
Abstract
Background
The COVID-19 pandemic has required new treatment paradigms to limit exposures and optimize hospital resources, including the use of neoadjuvant endocrine therapy (NAET) as bridging therapy for HR+/HER2-invasive tumors and DCIS. While this approach has been used in locally advanced disease, it is unclear how it may affect outcomes in resectable HR+/HER2- tumors.
Methods
Women ≥18 years diagnosed with in situ (Tis) or non-metastatic HR+/HER2- breast cancer from March-May 2019 and 2020 were included. Fisher’s exact test and two-sample t test were used to compare baseline characteristics and surgical outcomes between strata. Sub-analysis was performed between patients who received primary surgery vs a bridging NAET approach.
Results
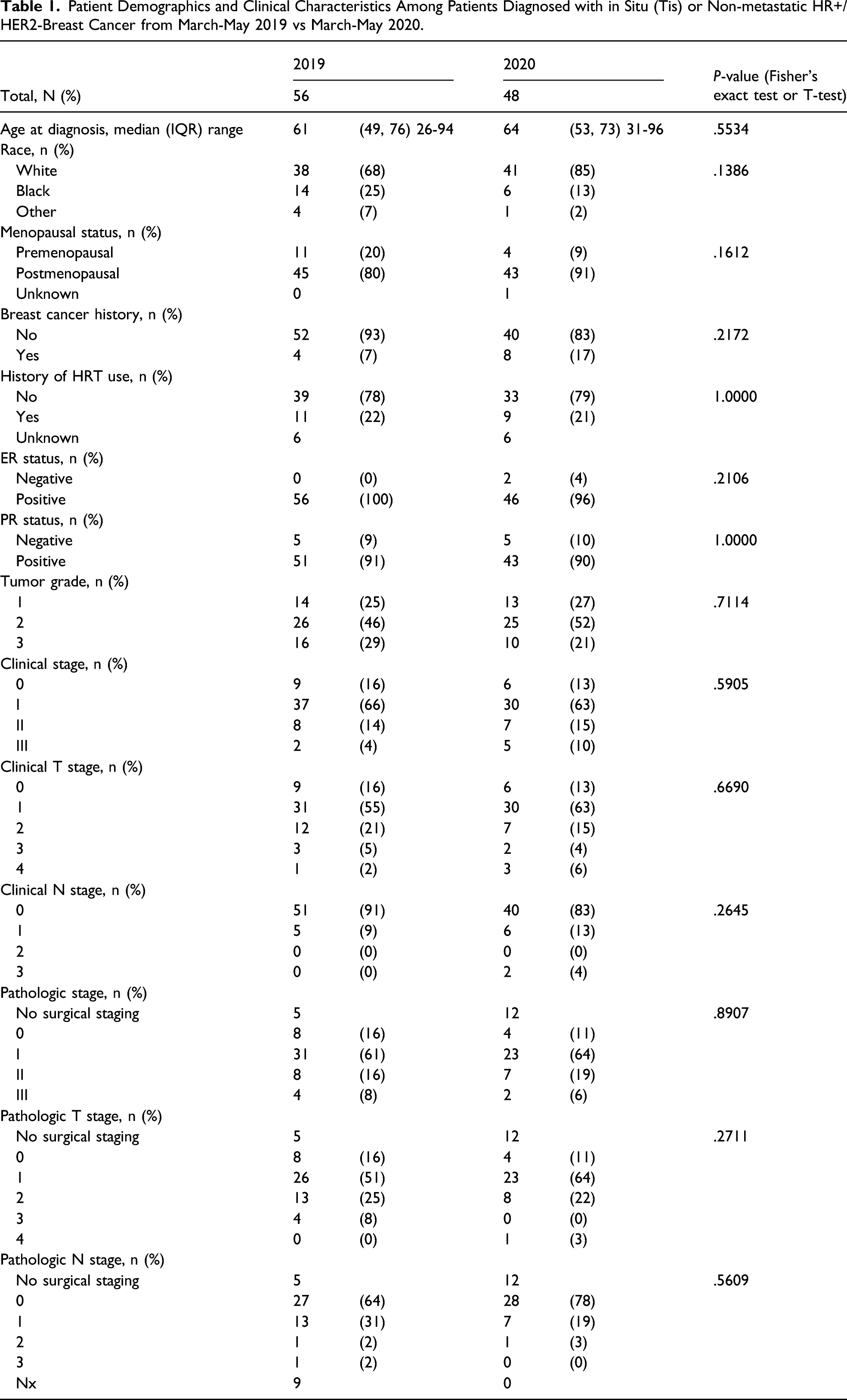
Despite similar clinical characteristics, patients in 2019 were more likely to have a surgery-first approach (75% vs 42%, P-value = .0007), receive surgery sooner (22 vs 29 days, P-value < .001), and within 60 days from diagnosis date (100% vs 85%, P-value = .0301). Neoadjuvant endocrine therapy was a more prevalent approach in 2020 (48% vs 7%, P-value < .0001). Rates of clinical to pathologic up-staging remained consistent across primary surgery vs bridging NAET subgroups (P-value = .9253).
Discussion
Pandemic-driven treatment protocols provide a unique opportunity to assess the utility of bridging endocrine therapy for resectable HR+/HER2- tumors. Differences in clinical and pathologic staging were similar across groups and did not appear to be affected by receipt of NAET. Our limited cohort demonstrates this strategic therapeutic avenue can optimize health care utilization and may be a reasonable approach when delaying surgery is preferred.
Keywords
Key Takeaways
Pandemic treatment protocols provide a unique opportunity to assess the safety of bridging endocrine therapy for HR+/HER2- invasive cancer in women with resectable tumors. Despite delays to surgery, women treated with bridging neoadjuvant endocrine therapy did not exhibit higher rates of pathological up-staging when compared to a case-matched population treated under pre-pandemic standard of care guidelines.
Introduction
In December 2019, a novel coronavirus, SARS-CoV-2 (COVID-19), was identified in Wuhan, China, and quickly spread globally. With its rapid human-to-human transmission and devastating consequences, including acute respiratory distress syndrome, the World Health Organization (WHO) officially declared the outbreak a pandemic and global health emergency.1-3 Due to the immunosuppressive effects of malignancies, surgery, and chemotherapeutic agents, cancer patients were identified as a particularly susceptible patient population to COVID-19 with infection resulting in increased morbidity and mortality than the general population. 4 Clinicians were now faced with an unseen challenge—balancing the risk of potential COVID-19 infection vs the risk of delayed cancer treatment for their patients.
In March 2020, the American Society of Breast Surgeons (ASBrS) and Society of Surgical Oncology (SSO) issued pandemic-driven guidelines to aid clinicians in prioritizing care for their breast cancer patients. Specifically, priority categories were defined based on disease severity and potential efficacy of treatments, and the use of neoadjuvant endocrine therapy (NAET) was recommended as first-line therapy for newly diagnosed hormone receptor positive (HR+) cancers and in situ disease for both premenopausal and postmenopausal women.5-7 In an effort to limit exposures and optimize hospital resources, the multidisciplinary breast cancer team at University of North Carolina Hospitals at Chapel Hill, NC, responded by immediately enacting treatment and surveillance guidelines as detailed by ASBrS and SSO recommendation.
Limited data has been published comparing outcomes of patients who received care under pandemic guidelines to standard of care prior to the COVID-19 outbreak. While the use of neoadjuvant endocrine therapy as a bridging therapy has been validated in locally advanced estrogen receptor positive (ER+)/human epidermal growth factor negative (HER2-) tumor subtypes in postmenopausal women,8,9 NAET efficacy in resectable estrogen receptor positive (ER+) breast cancers remains unclear.10,11 In this analysis, we investigate variances in therapeutic approach for breast cancer patients who were diagnosed during the COVID-19 pandemic to determine if hospital resource constraints had impact on time to definitive surgery and pathologic cancer staging. In a sub-analysis, we evaluate differences in early patient outcomes between women treated with bridging endocrine therapy compared to a surgery-first approach.
Methods
Study Design and Objectives
All women ≥18 years old diagnosed with in situ (Tis) or non-metastatic HR+/HER2- breast cancer from March to May 2020 at the University of North Carolina (Chapel Hill, NC) were included. This time frame was intentionally selected to observe treatment regimens driven by pandemic-related status and availability of hospital resources. A second study population of women ≥18 years old diagnosed with in situ (Tis) or non-metastatic HR+/HER2- breast cancer from March to May 2019 at the University of North Carolina (Chapel Hill, NC) was included as a case-matched control cohort to make comparisons in patient demographics, clinical characteristics, and treatment protocols to a pre-pandemic baseline. Chart review was completed through January 31, 2021.
The intent of this study was to (1) examine differences in treatment regimens for breast cancer in 2020 vs 2019 and (2) evaluate if treatment protocol, specifically bridging endocrine therapy vs a surgery-first approach, affected early patient outcomes. Secondary outcome was number of days until definitive surgical treatment.
For patients who received a cancer operation, early patient outcomes were defined by comparing clinical to pathologic cancer staging. Patients were classified as “up-staged” if pathologic tumor or nodal status was greater than clinical tumor or nodal status. Similarly, patients were classified as “down-staged” if pathologic tumor or nodal status was less than clinical tumor or nodal status.
Statistical Analysis
Descriptive statistics were employed given limited sample size. The Fisher’s exact test and two-sample t test were used to compare baseline patient and tumor characteristics and surgical outcomes between the 2019 and 2020 strata. Sub-analysis was performed between patients who received surgery first vs bridging endocrine therapy in 2020.
All analyses were performed using SAS version 9.4 (SAS Inc, Cary, NC). All tests were two-sided at alpha = .05 with P < .05 considered statistically significant. The University of North Carolina Institutional Review Board deemed this study exempt (IRB# 20-1408).
Results
Patient and Tumor Characteristics
Patient Demographics and Clinical Characteristics Among Patients Diagnosed with in Situ (Tis) or Non-metastatic HR+/HER2-Breast Cancer from March-May 2019 vs March-May 2020.
Treatment Protocols and Early Outcomes
Treatment Regimens and Post-surgery Cancer Staging Among Patients Diagnosed with in Situ (Tis) or Non-metastatic HR+/HER2- Breast Cancer from March-May 2019 vs March-May 2020.
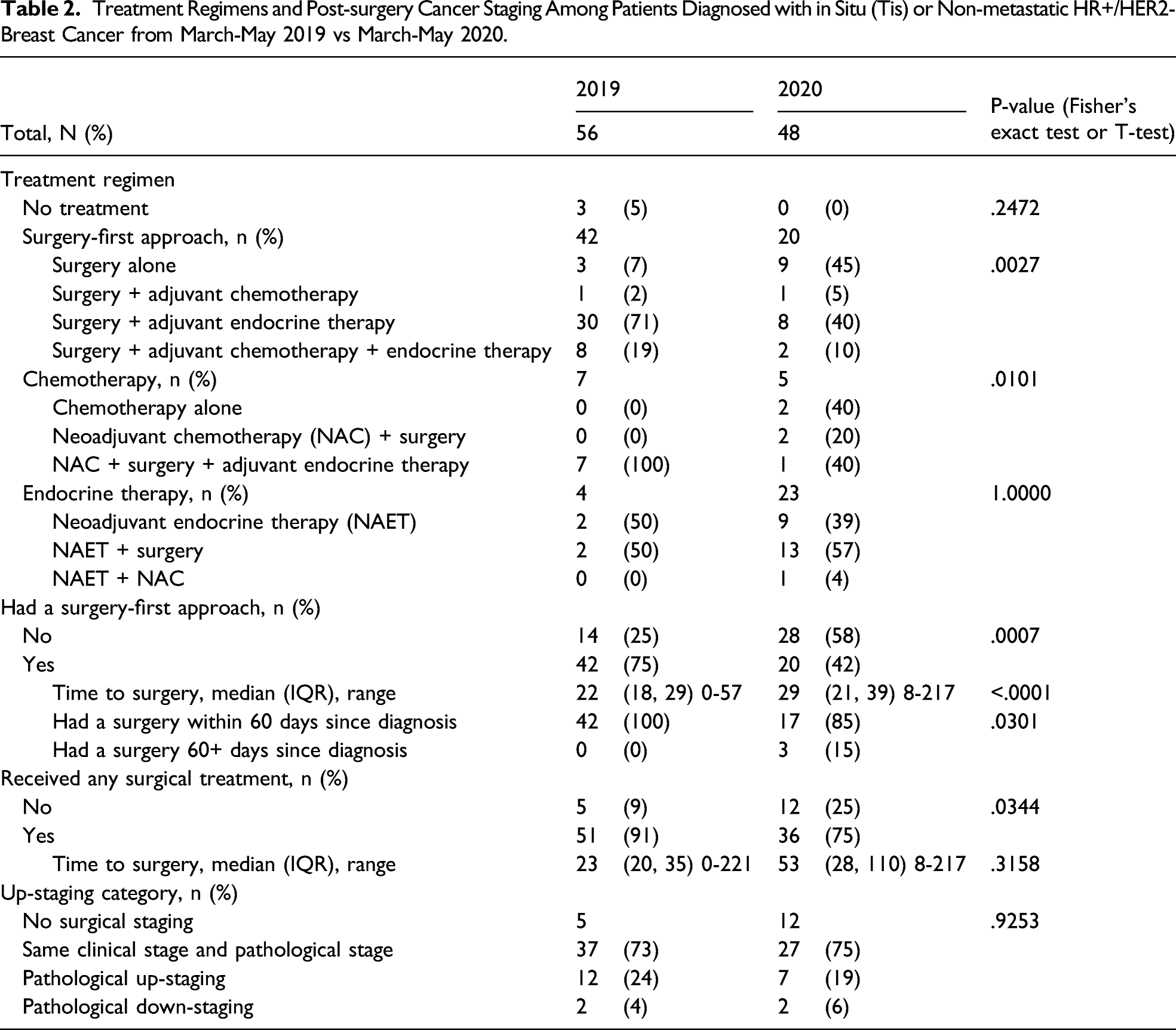
Women treated in 2019 were more likely to receive a breast cancer operation than their 2020 counterparts (91% vs 75%, P-value = .0344). Time to surgery was longer in the 2020 cohort (median 53 days vs 23 days); however, this was not statistically significant (P = .3158).
Despite differences in treatment protocols across 2019 and 2020 cohorts, rates of clinical to pathologic up-staging remained consistent (P-value = .9253). Most patients had no difference in cancer staging after surgery, less than a quarter had pathological up-staging (24% in 2019 and 19% in 2020), and even fewer had pathological down-staging (4% and 6% in 2019 and 2020, respectively).
Bridging Endocrine Therapy vs Surgery-First Approach
Patient Demographics and Clinical Characteristics Among Patients Undergoing Surgery First vs Bridging Endocrine Therapy from March-May 2020.
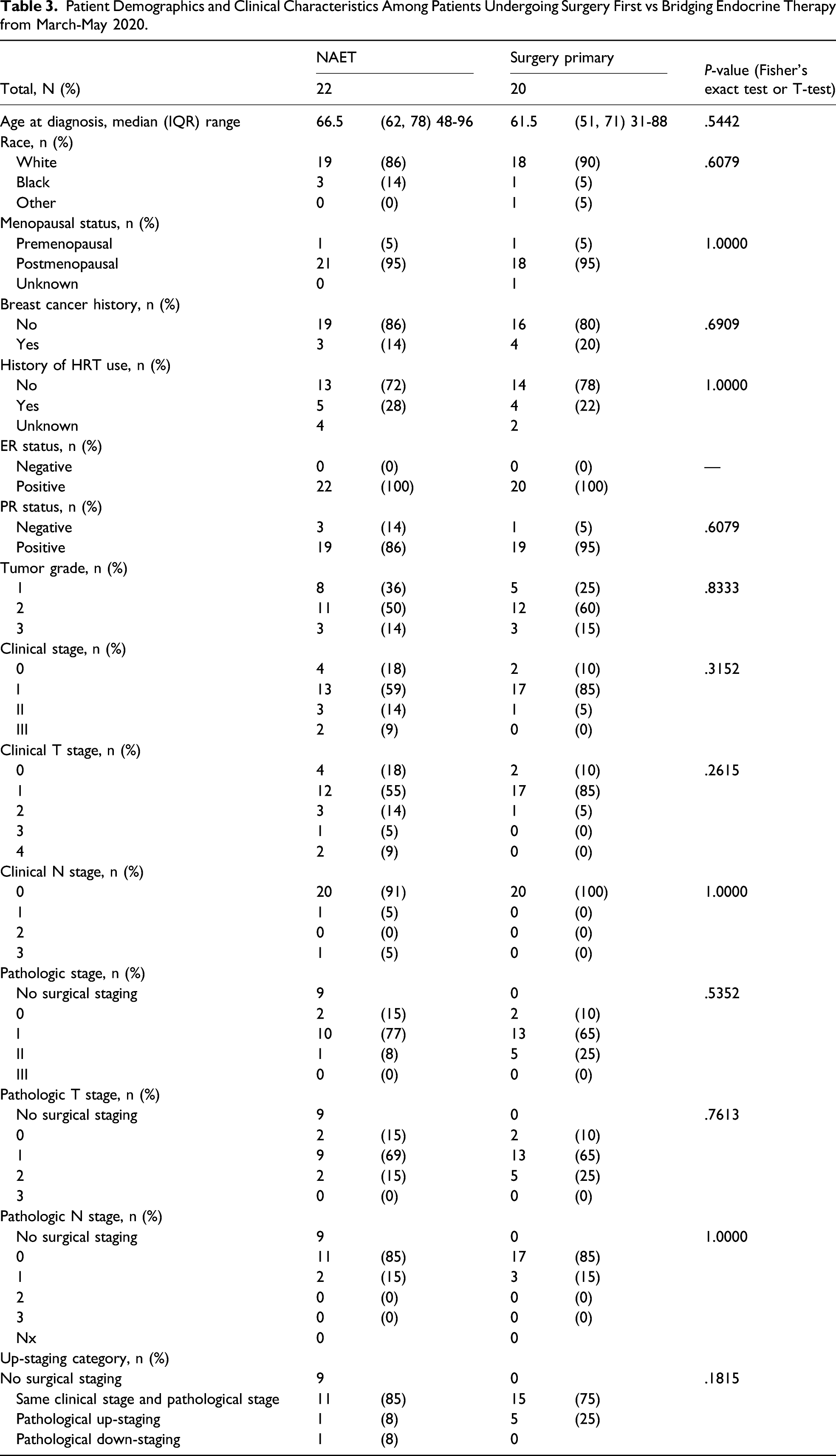
In 2020, 20 (42%) patients had a surgery-first approach, 22 (46%) received bridging endocrine therapy, and 6 (13%) received neoadjuvant chemotherapy. Overall, 36 (75%) patients received definitive surgical treatment by January 2021. At time of diagnosis, 6 (13%) had Tis disease, 30 (63%) had stage I disease, 7 (15%) had stage II disease, and 5 (10%) had stage III disease.
Among the 22 women who received bridging endocrine therapy, 13 (59%) had received surgery by January 2021. Median time to surgery was 73 days (IQR 52-105, range 27-148 days). 11 had the same pre-surgical clinical stage and pathologic stage, 1 had pathological up-staging (stage IA to IIA), and 1 had pathologic down-staging (stage IIA to IA). Median time to surgery in the surgery-first cohort was shorter at 29 days (IQR 21-39, range 8-217). Notably, 5 (25%) of these women had pathologic up-staging (4 from stage I to II and 1 from stage IIA to IIB) and 15 (75%) had the same pre-surgical clinical stage and pathologic stage.
Discussion
We have shown that women diagnosed with in situ or non-metastatic HR+/HER2- breast cancer received different therapeutic regimens when treated during the peak of the COVID-19 pandemic as compared to a case-matched control cohort from 2019. Despite similar patient characteristics among strata, primary surgery followed by adjuvant therapy was the predominant treatment for women in 2019, while bridging endocrine therapy was the principal modality used in 2020. Unsurprisingly, women treated in 2020 had longer wait times to definitive surgery and were less likely to receive surgery overall. Despite delays to surgery, women treated for their breast cancer under the health care constraints of COVID-19 did not exhibit higher rates of pathological up-staging when compared to a case-matched population treated under pre-pandemic standard of care guidelines.
The American College of Surgeons Oncology Group (ACOSOG) Z1031 trial demonstrated that receipt of NAET led to increased rates of breast conservation in patients with locally advanced ER+ invasive carcinoma. 12 Several studies investigating tamoxifen use in postmenopausal patients with resectable hormone receptor positive tumors support that bridging endocrine therapy should not affect breast cancer–specific survival.13-15 This therapeutic approach has previously been utilized to down-stage tumors and delay local progression for many months to years without consequence. 16 The results of our 2020 sub-analysis corroborate this statement, yielding no statistically significant differences in early patient outcomes for women treated with bridging endocrine therapy compared to a surgery-first approach. In a meta-analysis by Spring et al, neoadjuvant endocrine therapy was found to have similar response rates as chemotherapy, and with less toxicity, in women with ER + resectable breast cancer. 17 Nonetheless, NAET use for HR + breast cancer in the United States remains limited. A previous study examining the National Cancer Database demonstrated that only 3% of potentially eligible patients received NAET prior to the COVID-19 pandemic–related treatment regimen changes. 18 With pandemic guidelines yielding increased use of bridging NAET, this study adds to the growing body of evidence assessing the efficacy of this treatment protocol and supporting routine use in particular patient cohorts.
In contrast to our analysis, other investigations have found delays to surgery, with or without use of bridging endocrine therapy, results in mixed patient outcomes. An analysis examining impact of surgical delay in stage I-III invasive breast cancers found that less than 20% of tumors not selected for neoadjuvant chemotherapy had tumor progression with surgical delay >60-<294 days. 19 Notably, there was no nodal progression with surgery delay and luminal B phenotype was the only clinical predictor of tumor growth. In a recently published meta-analysis by Johnson et al examining survival and pandemic-driven delays to surgery, surgery postponement ≥12 weeks resulted in decreased overall survival in women with stage I/II breast cancer. 20 A recent investigation of breast cancer patient outcomes in cases who received diagnosis during the pandemic found these women had more advanced tumor size and nodal status. This resulted in increased adjuvant therapy use in comparison to patient counterparts treated pre-pandemic. 21
These varied outcomes question whether particular patient or practice factors apart from treatment paradigms may be driving outcomes. It is unclear from this analysis if pandemic-driven delays to surgery may exacerbate disparities in surgical management already present in particular ethnic/racial populations. Heightened clinician awareness of those affected by social determinants of health will continue to be of undoubted importance, especially in patient populations who have previously exhibited higher rates of endocrine therapy nonadherence.22,23 With new viral variants threatening to impact health care utilization once again, we suspect there will be continued and perhaps increased barriers to care for cancer patients given financial constraints from job loss, insurance status, and distance from treatment facility related to the pandemic. 24 In a national survey of breast cancer survivors treated during the pandemic, almost half of the women felt their cancer care had been hindered by the pandemic, with younger women reporting a disproportionate burden of treatment delay. 25 This patient perspective emphasizes the importance of patient-provider communication and informed discussion of therapies distinct from previously outlined treatment plans.
As with all retrospective studies, this analysis is dependent on reliance of accurately recorded data. It is important to note that our outcomes reflect only patients who received care at our institution and follow-up is limited to January 31, 2021. It is possible patients may have sought care at other institutions in hope of receiving surgery at an earlier date. Certain study measures such as receipt of a cancer operation and timing to surgery may be impacted when chart review is completed again. Data from this analysis are based on observations from a single institution; however, it is likely representative of all centers that treated patients under the pandemic guidelines outlined by Society of Surgical Oncology and American Society of Breast Surgeons. Given limited time duration between patient diagnosis and this analysis, we are only able to comment on early outcomes of breast cancer patients who received care during the COVID-19 pandemic. In future analysis, we plan to re-examine these cohorts (2020 and 2019) for differences in other patient outcomes, including disease-free survival. We are particularly interested in the cohort of women who were placed on bridging NAET under pandemic guidelines. If these women continue to have favorable response to this treatment regimen, this may result in later date to cancer operations outside of health care resource limitations.
Pandemic treatment protocols provide a unique opportunity to assess the safety of bridging endocrine therapy for HR+/HER2- invasive cancer in women with resectable tumors. Differences in clinical and pathologic staging were similar across groups and did not appear to be affected by receipt of NAET. While surgical excision will likely remain standard of care for in situ and early-stage disease outside of resource limitations, pandemic paradigms such as endocrine chemoprevention provide flexibility to providers treating breast cancer patients in trying environmental conditions. Our limited cohort demonstrates this strategic therapeutic avenue can optimize health care utilization, and also can be applied to future situations in which delaying surgery may be preferred. As with all oncology care, treatment protocols should be tailored with consideration of not only hospital resources but also patient and tumor factors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.