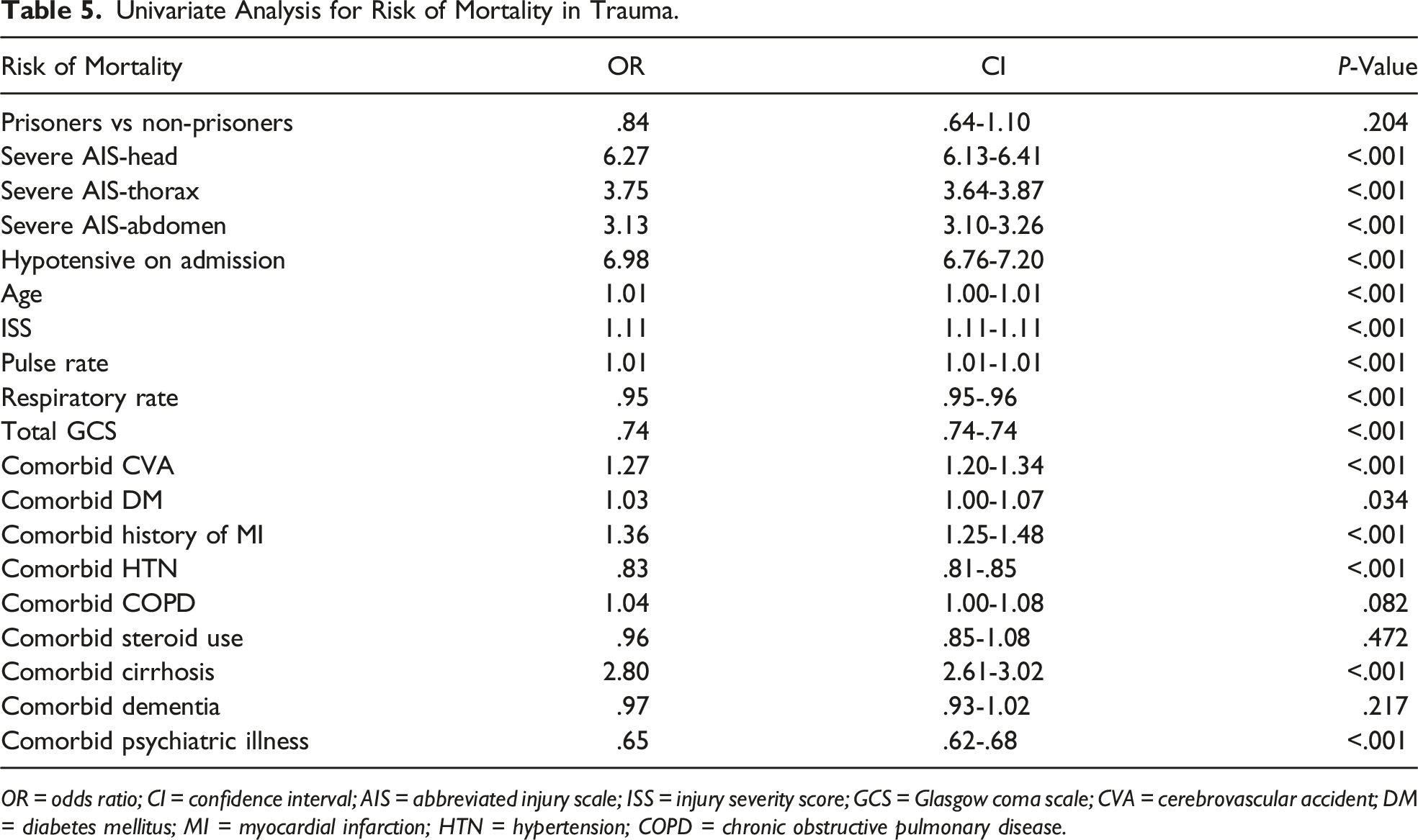
OR = odds ratio; CI = confidence interval; AIS = abbreviated injury scale; ISS = injury severity score; GCS = Glasgow coma scale; CVA = cerebrovascular accident; DM = diabetes mellitus; MI = myocardial infarction; HTN = hypertension; COPD = chronic obstructive pulmonary disease.
Multivariable Analysis for Risk of Mortality in Trauma.
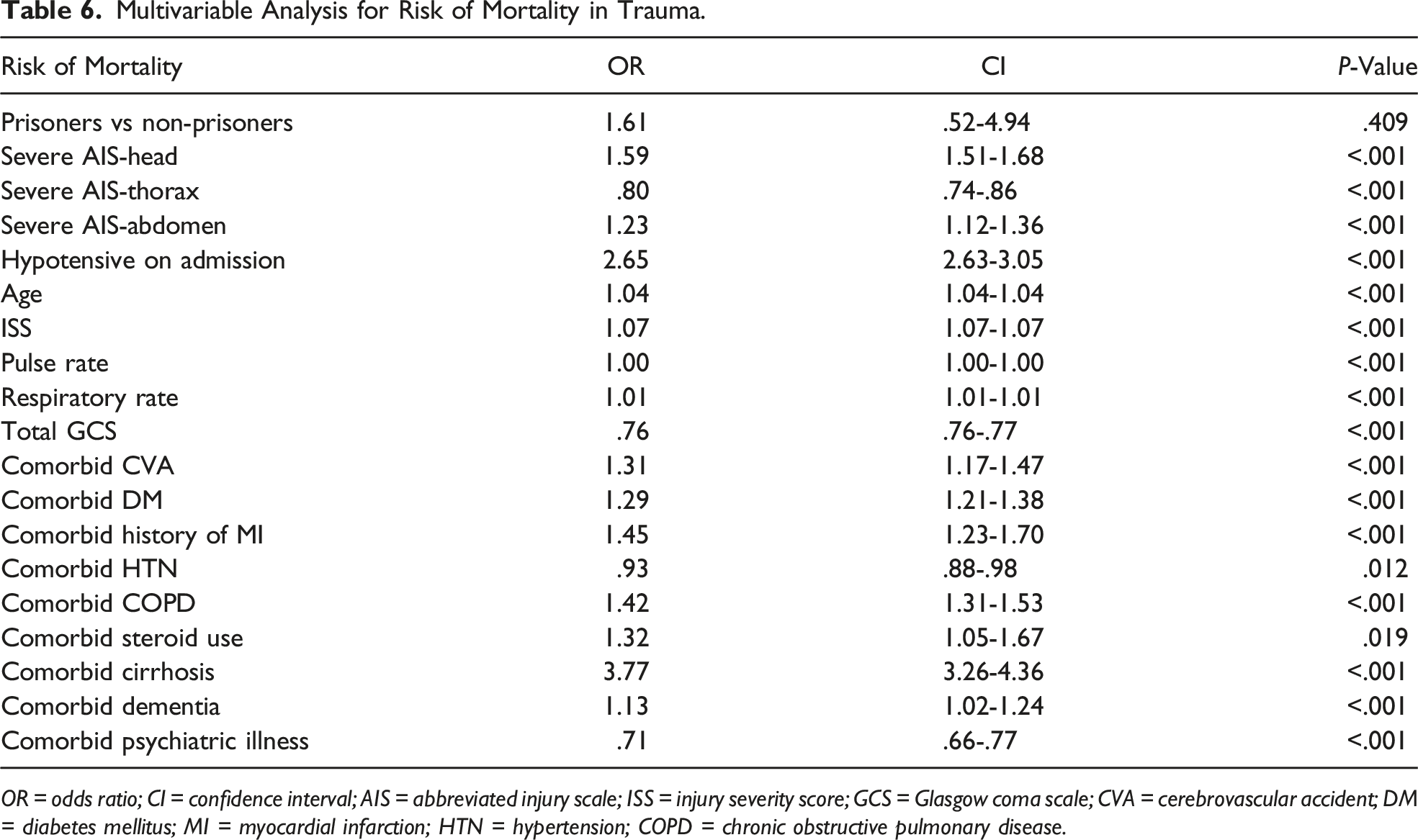
OR = odds ratio; CI = confidence interval; AIS = abbreviated injury scale; ISS = injury severity score; GCS = Glasgow coma scale; CVA = cerebrovascular accident; DM = diabetes mellitus; MI = myocardial infarction; HTN = hypertension; COPD = chronic obstructive pulmonary disease.
Discussion
In this large national TQIP analysis, we found that trauma patients presenting from a prison make up <.2% of all trauma patients and are more often younger, male minorities, and had fewer chronic medical comorbidities. In addition, we reported a similar rate and associated risk of mortality for trauma prisoners compared to non-prisoner trauma patients. Interestingly, our data demonstrated prisoners had lower rates of certain in-hospital complications, such as drug/alcohol withdrawal, PNA, and UTI compared to non-prisoners. Consistent with these findings, prisoners experienced decreased hospital LOS compared to non-prisoners. To our knowledge, this is the first paper that directly compares prisoner trauma patient mortality and non-prisoner trauma patient mortality using a large national population.
Prisoners represent a vulnerable population due to their limited autonomy and the social stigma associated with their incarceration.2,18 Previous studies have shown differing perceptions between the quality of treatment received by prisoners when compared to non-prisoners.19-21 Zust et al 18 found that nurses’ preconceived notions of inmates often negatively contributed to their ability to empathize with and care for their patients. 18 Prisoners may also be at increased risk of traumatic injury due to poor prison conditions. For example, Haber et al discussed how shackling can lead to an inability to break falls, increases the risk of thrombosis due to movement limitations, and has a negative association with empathy amongst many care providers. 2 However, despite potential preconceived inadequacies regarding the quality of care of prison patients, our national TQIP analysis found that prisoner trauma patients had no difference in rate and associated risk of mortality compared to their non-prisoner counterparts. Although not specific to trauma patients, multiple studies involving non-surgical prison patients demonstrated similar outcomes between prisoner and non-prisoner medical patients.22,23 Winter et al found no difference in mortality between inmates and non-inmates treated acutely for chest pain, and in fact demonstrated shorter time to first procedure for inmates (.46 days earlier). 22 Thus, it appears while qualitative metrics may have disparities, care in terms of objective outcomes is at least similar for prisoner patients.
Hospital LOS is an important metric both for quality of care, as well as associated healthcare cost. When treating trauma patients, each additional day of excessive hospital stay is associated with a 5% increase in risk of developing independent hospital-associated medical complications. 24 Furthermore, the estimated cost of each day of hospitalization ranges from an average of $645-$3500 depending on state and ownership of the hospital. 25 Our study found a decreased LOS for prisoners compared to non-prisoners. In congruence with our findings, previous studies have also demonstrated decreased LOS for prisoner populations.2,26 Although not specific to trauma patients, Haber et al found a significantly decreased LOS for incarcerated vs non-incarcerated patients (4 vs 5.6 days), with the largest sub-group of these patients (17.6%) being admitted for traumatic injuries. 2 One plausible explanation lies in the fact that the non-prisoner population often extends hospitalizations due to issues regarding discharge planning. For instance, Hwabejire et al found that only 20% of non-prisoner trauma patient discharge delays were clinical. 27 Looking at the remaining 80, 47% resulted because of difficulties in placement and 7% occurred due to payer-related issues. Given that prisoners have a clear discharge disposition, this may help explain their decreased LOS. Alternatively, a decreased rate of complications may be a driving factor for this discrepancy.
In support of this, we reported prisoners had significantly less drug/alcohol withdrawal, PNA, and UTIs. The decreased drug/alcohol withdrawal within the prisoner population is in spite of prior reports citing that prisoners continue to have access to, and use substances while in prison.1,28 Although we think it is more difficult to obtain a sufficient and steady supply of drugs in prison that would allow someone to withdrawal from these substances (ie, alcohol and opioids), we are unable to quantify this statement. However, non-prisoners had nearly double the rate of DM, which could help explain the increased rate for infections in the non-prisoner trauma patient population, as DM is a well-known risk factor for infection as demonstrated by Knowlin et al who demonstrated a higher incidence in both PNA (9.2 vs 6.3%) and UTIs (11 vs 3%) among diabetic trauma burn patients compared to non-diabetic trauma burn patients.29-32 Additionally, higher rates of COPD in the non-prisoner population may predispose them to a higher risk for PNA at baseline. Future prospective research is needed to elucidate the exact reasons for prisoners’ decreased rate of complications; however, it is reassuring that this vulnerable population appears to have fewer complications compared to the general trauma population.
Our study is susceptible to numerous limitations, such as those associated with performing a retrospective database study including missing data, reporting bias, and coding errors. Also, the populations compared in this study had numerous differences that we attempted to account for in our multivariable analysis; however, there may be other confounders that are missing within TQIP such as time to presentation from the prison or home-setting, baseline functional status, and baseline laboratory evaluations in the hospital. The database also does not allow us to identify the reason for and duration of incarceration, which may skew our data, as a prisoner for one day may have a different baseline medical status and outcomes than a prisoner of many years. Due to the fact that TQIP only includes verified trauma centers, some hospitals are not included. Injuries that are evaluated by an emergency medicine physician but not severe enough to warrant a trauma team evaluation are not included in the TQIP data set. Additionally, we assumed that traumas occurring in prison predominantly involve prisoners; however, our data simply identify the location of injury as a prison but does not specify whether the patient was a prisoner or non-prisoner (ie, correctional officer or visitor). Furthermore, we are unable to determine if any of the non-prisoners were previously prisoners, and we have an inability to account for socioeconomic differences in the populations. Since TQIP is limited to the index hospitalization, we also cannot evaluate any post-discharge and/or long-term outcome differences. Finally, while this study evaluates quantitative outcomes, qualitative outcomes cannot be measured and represent an area in need of future research. These include metrics such as patient expectations and experience which could be measured via interviews and/or focus groups as well as validated surveys such as the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) surveys. Despite these limitations, we believe this study will help foster further high-quality prospective multicenter research on this vulnerable population.
To our knowledge, this is the first large national analysis comparing outcomes of trauma patients presenting from prisons to non-prisoners. We reported that prisoners make up less than .2% of trauma patients. Supporting our hypothesis, we found no differences in the rate or associated risk for mortality between trauma patients from prisons compared to non-prisoners. Interestingly, prisoners had a shorter hospital LOS, as well as fewer complications. Future prospective studies are needed to confirm these results and explore additional areas of potential disparities such as qualitative outcomes.
Supplemental Material
sj-pdf-1-asu-10.1177_00031348221078984 – Supplemental Material for Comparative Outcomes for Trauma Patients in Prison and the General Population
Supplemental Material, sj-pdf-1-asu-10.1177_00031348221078984 for Comparative Outcomes for Trauma Patients in Prison and the General Population by AB Christian, A Grigorian, J Mo, EO Yeates, M, Dolich, TL Chin, SD Schubl, CM Kuza, M Lekawa and J Nahmias in The American Surgeon
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.