
Abstract
Anastomosing hemangiomas (AH) are rare benign masses. We report an occurrence of AH in the breast during pregnancy, its pathological analysis, and clinical management. Key in the evaluation of these rare vascular lesions is differentiating AH from angiosarcoma. A low proliferative Ki-67 index and small size on imaging and final pathology will confirm AH from angiosarcoma. Clinical management of AH requires surgical resection and standard interval mammography and clinical breast examination.
Keywords
Anastomosing hemangiomas (AH) are rare benign vascular lesions that closely resemble angiosarcomas. 1 Historically, AH are found in the genitourinary system; however, they have been reported less frequently in other areas of the body. At this time, there are only two cases of AH reported in the breast. The goal of this case report is to help identify distinctions between AH and low grade angiosacromas found in the breast as therapeutic management differs significantly between these benign and malignant lesions. Consent was obtained in accordance with the treating institution guidelines.
We report a case of a 37-year-old female who presented with a tender, palpable 10 mm right breast mass at the 12:30 position, 18 cm from the nipple. Of note, the patient identified the mass during pregnancy. Initial work-up began with diagnostic imaging, which demonstrated a mass with irregular borders with internal echogenicity on mammogram and ultrasound. Of note there was no distortion or spiculation on imaging. A core needle biopsy was recommended. The biopsy (Figure 1A-D) demonstrated a well-circumscribed vascular lesion (Figure 1A, arrowheads) composed of interconnecting capillary-sized vascular channels (Figure 1B-C) with features that suggest extramedullary hematopoiesis. The cells of the lesion were immunoreactive for vascular markers including ERG (Figure 1D, 200X) and the Ki-67 index was low (5%). No atypia, malignant cells, necrosis, or increased mitotic activity were identified. In order to definitively differentiate between an AH and a well-differentiated low-grade angiosarcoma, we proceeded with an excisional breast biopsy in the operating room. Low power images of the resection specimen further confirmed the well-circumscribed nature of the tumor (Figure 1E, arrowheads). A 4.5 mm benign AH was reported on final pathology. The patient recovered well and required no further management until her normal screening mammography at age 40. Composite displaying the histomorphologic and immunohistochemical features of the lesion as seen in the core biopsy (A-D) and subsequent excision (E and F). Figure A exhibits a low power view of the lesion with a well demarcated border (arrowheads) separating it from the adjacent adipose tissue. Medium-power and high-power views of the lesion in Figures B (H&E, 200X) and C (H&E, 400X) demonstrate that the tumor is composed of anastomosing capillary sides vascular channels lined with endothelial cells with uniform, slightly hyperchromatic, nuclei with focal hobnail pattern in addition to focal intravascular fibrin microthrombi (C, circles). The cells of the lesion were immunoreactive for vascular markers including ERG (D, 200X). Low power images (H&E, 20X) of the resection specimen further confirmed the well-circumscribed nature of the tumor (E, arrowheads) and showed changes of the prior procedure (E, asterisks) with the lesion showing the same histomorphologic features (F, H&E, 100X).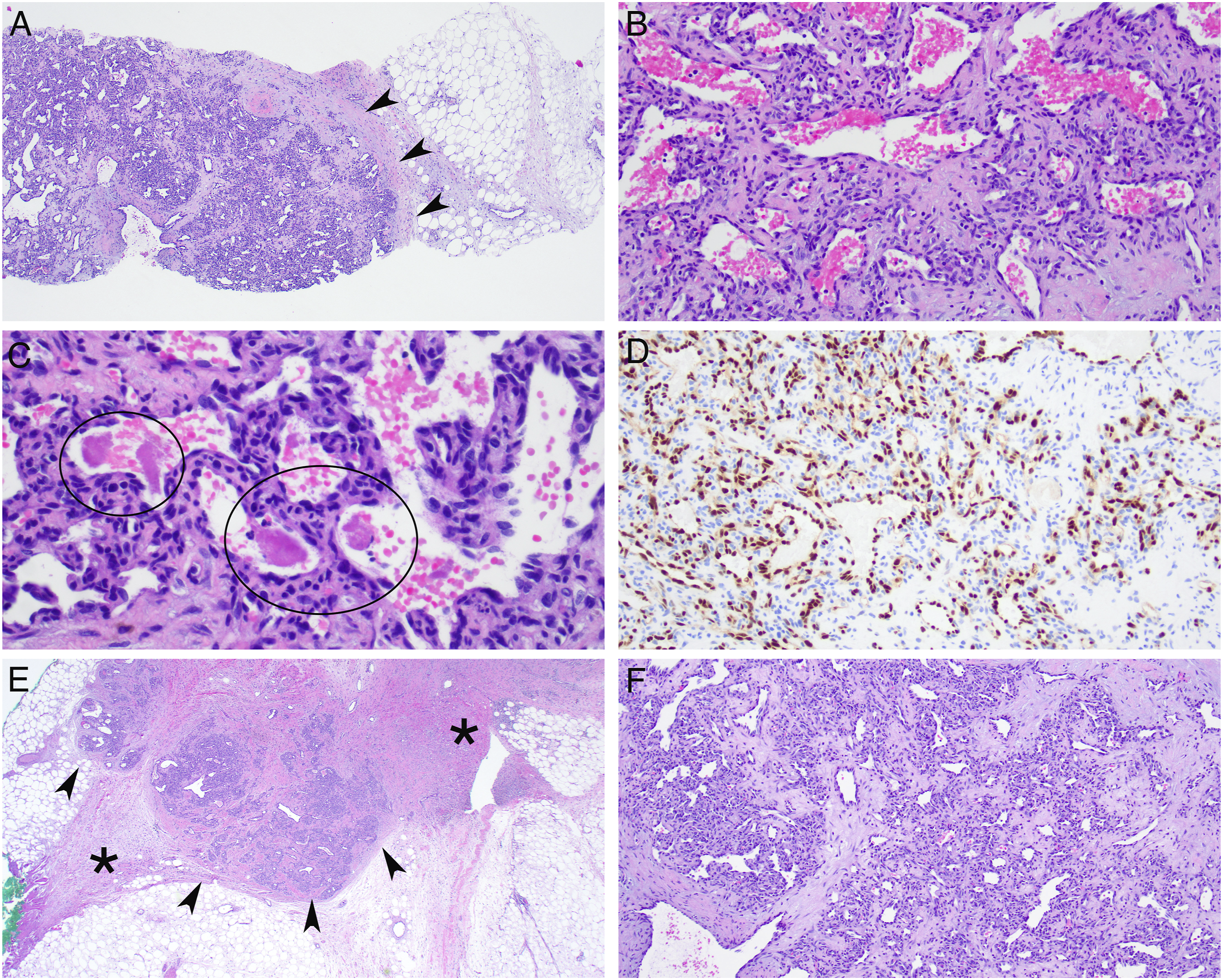
When comparing our presentation of a benign AH, angiosarcomas are typically larger in size (often greater than 2 cm), have a higher proliferative Ki-67 index, and are typically more infiltrative, which causes significant distortion in the normal breast architecture. 2 In a case by Varghese et al, an angiosarcoma initially identified as a cavernous capillary hemangioma had a Ki-67 index of 20-40%. 3 This case highlights the importance of defining the proliferative index when differentiating between a benign AH and angiosarcoma.
Although AH commonly presents in the genitourinary system, there have been more recent cases reported in the breast, and there continues to be limited literature discussing factors that stimulate AH formation. Furthermore, it is important to investigate for any pregnancy-related or hormonal-related physiologic features that can stimulate the formation of this vascular lesion. Extramedullary hematopoiesis (EMH) is not always present in AH, but literature of renal AH has reported features of EMH in individuals with polycythemia and end-stage renal disease. A similar process of EMH occurs in pregnancy due to the increasing demand of maternal blood volume to support the fetus, which involves an interaction of metabolic and hormonal mechanisms to activate hematopoietic stem cells and EMH. 4 Further investigation should be completed to determine any hormonal and extramedullary hematopoietic factors influencing AH formation or growth.
The differentiation of AH and angiosarcoma is crucial for management. If the excisional biopsy were to return as an angiosarcoma, this would require a multidisciplinary team approach, and the subsequent treatment would be influenced by tumor size, grade, and overall staging of the patient. On the contrary, in a patient with breast AH, once the patient was confirmed to have a benign disease process on excisional biopsy, she did not require any further management beyond regular breast cancer screening guidelines. This highlights the importance of an excisional breast biopsy for small lesions where the differentiation between a benign AH and an angiosarcoma cannot be determined by core needle biopsy alone.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.