
Abstract
Babies in the United States fare worse than their peers in other high-income countries, and their well-being is starkly unequal along socioeconomic and racialized lines. Newborn health predicts adult well-being, making these inequalities consequential. Policymakers and scholars seeking to improve newborn health and reduce inequality have recently looked to direct cash transfers as a viable intervention. We examine the only unconditional cash transfer in the United States, the Alaska Permanent Fund Dividend (PFD), to learn if giving pregnant people money improves their newborns’ health. Alaska has paid its residents a significant dividend annually since 1982. The dividend’s size varies yearly and is exogenous to Alaskans and the local economy, permitting us to make causal claims. After accounting for fertility selection, we find that receiving cash during pregnancy has no meaningful effect on newborn health. Current theory focuses on purchasing power and status mechanisms to delineate how money translates into health. It cannot illuminate this null finding. This case illustrates a weakness with current theory: it does not provide clear expectations for interventions. We propose four components that must be considered in tandem to predict whether proposed interventions will work.
Health at birth is a strong indicator of later health and well-being: birth outcomes have long-term economic and health consequences, including effects on infant mortality, academic performance, and adult income (Barr, Eggleston, and Smith 2022; Conley, Strully, and Bennett 2003; Currie 2009). Even at this “starting gate,” the U.S. social structure is apparent, reflecting systems of inequality and power (Conley et al. 2003). Children’s health at the start of life is highly correlated with their parents’ finances (Chen, Oster, and Williams 2016; Olson et al. 2010). Across income levels, infants born to parents of color have worse health (Forde et al. 2019; Geronimus 1992). In the United States, inequality is embodied at birth.
Acknowledging the importance of early life, federal and state governments have tried to promote newborn health. Nonetheless, the United States lags behind other high-income nations in this regard (OECD 2017). Common and long-standing interventions that try to improve newborn health have targeted proximate causal mechanisms, such as nutrition during pregnancy or access to prenatal care. For instance, the Women Infant and Children program (WIC), perhaps the most well-known program with this focus, provides eligible pregnant, postpartum, and breastfeeding people and their children supplemental nutritious foods as well as access to health screenings and nutrition counseling (USDA 2023).
Of late, however, policy proposals have increasingly called for providing participants with cash rather than services, goods, or near-cash benefits like Food Stamps. The logic undergirding these calls is that families know best what they need, and providing unrestricted income gives them the autonomy and dignity to craft their own futures using the same resources (i.e., unconditional cash) wealthier people use to secure their well-being (Shah and Neighly 2022). Furthermore, providing cash can lower the administrative burden on both program participants and administrators while supporting reproductive autonomy (SisterSong 2023). With this in mind, philanthropic institutions and city governments have begun pilot studies to distribute cash to pregnant people (California Preterm Birth Initiative 2024; City and County of San Francisco, Office of the Mayor 2020; Hellman 2023; Malawa, De La Cruz, and Karasek 2021; Newman 2022; Perigee Fund 2022).
Here we ask: what effect, if any, does providing additional income during pregnancy have on infant health? Central to that question is another: what can money buy? Answering these questions requires isolating the effects of money from the effects of how we typically go about getting money. In short, we need an exogenous source of income. In this article, we examine a universal cash transfer in Alaska—the Alaska Permanent Fund Dividend (PFD). We exploit it to gain insight on the potential of cash transfers as an intervention to improve newborn health. The PFD is a state program that has made a yearly cash payment from Alaska’s sovereign wealth fund to every Alaskan resident, with few exceptions, since 1982.
We make causal claims on the basis that the value of the PFD payment is not predictable by individual Alaskans’ behavior or the local economy (Hsieh 2003; Kueng 2018). We provide more detail on the case below, but, in short, the size of the distribution is dictated by statutory formula that siphons a portion of the fund’s revenue to pay these dividends (McGee 2020). The amount of the transfer is substantial, typically exceeding the value of the standard U.S. social safety net, including the Supplemental Nutrition Assistance Program (more commonly known as Food Stamps) and the Earned Income Tax Credit (EITC) for a family of four.
We find very small, negative effects of a cash influx during pregnancy on birth outcomes after accounting for how the dividend affects who selects into giving birth. Additional analyses suggest these negative effects may be due to increases in births to parents who are at higher risk for poor birth outcomes based on non-demographic traits not empirically accounted for in our selection model. This evidence suggests that income improves the in-utero environment, allowing a small number of higher-risk fetuses to be conceived and survive to birth who otherwise would not. Yet our results indicate that cash transfers made during pregnancy—at least of the size disbursed through the PFD program—have no substantively meaningful effect on birth outcomes.
Why did these cash payments not improve newborn health? Based on present theory we cannot say. This is a problem. We want and need our theory to inform interventions; well-crafted interventions are informed by both theory and empirics.
Despite robust findings showing the connection between socioeconomic position and health, we know less about the particular mechanisms linking different types of socioeconomic resources to various health outcomes, a critical requirement for formulating policies to reduce these inequalities (Herd, Goesling, and House 2007). The field has delineated two primary mechanisms by which socioeconomic resources and status influence health. One mechanism is the purchasing power of money to acquire salubrious materials to reduce health risks in a capitalist economy. The second mechanism is status; rather than material resources, some scholars argue, it is the ongoing stress of living on the margins that degrades health.
Our theoretical intervention is three-fold. First, we assess the strength of empirical support for the two sets of theorized mechanisms. We find that abundant evidence supports these mechanisms, but their relative importance for particular health processes and outcomes is unknown. We then discuss why the empirics to illuminate this information have eluded us to date and how that impedes theoretical advancements. This serves as motivation for our case. Finally, we discuss prediction of effective interventions and propose four components that must be considered in tandem: (1) the type of resource, (2) the size of the resource, (3) whether providing the resource affects other causes of population health, and (4) the timing of the resource relative to the health process and outcome. Our work suggests we need to know more both empirically and theoretically to design interventions to equalize the starting line.
Theorizing the Effect of Cash During Pregnancy
Two Types of Mechanisms: Social Status and Purchasing Power
Numerous theories articulate how income translates into health. The two primary pathways identified by these theories are social status and purchasing power. That is, social structures shape how highly people are perceived or regarded and who gets what resources.
Status theory specifies how social status, separate from monetary inequalities, can result in health disparities. The theory was borne out of studying the British civil service which, despite being demographically homogenous, had a social status health gradient (Marmot 2005; Marmot, Shipley, and Rose 1984; Marmot et al. 1991). Weathering theory describes the problem as one of “the physiological effects of living in marginalized communities” (Geronimus 2023:10). We also see the effects of status in studies of threats to group status. Indirect threats during pregnancy to marginalized people, including legal and rhetorical threats, harm newborn health (Gemmill et al. 2020; Gemmill et al. 2019; Lauderdale 2006; Novak, Geronimus, and Martinez-Cardoso 2017; Samari et al. 2020; Torche and Sirois 2019). In the reverse direction, birth outcomes improve when group status improves (Moinester and Stanhope 2024; Torche and Rauf 2021).
Mechanisms related to purchasing power, as opposed to social status, focus on what money can buy. Fundamental cause theory (FCT) is the most popular theory in this vein, although FCT is not solely focused on purchasing power. As originally articulated, FCT posited that individuals with more socioeconomic resources are able to secure better health than people with fewer resources because they can more effectively use flexible resources to avoid health risks and access protective health measures (Link and Phelan 1995; Phelan and Link 2015). Flexible resources are defined as knowledge, money, power, prestige, beneficial social connections, and freedom.
FCT’s set of flexible resources originally spanned mechanisms that would influence both purchasing power (money) and status (prestige) as well as others that fall somewhere in between these poles—knowledge, power, freedom, and beneficial social connections. FCT has expanded to include racism, racial capitalism, and stigma as additional fundamental causes of health inequality (Hatzenbuehler, Phelan, and Link 2013; Phelan and Link 2015; Laster Pirtle 2020). Because flexible resources are just that—flexible—the theory predicts that advantaged people can use their resources to maintain better health when faced with new diseases and new health contexts.
Theory has delineated clear mechanisms by which socioeconomic status affects health. But we do not know how to fully translate this knowledge into interventions. Theory gives us a sense of how to intervene—with flexible resources based in purchasing power and in status. It also gives us some insight into when to intervene, where we turn next.
The Matter of Time
Translating material or status resources into health is also a matter of timing. Timing depends on one’s position in the social structure and one’s health trajectory over the life course. Weathering, cumulative (dis)advantage, and life course theories describe how early insults, or instances of psychological or physical damage, can have large ramifications.
Geronimus (1992) originally described the weathering theory to explain Black-White disparities in infant mortality. She argued that accelerated aging among the Black population from the cumulative stress of living on the margins, and the energy required to cope with repeated degradation, produced racialized health inequalities (Geronimus et al. 2006). Empirical investigation of a wide array of health outcomes for racialized minorities, and for poor people compared to non-poor people, supports the weathering hypothesis (Dennis 2019; Fishman 2020; Forde et al. 2019).
Relatedly, cumulative disadvantage/advantage theory, originating with Merton’s (1968) and Zuckerman’s (1965) Matthew effect, describes how early-life health advantages and disadvantages grow over time and compound, resulting in greater inequalities at later ages than at the start of life. This framework highlights the temporal nature of health processes and the long-term effects of some risk factors beyond the period they are experienced.
Life course perspectives draw our attention to how health processes unfold over time and the windows during which harmful exposures are particularly potent (Jones et al. 2019). Some insults may be overcome through a “countervailing mechanism,” whereas others produce permanent effects and therefore may require “risk-factor elimination” (Ferraro and Kelley-Moore 2003). Some exposures are more damaging at particular times, and the timing of an intervention should take that into account (Preston et al. 2003).
The Problem of Prediction
Where do these various theoretical approaches leave us in understanding the effect of a universal cash transfer during pregnancy on birth outcomes? If we were to lean heavily on purchasing power, then we would predict that an influx of cash, a flexible resource, would improve health. However, the FCT does not consider the timing and context within an individual’s life course. It does not answer the following question: when in a person’s life course would it be more or less efficacious to intervene for a particular health outcome? Perhaps the income is enough, but it comes too late. Or, if we were to lean heavily on status theory, then we would expect an influx of income that does not change the social hierarchy would not affect health.
We do not know how heavily to weigh purchasing power versus status. Nor do we know when would be the best time to intervene to interrupt a pathway toward poor newborn health. Despite significant and important theorizing about the effects of socioeconomic status and marginalization on health, our current theories cannot help us predict which interventions to improve newborn health will work better than others. For most health outcomes, including newborn health, we do not know enough about how income works to make sound predictions (Herd et al. 2007).
We contend that our theories cannot provide us with better instruction because they are rarely tested against each other or even in isolation, so we have no understanding of how they relate dynamically. This is a tall order because large-scale interventions that increase socioeconomic resources typically occur through the social welfare system, and participating in this system typically affects social status in the United States.
Social welfare programs in the United States are targeted to specific populations, typically low-income working families. Targeting has numerous policy benefits, such as intervening in inequality and efficiently allocating resources, yet it also entails identifying and marking people as poor, a stigmatizing category in the United States. Furthermore, in implementing policies designed to mitigate against fraud or unintended consequences of program receipt, state workers ask intrusive questions, such that accessing many benefits becomes a humiliating and degrading process (Bridges 2010, 2011a, 2011b, 2017; Hughes 2019; Piven and Cloward 2012). To be clear, the status insults vary across programs and are more direct in some programs than others. For instance, receiving some benefits from Temporary Aid to Needy Families requires proving what birth control a recipient uses (California Department of Social Services 2020). EITC recipients, in contrast, report far less stigma, in part due to the program’s reduced surveillance and its administration through the Internal Revenue Service (Pulvera et al. 2023; Sykes et al. 2015). The coupling of a status insult with the receipt of resources means most empirical studies cannot adjudicate between the two sets of mechanisms.
Where does that leave us? Drawing on the health theories outlined above with a focus on interventions, we contend that to evaluate any intervention theoretically we need to consider four components: (1) the type of resource, (2) the size of the resource, (3) whether providing the resource affects other causes of population health, and (4) the timing of the resource relative to the health process and outcome. These components should be tailored for particular populations and contexts.
This requires an enormous empirical lift. We argue, though, that this lift is precisely what the field needs to both be of use for policymakers designing interventions and to launch the next theoretical leap. The case we examine here has unusual analytic capacity to bring insight to the question of what money can buy because it is an exogenous income source that is delivered by the state without a status insult. We review our current case briefly to highlight the utility of considering these mechanisms in tandem.
The Alaska Permanent Fund Dividend is a large universal cash transfer; it is a flexible resource that recipients can use any way they desire. The dividend does not entail a status insult because the cash transfer is universal and does not come with scrutiny or surveillance and therefore does not affect other causes of health. The transfer is received after conception during pregnancy. Where this timing fits into the health processes that result in poor birth outcomes is unknown.
Based on this assessment, we can identify critical elements of our intervention and pinpoint areas of ignorance that impede our ability to make clear predictions about the effects of the intervention. Specifically, we do not know whether the size of the cash transfer, although substantial, is sufficient to affect birth outcomes, nor do we know if birth outcomes can be changed via a cash intervention during pregnancy.
If the cash influx improves the birth cohort’s health, we would then learn three things: (1) newborn health can be affected by increased purchasing power, although the precise mechanism would still be unclear; (2) the amount is sufficient; and (3) health processes leading to poor birth outcomes are reversible during pregnancy.
If the cash influx worsens newborn health, we would know the treatment did have an effect but, again, not by what mechanism. It could have increased or introduced new health risks or enabled higher-risk fetuses to survive to birth.
If the cash influx results in no change to newborn health, then we would similarly be at a place of ignorance. Perhaps birth outcomes are better improved via status mechanisms; perhaps the size of the resource was not enough; perhaps the timing was wrong and came when the health process was irreversible. Our analysis cannot disentangle these possibilities; this would be the purview of future work.
Our study does not close the book on the importance of purchasing power, but because the policy we study uniquely does not combine a status insult with the provision of material resources, it can provide insight most other prior research cannot into what health money can buy.
Given that theory does not guide us to consistent or strong predictions about the effect of a universal cash transfer on birth outcomes, we do not posit a hypothesis. Instead, we view our analysis as providing insight into some of the critical questions that various theoretical perspectives raise for interventions that increase socioeconomic resources.
Empirical Work on the Effect of Income on Newborn Health
To ascertain the causal relationship between income and newborn health, we must examine the provision of cash independent of the recipient’s behavior. Despite other beneficial features, social safety net programs do not enable this examination. First, the provision of cash is typically accompanied by a loss of dignity associated with the severe administration of means-tested benefits in the United States. This threatens causal inference by entangling increased income with a decrease in other flexible resources (e.g., power and prestige), and because the low participation rates among eligible populations creates a strong link between individual behavior and treatment (Herd and Moynihan 2019). Put another way, it is not random who receives the income, even among eligible populations. Second, these programs come with participation requirements, such as employment, or incentives to promote marriage (Moffitt et al. 2009). These requirements can affect who participates (Ku, Brantley, and Pillai 2019) and make it analytically difficult to parse out effects of receiving the benefit from effects of the program requirements or incentives. Furthermore, data on newborn health do not include information on program participation. Scholars often proxy for participation using eligibility criteria. However, because program participation hovers around 75 percent of the eligible population, the error in identifying participants is large.
Additionally, previous studies of interventions have focused exclusively on the pregnancy period, overlooking potential effects of a treatment on selection into pregnancy and childbirth. By overlooking the pre-conception period and the process of selecting into giving birth, most prior work does not capture processes that can indirectly affect a cohort’s well-being at birth and whose effects can be greater than any prenatal behavior (Nobles and Hamoudi 2019). This can lead to biased and inaccurate causal effect estimates.
Our use of the Alaska Permanent Fund Dividend overcomes these empirical limitations. The program’s universality means the additional resources are provided without diminishing prestige or power. Universality also enables us to identify participants within standard data on newborn health.
Evidence from Income Transfers
Causal analyses of income transfers to socioeconomically disadvantaged populations show that increased income has mixed results and primarily small effects on newborn health (Bruckner, Rehkopf, and Catalano 2013; Chung, Ha, and Kim 2016; Currie and Cole 1993; Hamad and Rehkopf 2015; Hoynes, Miller, and Simon 2015; Kehrer and Wolin 1979; Markowitz et al. 2017). 1 For instance, state EITCs increase birth weight of children born to disadvantaged mothers by less than the weight of this article printed (birth weights increased approximately 15 grams, or three printed pages) (Markowitz et al. 2017; Strully, Rehkopf, and Xuan 2010). The EITC increases income by increasing labor market participation and through a tax benefit. Scholars cannot distinguish between the two effects. Using variation in the timing of when the Food Stamps Program, a near-cash transfer, was implemented by neighboring states, Almond, Hoynes, and Schanzenbach (2011) find increased birth weight with the program, with the largest improvements for the lowest birth weights. They cannot identify who received Food Stamps and so inflate their estimates to approximate the treatment of the Food Stamps program on the treated. They find an improvement of 15 to 20 grams for White children and 13 to 42 grams for Black children. The start of the PFD improved birth weight by 20 grams during the time Alaskans were anticipating but did not receive the money, and by 35 grams when they first received it (Chung et al. 2016).
Current cash transfer experiments are modeled on the Negative Income Tax experiments of the late 1960s and early 1970s in a handful of cities in the United States and Canada. The additional income given to women in Gary, Indiana, increased birth weight for babies of women at high risk of having poor-health infants. This experiment, however, suffered from a small sample size that was not diverse with regard to most demographic characteristics (Kehrer and Wolin 1979). The experiment showed no effect of the cash on newborn health in Manitoba (Forget 2011).
Although the effects on average birthweight are modest, cash transfers have a larger effect on the incidence of low birth weight (under 2,500 grams). Exploiting the 1993 expansion of the federal EITC, Hoynes and colleagues (2015) find that, for every thousand dollars, the effect of the treatment on the treated is a 2 to 3 percent decline in low birth weight. State EITCs reduce the probability of low birth weight by 4 to 11 percent among low-educated mothers (Markowitz et al. 2017). Food Stamps reduce the likelihood of low birth weight for White babies by 1 percent, and by 7 to 8 percent when inflated to estimate the treatment on the treated; the effect on Black babies was similarly sized but not statistically significant (Almond et al. 2011).
The start of the PFD decreased the likelihood of a low birthweight baby by 0.5 percentage points in the anticipatory period and 0.7 percentage points in the realized period (Chung et al. 2016). This analysis, however, chose control states for a synthetic control for Alaska based solely on trends in birth outcomes. State-level factors that could affect birth outcomes, including economic conditions and policies, were not incorporated. This is of particular concern in this case given that Alaska abolished income tax in 1980, just two years before the first disbursement of dividends (Groh and Erickson 2012). This tumultuous policy period before the PFD suggests synthetic control methods—or any controls that focus on the start of the program—are not well-suited for this case. Furthermore, we argue, along with others (e.g., Nobles and Hamoudi 2019), that models must account for selection effects, which one cannot do with a focus on the program’s start.
Income transfers can also affect other birth outcomes. The 1993 EITC expansion improved Apgar scores, on average, and decreased the likelihood of low Apgar scores. It also decreased the likelihood of a preterm birth (Hoynes et al. 2015), as did state EITC programs (Karasek et al. 2023; Markowitz et al. 2017). The Food Stamp Program had no detectable effect on preterm births (Almond et al. 2011). Other work, however, finds no or negative effects of cash transfers on infant health (Bruckner et al. 2013; Hamad and Rehkopf 2015). Using policy changes in the EITC benefit levels as an instrument for post-tax income, Hamad and Rehkopf (2015) find no causal relationship between income and birth weight, low birth weight, or preterm birth.
Heterogeneous Effects
Unsurprisingly, the effects of cash transfers on newborn health differ by birthing parent characteristics. Children born to Black mothers have greater sensitivity than do children born to White or Latina mothers (Hoynes et al. 2015). Black women in California who were likely EITC eligible had increased odds of a very low birthweight baby after women were expected to receive the credit (Bruckner et al. 2013). The effect of cash transfers differs by parental age, with the youngest and oldest birthing parents being less sensitive to the transfer than parents in the middle of the age range (Strully et al. 2010). The effect of the cash transfer does not differ by marital status among low-income birthing parents (Markowitz et al. 2017). First-births are less sensitive to the additional cash (Hoynes et al. 2015; Markowitz et al. 2017). These studies, however, examine cash transfers to disadvantaged populations with limited axes of variation.
Empirical Case: Alaska Permanent Fund Dividend
We examine the payments the Alaskan state government made to every Alaskan resident since 1982 through the Alaska Permanent Fund Dividend. Every October, this cash transfer is given to a large and diverse population, including children (via their guardians), irrespective of their characteristics or behavior (Kueng 2018). Following prior work, we argue that the amount of money given every year increases and decreases in a way that mimics random assignment in an experiment (see Hsieh 2003; Kueng 2018; Watson, Guettabi, and Reimer 2020). That is, for over three decades, a repeated quasi-natural experiment has occurred involving the hundreds of thousands of people living in Alaska.
The amount of the transfer varies markedly. It ranges from a low of $331 (1984; $626 in 2010 dollars) to a high of $3,269 (2008, including a $1,200 bonus; $3,366 in 2010 dollars) per resident with a mean of $1,547 (SD = $586) (see Figure 1). To put this in context, the value of the cash transfer for a family of four ranges from the equivalent of 70 percent of the value of Food Stamps to three times the value of Food Stamps. For each household, it typically exceeds the value of the federal EITC (Crandall-Hollick 2018). The variation in the payment amount is due to the nature of the dividend calculation: during our study period, state law dictated a formula for the dividend fund as a share of net earnings on investments held by the Alaska Permanent Fund Corporation over the past five fiscal years (Erickson and Groh 2012). This variation, which we argue is random with respect to individual Alaskans, is analytically useful, as it allows us to measure the effects of different treatment dosages. This year-to-year variation is the first source of variation we exploit in our analyses. The second source is variation in the amount received across households in a given year.
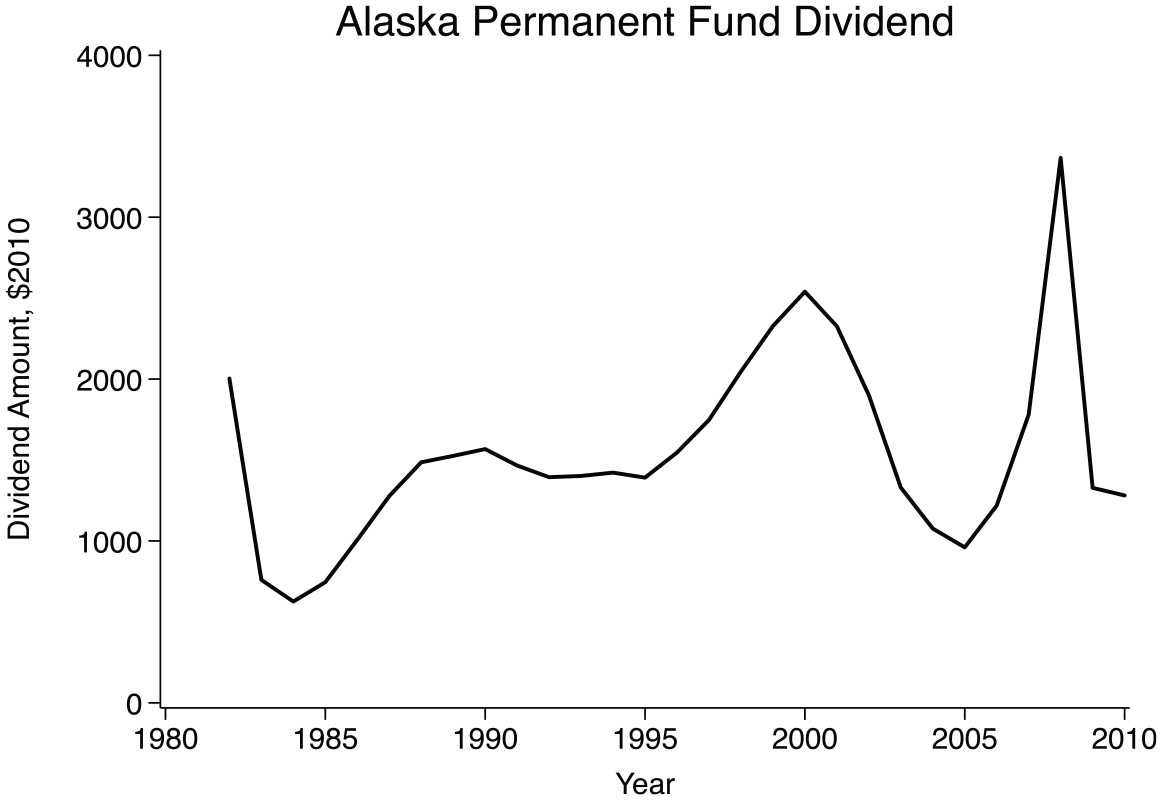
Alaska Permanent Fund Dividend Per-Person Dividend Payments in $2010, 1982 to 2010
Unlike other cash transfers in the United States—or near-cash transfers such as Food Stamps—the dividend is given to every resident. Any individual who has been resident in Alaska for the prior 12 months or was born in Alaska in the prior 12 months is eligible, with rare exceptions. Minors’ dividends are paid to one parent or legal guardian (Erickson and Groh 2012). There are no low-income requirements, as with welfare (Currie and Cole 1993; Moffitt 1998), Food Stamps (Almond et al. 2011), or the EITC (Baughman and Dickert-Conlin 2009; Hoynes et al. 2015; Strully et al. 2010). The dividend is not only available to working people like the EITC, or only to pregnant people like WIC. It does not phase out, even at high income levels like the tax provision of personal exemption (Whittington 1992; Whittington, Alm, and Peters 1990). Given this, and Alaska’s demographic similarity to the nation as a whole (detailed below), our case provides the best available window into the effects of an unconditional cash transfer in the United States.
Despite these beneficial analytic features, the PFD program differs in some important ways from proposed cash transfer policies that are gaining popularity. First, the size of the transfer varies year to year. While this is convenient for analysis purposes, most policy proposals suggest consistent payments that do not vary, except for cost-of-living increases. Second, although the transfer is often large compared to other benefits such as SNAP or the EITC, it falls far short of the benefits transfer proponents advocate. Third, the dividend is paid as an annual lump sum, whereas many proposals have monthly payments. Fourth, the transfer is “flat,” or untargeted, providing the same amount of money to every resident. While this aligns with the legislative intent of the PFD, many would argue it is an inefficient allocation of resources for a policy aimed at reducing inequality.
Although the PFD has few program requirements, it may shape behaviors related to income generation or benefit application in ways that affect total individual household income. For instance, some evidence suggests some recipients slightly reduce work hours after higher dividend payments (Bibler, Guettabi, and Reimer 2023). We cannot directly empirically examine these behavioral effects in this study, but it is the sum total of people’s various responses we are interested in as it relates to birth outcomes. For instance, if pregnant people respond to larger dividend payments by reducing work hours, which reduces stress and improves the fetus’s health, our analysis will be able to detect this.
An extensive application for first-time applicants requires proof of residency, among other verifications. Subsequent annual applications are trivial. Applications are due in March. Participation rates are high, above 92 percent in many years and often above 97 percent (Alaska Permanent Fund Dividend Division 2000). News reports estimate the dividend amount in the spring with marked accuracy (Kueng 2018). The official amount is announced in September, and the payment is made as a lump sum in October. In the early years of the dividend, the payment was made via check; in 1993, direct deposit became available.
Medicaid has covered abortion in Alaska since the 1970s. A relatively large proportion of abortions are paid for by Medicaid (42 percent in 1990; 46 percent in 2010) (for a summary, see New 2015). Thus, despite abortion being a theoretical mechanism in our proposed model for how income could affect the composition of birthing parents, prior analyses show that dividend payments do not affect abortion rates in the state at a population level (Cowan and Douds 2022).
The Case for Exogeneity
Our causal claims rest on three features of the case. First, the amount of the dividend is not predictable by individual Alaskan residents’ behavior (i.e., it is exogenous). Second, the amount varies year to year and across households. Third, some people who give birth in a given year are pregnant when the dividend is disbursed in October and some are not.
The fund was established in 1976 via an amendment to the state’s constitution (Groh and Erickson 2012). Court battles delayed implementation of the dividend disbursement until 1982. The initial endowment was from mineral royalties and leases of Alaskan public lands, primarily for oil extraction. The Alaska Permanent Fund Corporation—a quasi-independent state agency—invested the endowment in broadly diversified financial and real assets. The revenue for the transfer is a fixed percentage of returns from the investment fund over the previous five fiscal years.
Not all the fund’s returns are distributed; most of the returns are re-invested. The principal continues to be fortified by mineral royalties and leases, but proceeds from minerals have substantially declined as a portion of the fund’s total market value. The fund’s annual revenue from mineral royalties and leases represents less than 0.6 percent of the total market value today (Kueng 2018). State mineral revenue represents only 2 percent of annual fund additions. Since 1985, investment returns have been the primary growth mechanism. Mineral royalties from a given year are deposited directly into the principal of the fund and are not counted as earnings in the dividend fund calculation; mineral revenues can only influence payments in subsequent years after realizing gains from investment. This assuages concerns that the dividend amount is reflective of local Alaskan economic conditions. Furthermore, oil price shocks that might affect the non-PFD portion of Alaskans’ income and the local economy generally would not affect the dividend amount.
Our analytic strategy relies on annual variation in the size of the dividend. If Alaskans smoothed their consumption, then this would threaten our casual inference. Prior work shows Alaskans do not smooth their consumption in response to the PFD for either durables or nondurables (Amorim 2022; Kueng 2018) (but see also Hsieh 2003). Although this contrasts with traditional economic theory, it is consistent with reviews of the question in economics (Jappelli and Pistaferri 2010). We conduct a series of sensitivity analyses that show birth outcomes are more sensitive to the absolute magnitude of the dividend than to changes in it.
The Exclusion Restriction
If a factor that affects newborn health is correlated with the dividend amount, then we might misidentify the dividend as the source of that effect. Two factors that could potentially meet this criterion are Alaskan economic conditions and public health investments. As discussed earlier, revenue for the dividend is not directly derived from state mineral extraction revenue, so the local economy is not related to the dividend amount in a way that would threaten our causal estimates. Nonetheless, our analyses include the annual Alaskan unemployment rate, per capita income, and the price of oil to account for local economic conditions, and our findings are robust (see Appendix Table A1).
If in years when the dividend was high Alaska also made public health investments with a focus on maternal and child health, then we would be unable to parse the effects of the cash transfer from the investment. We examined historic public health expenditure reports and public health histories and interviewed five public health officials. The public health system changed over the study period by expanding access to maternal and newborn healthcare for rural Alaskans (Borland et al. 2015; Nord 1995). To attend to this, we conduct a sensitivity analysis of only Anchorage residents, as there was no meaningful new investment in Anchorage. The results for Anchorage are substantively similar to the state as a whole (see Appendix Figure A2), which allays concerns that public health funding, rather than the PFD income supplement, is driving our results.
Generalizability
Parts of Alaska are similar to other parts of the United States, but Alaska has some notable differences to the country as a whole. Table 1 compares the Alaskan and U.S. populations over our study period on key demographic factors. Anchorage, where over half of Alaskans live, is similar in many respects to other medium-sized cities. In both Alaska and the United States, 64 percent of the population is non-Latinx White. In Alaska, however, the racially minoritized population is composed of markedly more Alaska Native people and fewer Black Americans and Latinx Americans than the country as a whole. Alaska also has a larger proportion of rural residents. Parts of rural Alaska are markedly more remote than rural areas in the other 49 states. Alaska’s fertility rate is also higher than the nation’s. This is largely driven by the childbearing of Indigenous Alaskans, who disproportionately reside outside of Anchorage. Our sensitivity analysis of Anchorage alone attends to this and concerns about rurality for generalizability.
Comparison of U.S. and Alaska Demographics: 1980 to 2010
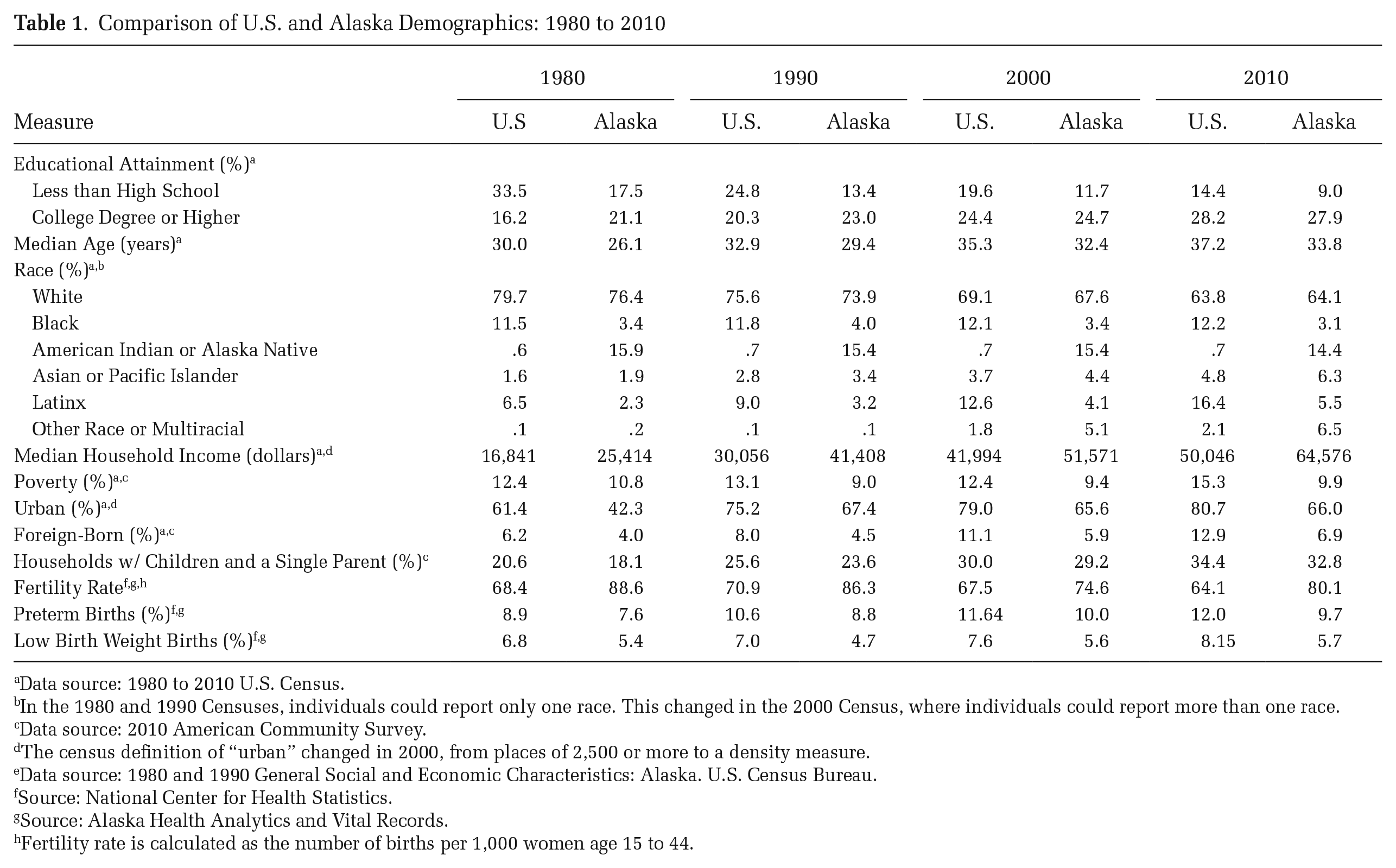
Data source: 1980 to 2010 U.S. Census.
In the 1980 and 1990 Censuses, individuals could report only one race. This changed in the 2000 Census, where individuals could report more than one race.
Data source: 2010 American Community Survey.
The census definition of “urban” changed in 2000, from places of 2,500 or more to a density measure.
Data source: 1980 and 1990 General Social and Economic Characteristics: Alaska. U.S. Census Bureau.
Source: National Center for Health Statistics.
Source: Alaska Health Analytics and Vital Records.
Fertility rate is calculated as the number of births per 1,000 women age 15 to 44.
Methods
Integrating Selection into Giving Birth into Analyses of Newborn Health
Income can affect a birth cohort’s health through two pathways: a fertility effect and a prenatal response effect. Our analysis aims to estimate the prenatal response effect of cash given after conception and during pregnancy. However, previous work shows that larger dividend payments in Alaska are followed by increases in births to socioeconomically disadvantaged groups (Cowan and Douds 2022). Given that parental socioeconomic disadvantage is positively correlated with worse newborn health, this selection effect alone could result in a birth cohort with diminished health, causing us to incorrectly estimate the effect of cash transfers received during pregnancy. 2 To properly estimate the effect of a universal cash transfer on newborn health, we must first account for the indirect effect of cash transfers on newborn health through a fertility selection effect, as ignoring these effects when examining birth outcomes could introduce marked bias (Nobles and Hamoudi 2019).
We account for the indirect effect of the PFD on newborn health through its effect on the demographic composition of birthing parents (for a depiction of this process, see Appendix Figure A1). The additional income provided by the PFD changes the composition of birthing parents up to two years after disbursement, increasing births among socioeconomically disadvantaged groups (Cowan and Douds 2022). To account for this effect in our outcome analyses, we create weights that account for the heterogeneous effects of the cash transfer on fertility.
We create weights by estimating Cowan and Douds’s (2022) model predicting the Alaskan birth rate with the addition of interactions between each of the birthing-parent demographic characteristics (age, marital status, educational attainment, racial identity, and parity) and the two dividend amounts (DIVj(t – 1) and DIVj(t – 2)) measuring payments one and two years prior to birth (a total of 10 two-way interactions). The full model specification is in the Appendix. This model estimates all heterogeneous effects across demographic groups at once to produce one weight. To create the weights, we predict birth rates from the model by year and demographic grouping (DG)—groups determined by constellations of age, marital status, educational attainment, racial identity, and parity—with the t – 1 and t – 2 cash transfer amounts set to the minimum dividend payment amount ($625.80). These predictions represent the probability a person would give birth in year t if the dividend payments at t – 2 and t – 1 had been at their minimum levels. Because our data include only years in which payments were made, we use the minimum dividend amount rather than 0 to avoid extrapolating outside of our observed data to create these rates. We use these predicted rates as weights in the birth outcome models to attend to composition effects that can indirectly affect birth outcomes. This is akin to an inverse probability of treatment approach.
Prenatal Response
We assess the effect of receiving the dividend payment during pregnancy on birth outcomes for all singleton births to people age 15 to 44. Here, we take advantage of the fact that some people who give birth in year t were not pregnant in October when the payment was disbursed. We control for birth outcome trends in all models by including annual measures of each outcome for the United States as a whole, derived from the natality data (e.g., U.S. average birth weight).
Our birth outcome analyses consist of unadjusted and adjusted regressions predicting the following outcomes: birth weight in grams, low birth weight (<2,500 grams), very low birth weight (<1,500 grams), preterm birth (<37 weeks), and five-minute Apgar score. We also have two pregnancy outcomes: the month prenatal care began and number of prenatal visits. We estimate logistic regressions for dichotomous outcomes, and we estimate ordinary least squares regressions for continuous outcomes. In unadjusted models, our selection weight is not applied and the outcomes are predicted by the household dividend payment in year t, the year, and the average birth outcome for the United States. In fully adjusted models, selection weights are applied, and the outcomes are predicted by the household dividend payment in year t, birthing parent characteristics, the year, the Alaska unemployment rate, and the average birth outcome for the United States. All models predicting birth weight, low birth weight, and preterm birth also control for the infant’s sex assigned at birth. We estimate continuous outcomes using the following adjusted model:

where j indicates DG and t indicates year. Yjt is the outcome for DG j in year t; β0 is the intercept; DIVj(t) is the cash transfer to each household in that year, set to 0 if no dividend was received during pregnancy; vector
We estimate dichotomous outcomes using the following adjusted model:

where (pjt) is the probability of the dichotomous outcome for DG j in year t, and other model elements are the same as in the OLS model.
We weight the adjusted models using the probability weights obtained from the rate model that indicate the parent’s likelihood of giving birth if there had been two prior minimum-value transfer payments. This approach allows us to estimate the effect of the transfer in year t on birth outcomes net of the demographic compositional effects induced by the heterogeneous treatment effects of the dividend at t – 1 and t – 2 on who gives birth at t. That is, the weights allow us to examine the effect of a transfer during pregnancy as if no prior increase in the transfers had occurred. For pregnancies during which no dividend payment was received, the dividend amount is set to 0. Given findings on consumption smoothing, we believe this to be the best strategy for these pregnancies. However, our results are robust to alternative treatments, including assigning them the dividend value at t, which assumes saving, and dropping them.
This analytic strategy takes advantage of three sources of variation: yearly variation in the size of the dividend, variation across household sizes in amount received in a given year, and variation in who receives the dividend while pregnant. This strategy thus relies on internal controls and does not include an external comparison group or pretreatment control. We contend that this strategy is appropriate given the treatment has continuously occurred in varying “dosages” for almost three decades. A pretreatment control period prior to the first disbursement in 1982 cannot serve as a suitable control for, say, 1995, 13 years into the treatment. External controls, too, such as demographically similar states, may not be suitable for a continuously treated population. A popular approach to this type of case, synthetic control, is a poor choice in our empirical case. Even were we to restrict our analysis to the early years of disbursement, the establishment of the PFD was part of a series of structural changes to Alaskan life that came with the oil boom, including abolishment of the state income tax in 1980.
We present these results for the birth cohort as a whole. We also separately examine birth outcomes to birthing parents with low (high school or less) and high (bachelor’s degree or more) educational attainment, as well as to birthing parents who are Alaska Native and White. Comparing effects across these groups allows us to assess how a cash transfer during pregnancy may differentially affect birth outcomes across groups with different levels of resources. Finally, we examine the possibility of selection on non-demographic characteristics that could not be captured in our weight creation procedure. That is, we assess whether smoking and drinking during pregnancy affects the birth outcomes we estimate by adding them as covariates in the birth outcome models. We then consider whether smoking and drinking were adopted or increased during pregnancy, or if they ceased or persisted through pregnancy. These results will determine whether to think of these as prenatal behaviors or more as parental characteristics on which selection into childbearing may occur.
Sensitivity Analyses
Because scholarship on the PFD is recent and rapidly increasing, there is not yet consensus on how to model the PFD, nor the selection processes, so we test our conclusions using a wide array of sensitivity tests: (1) We performed our analyses for Anchorage alone to assuage concerns about the exclusion restriction and generalizability. (2) We estimate our models using the per-person dividend amount rather than the household dividend amount. This removes one source of variation: the difference in the dividend paid to households depending on household size. (3) We estimate our models with year fixed effects added to ensure our estimates are not driven by comparing temporally distant years. (4) We examine whether normalization to the dividend occurs by assessing whether jumps or dips in the dividend, which can be thought of as unanticipated, better predict birth outcomes than does the magnitude of the payment. (5) We test other macro-economic indicators besides the unemployment rate: namely, the price of crude oil and Alaskan per capita income. (6) We altered our missing data procedures, as described below.
Data
Natality Data
All analyses use restricted natality data provided by the National Vital Statistics System, which include all births in the United States from 1982 to 2010. These data contain the complete population of U.S. births and include a wealth of information on birthing parents, including their demographic characteristics and prenatal behavior like smoking, drinking alcohol, and prenatal visits. For most of our analyses, we use only births to people residing in Alaska. Birthing parent characteristics included in our analyses are age, racial identity, marital status, education, and parity. Following convention, we group individuals into five-year age groups and restrict the analysis to people age 15 to 44. Given the racial composition of Alaska, we group birthing-parent racial identity into White, Alaska Native, and other. Marital status is dichotomized as married and unmarried. We group educational attainment into less than high school, high school, some college, and bachelor’s or greater. Parity is coded as first birth, second birth, third birth, and fourth or above birth. Smoking during pregnancy is a dichotomous measure (1 = smoked at least one cigarette a day, on average, while pregnant; 0 = did not smoke while pregnant), as is drinking during pregnancy (1 = drank alcohol while pregnant; 0 = did not drink while pregnant). We also examined whether the birthing parent was born in Alaska; this does not predict birth outcomes and is excluded from our analyses shown here.
For birth outcomes, we examine birth weight in grams, low birth weight (<2,500 grams), very low birth weight (<1,500 grams), preterm birth (<37 weeks), and five-minute Apgar score (0 to 10). For pregnancy outcomes, we examine month prenatal care began (1 to 11) and number of prenatal visits (0 to 49).
In all analyses, we use the dividend amount given to each household. We identify household size through the marital status and parity variables in the natality data. An alternative specification would be to include only the annual per-person dividend. We argue that total household payment is a better measure for a number of reasons. First, it represents the total amount of money each family receives. To model, for instance, a family of four as receiving the same amount of money as a family of one would dramatically misrepresent the cash transfer. Second, we can account for the fact that with each additional family member comes additional expenses by including parity and marital status in our analyses. This adjusts for family size but acknowledges that a spouse’s net expenses are quite distinct from a child’s. Our main analyses all use the total household dividend amount, but we also present sensitivity analyses using the per-person dividend amount. All dividend measures are converted to 2010 dollars.
We align all data sources to years based on PFD payment distribution. Because payment occurs in October of each year, PFD-aligned years begin in October and end in the following September. As an example, a birth occurring in April 1996 was coded as PFD year 1995 because it falls in the 12 months following the distribution of the 1995 dividend payment. All references to years below refer to PFD-aligned years.
All analyses also account for macro-level Alaskan economic trends through inclusion of the Alaskan unemployment rate as a control. Sensitivity analyses also include per capita income and the crude price of oil. These measures are aligned to PFD distribution. To do this, we assign one-fourth of the value of the measure in year t to PFD year t, and three-fourths of the value of the measure in year t + 1 to PFD year t.
Missing data
In total, 4 percent of births had missing values on one or more covariates; this ranged from 0.93 percent of births in 1996 to 15.3 percent of births in 2003. To address missing data, we used a threshold deletion strategy. Specifically, we chose a threshold of 7.5 percent and excluded from our analysis any year in which more than 7.5 percent of births had missing values on one or more covariates. Based on this threshold, we excluded 2001, 2003, and 2008 from our analyses. For all other years, we dropped all cases with missing values on covariates and then randomly dropped more observations until the percentage dropped reached 7.5 percent. That is, for all included years, exactly 7.5 percent of cases were dropped. We use this approach to ensure the total number of births per year is not affected by different rates of missing data across years. This approach matches the missing data strategy used for the birth rate model from which we generate our weights to account for selection into giving birth (Cowan and Douds 2022). The threshold-deletion strategy ensures that birth counts for each year are artificially reduced by the same proportional amount. As a sensitivity analysis, we also tested alternative thresholds (6 and 9 percent) and our results were not substantively altered.
We used individual-level data produced from the threshold deletion procedure in the outcome analyses. For observations with missing values on the outcomes, which ranged from 0.02 percent for birth weight to 3.4 percent for number of prenatal visits, we used listwise deletion because our birth outcome analyses do not have the same sensitivity to changes in counts as does the birth-rate model used to produce the weights.
Population Counts
To assess birth rates, we require denominators that are population counts. The denominators for the birth rates are population estimates for women age 15 to 44 by DG, which we obtained in two steps. First, we linearly interpolated proportions of the population by DG from 1980, 1990, and 2000 Census five-percent samples and the 2008–2012 American Community Survey sample. Second, we multiplied these proportions by intercensal population counts for women age 15 to 44 by five-year age groups provided by the Alaska Department of Labor and Workforce Development. These population counts incorporate information from the applications to the annual Permanent Fund Dividend. Given these unique, annual data from Alaska, the denominators are more accurate than those typically used in rate analyses that rely only on intercensal interpolation.
Pregnancy Risk Assessment Monitoring System
To assess the relationship between the dividend and whether birthing parents sustain, begin, or stop consuming tobacco and alcohol, we examine data from the 1990–2010 Pregnancy Risk Assessment Monitoring System (PRAMS) surveys. PRAMS surveys are conducted annually by the Centers for Disease Control in collaboration with individual state health departments. In each participating state, a stratified sample of postpartum birthing parents is drawn from the state’s birth certificate file, and questionnaires are filled out on paper; telephone follow-up is used to reduce non-response.
Alaska’s PRAMS samples approximately one in every six birthing parents of newborns each year. They oversample Alaska Native birthing parents, and weighting adjusts estimates to reflect the total population of Alaskans who gave birth in a given year.
The measures used regarding smoking are whether and how much the parent smoked in the three months before getting pregnant and whether and how much they smoked in the third trimester of their pregnancy. With regard to consuming alcohol, we use one measure that captures whether and how many times the respondent drank five or more alcoholic drinks in one sitting in the three months prior to getting pregnant, and another question assessing the same measure during the third trimester. We dichotomize both sets and create four categories for smoking/drinking: never (did not smoke/drink prior to or during pregnancy), always (consumed both before and during), began consuming, and quit consuming.
Results
Table 2 presents descriptive statistics for birth outcomes and birthing parent characteristics. Here we briefly comment on outcomes and characteristics that changed over time. Occurrence of low birthweight, very low birthweight, and preterm birth increased slightly between 1985 and 2010, from 3.97 percent of infants born low birthweight in 1985 to 4.19 percent in 2010. Aligning with national trends, birthing parents tended to be older at the end of the time period. Whereas 31.57 percent of birthing parents were age 20 to 24 in 1985, 28.54 percent were in 2010, and birthing parents age 40 to 44 increased from 0.75 percent in 1985 to 2.20 percent in 2010. The share of births to married birthing parents declined from 81.83 to 62.40 percent. In addition, birthing parents became, on average, more educated during the period, with the share having less than a high school education declining (13.03 versus 11.00 percent) and the share with a bachelor’s degree or more increasing (16.90 versus 22.44 percent). Finally, birthing parents were less likely to be White and more likely to be Alaska Native or other race across the period. Our models include controls for birthing parent characteristics, and in supplementary models we add year fixed effects to ensure our results are not driven by comparisons of temporally distant years.
Descriptive Statistics of Birth Outcomes and Birthing Parent Characteristics, 1985 to 2010
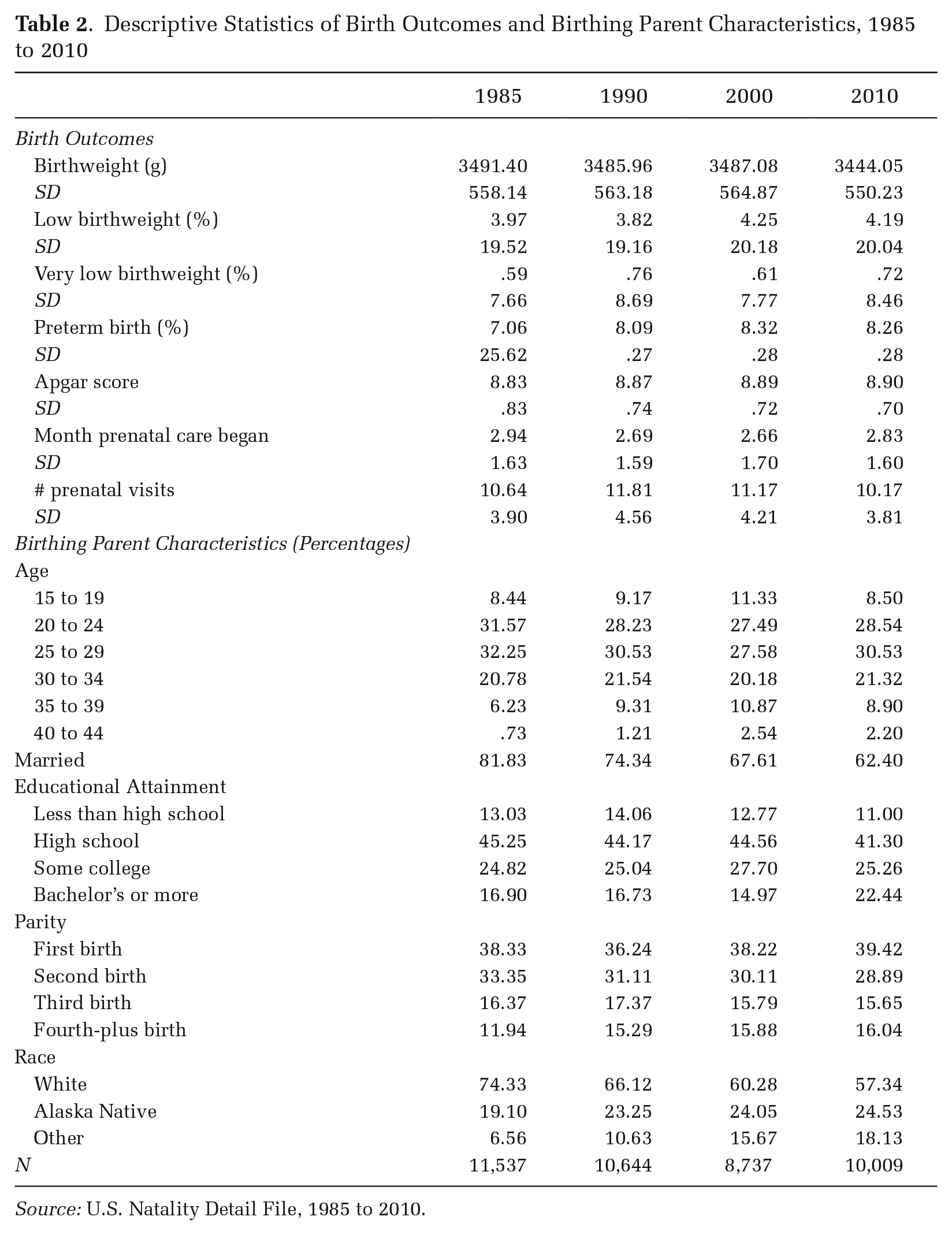
Source: U.S. Natality Detail File, 1985 to 2010.
Birth Outcomes
As we argue above, newborn health is indirectly a function of who gives birth and directly a function of prenatal response during pregnancy. Figure 2 shows how the size of the dividend affects birth outcomes. For each outcome, coefficients with 95 percent confidence intervals for the dividend in year t are reported for the unadjusted and adjusted models for five groups: the full population, birthing parents with low educational attainment (a high school degree or less), birthing parents with high educational attainment (a bachelor’s degree or higher), White birthing parents, and Alaska Native birthing parents. We report findings for the latter two groups because they are the two largest racialized groups in the population. Model estimates for other racialized groups are consistent with the presented findings but have high levels of uncertainty due to small group size. Dividend payments are measured in $1,000 units.
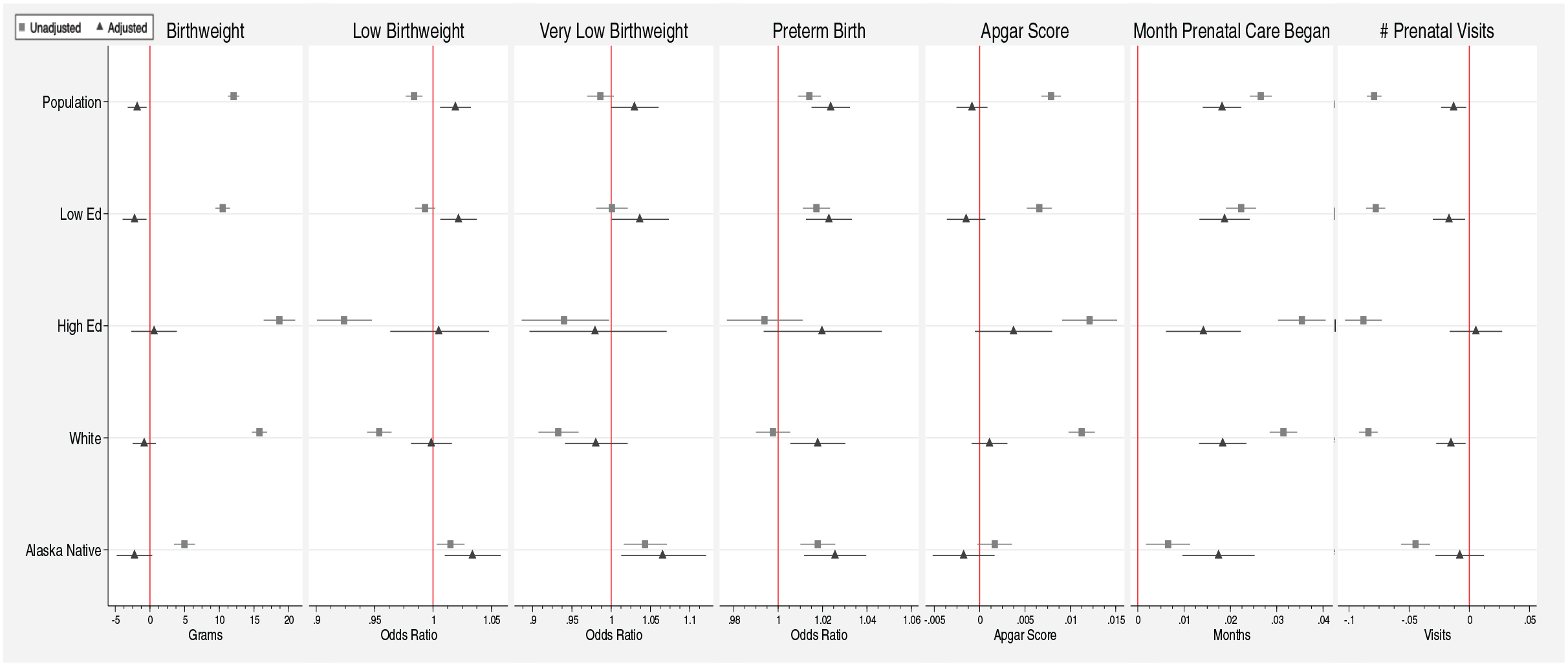
Birth Outcome Model Results
Across most birth outcomes, unadjusted models at the population level suggest that larger cash transfers during pregnancy are associated with improved outcomes. For instance, the unadjusted models predict an increase in birthweight of 12.06 grams and lower odds (OR = 0.98) of low birthweight per $1,000 received during pregnancy. However, the adjusted models, which are weighted to account for selection into giving birth and birthing-parent demographic characteristics, indicate that receiving a cash transfer during pregnancy has negative but very small effects on birth outcomes. If a pregnant person receives an additional cash payment of 1,000 dollars per household, the effect on birth weight is a decrease of 1.84 grams. An additional 1,000 dollars per household causes a small increase in the likelihood of low birth weight (OR = 1.019) and preterm birth (OR = 1.023). A cash transfer has no effect on incidence of very low birthweight or five-minute Apgar scores. Together, these results suggest that income transfers during pregnancy do not meaningfully improve birth outcomes at the population level.
Larger dividend payments result in a very small delay in the start of prenatal care (0.018 months or 13 hours) and the number of prenatal visits (–0.013 visits). The effects are similar if measured as the likelihood a person obtained prenatal care in the first trimester. Prenatal care has positive effects on parental well-being, but it has no effect on birth outcomes (Fiscella 1995), so this does not meaningfully explain our results. Models estimated with year fixed effects, with the per-person dividend amount rather than the household amount, and using different macro-economic controls all show results substantively similar to our main results (see Appendix Tables A1, A2, and A3).
The middle section of Figure 2 presents results for models including only birthing parents with low (high school diploma or less) or high (bachelor’s degree or more) educational attainment. Comparing results from these models, we see that the negative effects of cash payments on birth weight, low birth weight, very low birth weight, and preterm birth are driven by births to parents with low education. We find no negative effects for births to highly educated parents. A $1,000 cash transfer causes a minuscule delay in the timing of the start of prenatal care for parents in both educational categories. Despite these differences across educational groups, the negative effects on birth outcomes to parents with low educational attainment are still very small.
The bottom section of Figure 2 presents results for White and Alaska Native birthing parents separately. Among racialized groups, the small negative effects seen at the population level are largely driven by births to Alaska Native birthing parents, not White birthing parents. Dividend payments had no effect on birthweight for births to White or Alaska Native birthing parents, yet slightly increased the odds of low (OR = 1.03) and very low (OR = 1.07) birthweight for Alaska Native birthing parents. Dividend payments increased the likelihood of preterm birth for both groups. We see no effect of the dividend on Apgar scores for either group, but there is a slight delay in the start of prenatal care (0.02 months for both groups). The dividend also causes a miniscule decrease (–0.02 visits) in the number of prenatal visits for White recipients but not for Alaska Native people.
When we re-estimate our models for births in Anchorage alone, shown in Appendix Figure A2, results are substantively similar with a few exceptions. First, adjusted models show the dividend has no statistically significant effect on the month prenatal care began for parents with low educational attainment, and no statistically significant effect on the number of prenatal visits for the population and for parents with low educational attainment. Adjusted models show a small negative effect on average birthweight for Alaska Native parents and no effect on low birthweight. Likewise, effects for month prenatal care began and number of prenatal visits for White parents—both statistically significant for the full state population—are not significant for Anchorage only. Given the very small negative effect sizes at the state level, we consider a null effect substantively similar. The Anchorage results assuage concerns about generalizability and the exclusion restriction, as Anchorage is more demographically similar to the U.S. population and has a more similar fertility rate than does the state as a whole. Furthermore, Anchorage did not receive additional investments in prenatal health during the study period.
The very small effects identified raise the question of whether Alaskan residents, after a period of acclimation, come to expect the dividend and normalization to the treatment occurs. We test this possibility by re-estimating our models with two different types of treatment measures meant to capture “unexpected” portions of the payments. First, we measured each year’s dividend amount as a deviation from prior years’ average payment amounts with three different lags: one, three, and five years. Second, we regressed dividend payments on year for the previous three and five years and then predicted the dividend amount in a given year. We calculated the residual by subtracting the observed payment from the predicted payment and used this residual as the treatment. Re-estimated models using these various treatment measures do not support a normalization explanation (results available upon request). Jumps and dips in the dividend do not significantly predict birth outcomes; instead, the magnitude of the dividend in a given year affects, albeit very slightly, a cohort’s birth outcomes.
Evidence regarding whether positive or negative shocks during specific stages of pregnancy have differential effects is mixed. To account for the possibility of effects varying according to when in a pregnancy additional income was received, we conducted our birth outcome analyses stratified by trimester. Results of these analyses are consistent with the full model results and do not reveal consistent differential effects by trimester but may suggest smaller or null effects when money is received in the third trimester. Results available upon request.
Mechanisms Linking Income and Birth Outcomes
What mechanism explains the (albeit small) effect of cash on birth outcomes? As in much research, our data are insufficient to fully account for mechanisms, but we have some suggestive evidence. When we control for whether a birthing parent smoked or drank during pregnancy, there is no relationship between the dividend payment and birth weight or low birth weight (see Table 3).
Birth Outcomes: Smoking and Drinking Controls
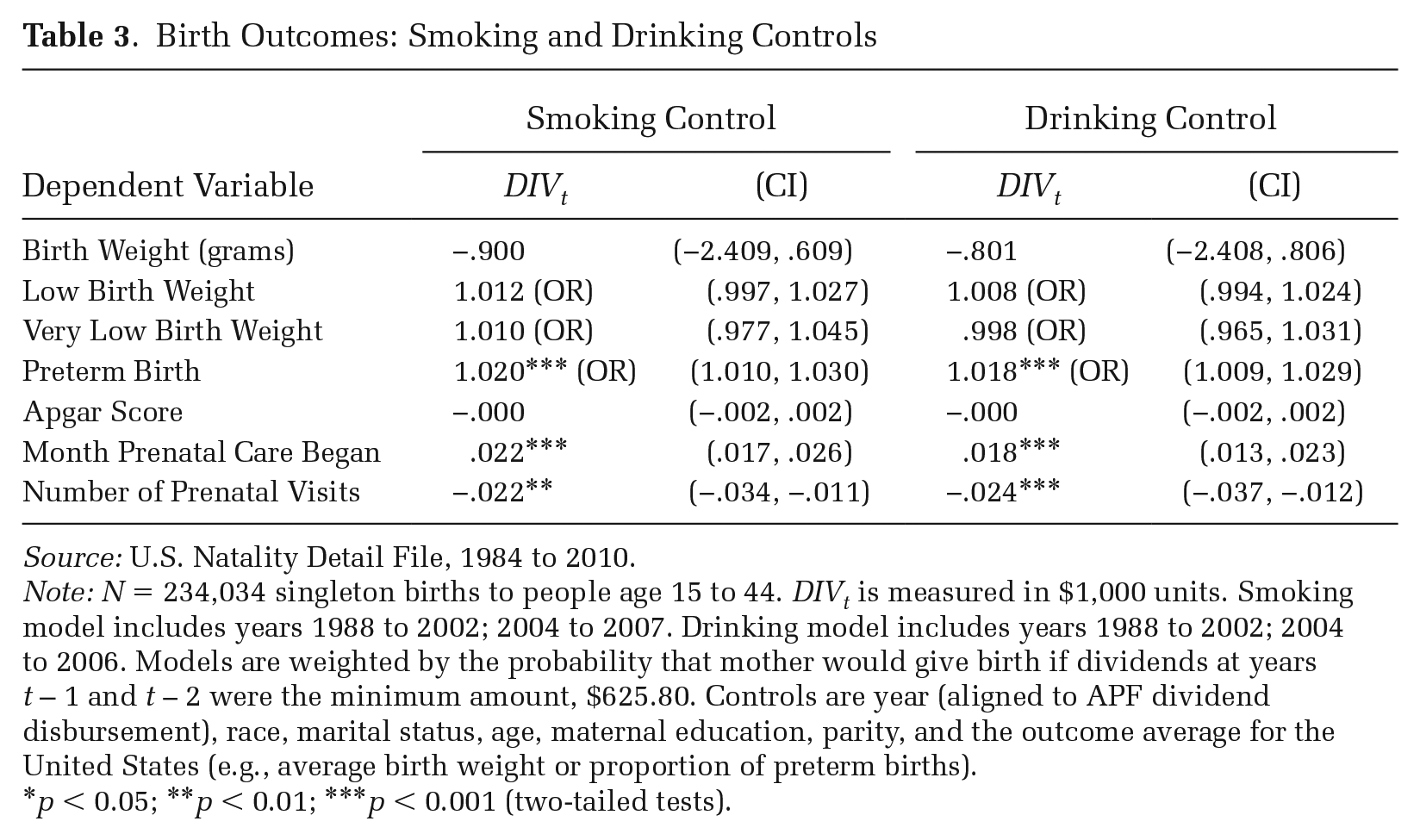
Source: U.S. Natality Detail File, 1984 to 2010.
Note: N = 234,034 singleton births to people age 15 to 44. DIVt is measured in $1,000 units. Smoking model includes years 1988 to 2002; 2004 to 2007. Drinking model includes years 1988 to 2002; 2004 to 2006. Models are weighted by the probability that mother would give birth if dividends at years t – 1 and t – 2 were the minimum amount, $625.80. Controls are year (aligned to APF dividend disbursement), race, marital status, age, maternal education, parity, and the outcome average for the United States (e.g., average birth weight or proportion of preterm births).
p < 0.05; **p < 0.01; ***p < 0.001 (two-tailed tests).
Smoking and drinking controls do not substantively change the small negative effects on preterm birth, suggesting the greater incidence of low birth weight seen in the main model does not occur through a mechanism of preterm delivery. The small effects for the start of prenatal care and the number of prenatal visits are also unchanged with the addition of smoking and drinking controls.
It is possible that the extra income enables pregnant people to engage in these behaviors that negatively affect newborn health. We think it is more likely, though, that the extra income is enabling more people who smoke or drink to give birth. To discern between the two possibilities, we turn to the PRAMS data.
Many Alaskans quit or reduce their smoking and drinking while pregnant (see Table 4). Smoking and drinking may have a direct effect on newborn health, but these are not new behaviors during pregnancy. Rather, more people who smoke and drink are giving birth. Perhaps paradoxically, this suggests the negative effect of the additional cash on birth outcomes is due to an improved in-utero environment. That is, the cash averts some miscarriages of less healthy fetuses and facilitates their live birth. To be clear, this is highly speculative, although prior work has found evidence that the Alaskan payments have improved in-utero health, reducing miscarriages (Singh 2023).
Smoking and Drinking Behavior of Pregnant People in Alaska, 1990 to 2010
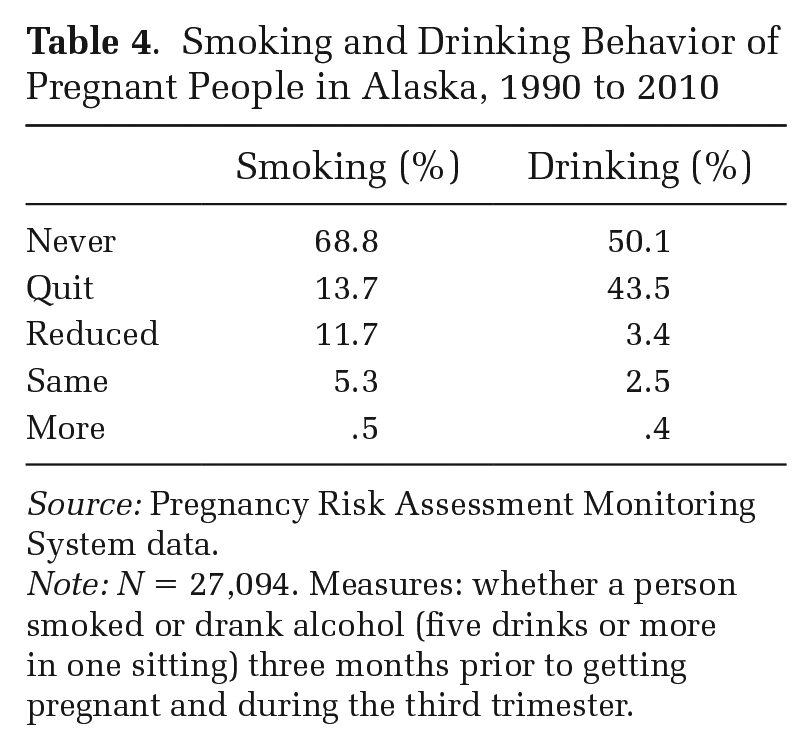
Source: Pregnancy Risk Assessment Monitoring System data.
Note: N = 27,094. Measures: whether a person smoked or drank alcohol (five drinks or more in one sitting) three months prior to getting pregnant and during the third trimester.
Discussion
Good health is foundational to well-being and is a precondition for thriving in social, educational, and occupational arenas. Yet from the very start of life, America’s inequitable social structure is embodied in the health of newborns; children born to parents of color and parents in poverty have worse health than children born to White and non-poor parents, on average (Forde et al. 2019). Across the political spectrum, advocates and politicians seek to eradicate these inequalities at birth. Determining what types of intervention can successfully aid newborns’ health is a critical endeavor, but, at this point, our well-evidenced theories do not equip us to make clear predictions about what kinds of interventions will work.
Our analysis focuses on a universal cash transfer. The Alaska PFD has a theoretical advantage to other income transfer policies for testing causal mechanisms: the PFD provides cash universally without changing the social structure or imbuing its recipients with stigma, allowing for a direct test of the effect of additional purchasing power on birth outcomes with no changes in social status, another key mechanism shaping health. Other features of the case facilitate causal estimation of the effect of cash received during pregnancy on birth outcomes. First, the payments are exogenous. Second, because the payment is universally given to Alaskan residents, we can precisely identify the treated population, which is often difficult when studying other types of policy interventions. Given that the dividend is universal, there are few worries about confounders or selection into receiving the dividend on the basis of personal and social characteristics used when modeling newborn health. Third, our analyses can exploit three sources of variation: marked annual variation in the cash transfer, variation within households within a year given household size, and variation in whether people receive the dividend while pregnant. Fourth, we can empirically account for how the dividend payments affect selection into pregnancy and childbirth on the basis of demographic characteristics, and thus avoid mis-specifying a selection effect as the effect of the cash during pregnancy.
Once we account for selection effects, we find very small, negative effects of a cash influx during pregnancy on birth outcomes; at the population level, additional cash results in a minuscule reduction in average birthweight and a very small increase in the odds of low birthweight. These effects are often, but not always, driven more by birthing parents with low educational attainment than high educational attainment, and more by Alaska Native parents than White parents. Our selection model accounts for differences in fertility rates by a number of demographic characteristics, but due to data limitations we cannot account for all characteristics. Additional analyses suggest these negative effects are due to a fertility increase among people with unaccounted-for characteristics, such as tobacco and alcohol consumption during pregnancy. Although perhaps initially counter-intuitive, this evidence suggests that income affects fertility by improving the in-utero environment, allowing a small number of higher-risk fetuses to be conceived and survive to birth who otherwise would not. Through this mechanism, we see an improvement in one birth outcome—survival to birth—but we detect no other improvements for infants’ health among either the full or socioeconomically disadvantaged populations.
Limitations
Despite the article’s strengths, there are some weaknesses. First, although Alaska is similar to many rural states, there remain concerns about generalizability. Anchorage is more similar to other U.S. cities than Alaska’s rural areas are to other U.S. rural areas, and our results for Anchorage alone are substantively similar. Nonetheless, Alaska is different from other states, particularly because the racially minoritized population contains many more Alaska Native peoples and smaller populations of other groups, compared to many other states.
Second, we cannot link people across births in the natality data. The data report parity, but we do not know birth intervals or other personal histories that may matter for fertility and birth outcomes. Furthermore, the natality data do not report on cohabitation, which became an increasingly common family structure during this period. The natality data also do not provide information on the birthing parent’s income. We rely on education to have a sense of individuals’ socioeconomic position.
Third, although our analysis can account for short-term fertility selection effects of the dividend on a birth cohort’s health, we cannot identify and model long-term effects the dividend has on the population’s mutable characteristics, such as educational attainment. If the dividend allows more people to attend and graduate from college, for instance, this change would have long-term effects on the health of future birth cohorts. Such an effect is outside the scope of our present analysis, but investigating longer-term effects is an important area for future research. 3
Implications
Our analysis provides empirical and theoretical insight into the relationship between socioeconomic resources and health. Empirically, we find that a universal cash transfer of substantial size—an increasingly popular policy proposal—made during pregnancy has no substantively meaningful effect on birth outcomes.
Why do we find no effect? We argued that current theories do not coherently guide our ability to identify effective interventions. We combine insights from existing theories to propose four components that must be considered in tandem to predict whether proposed interventions will work: (1) the type of resource, (2) the size of the resource, (3) whether providing the resource affects other causes of population health, and (4) the timing of the resource relative to the health process and outcome. The answers to these four questions will differ based on the health outcome and the context in which the intervention takes place. We revisit these components here to help highlight where our theoretical understanding is still incomplete.
We examined a unique program that increases economic resources without changing anything else, such as the distribution of resources or stigma or power. Considering components one and three together, we see an increase in money without any accompanying change to social structure or social status. This intervention alone was insufficient to improve newborn health. Considering the second component, the size of the resource, it is possible the payments were too small.
Another possible reason why the payments failed to change birth outcomes is that the resources come too late. Perhaps the health processes leading to poor birth outcomes—like accelerated aging through weathering—have already taken their toll. We do not have a strong empirical understanding of what health processes produce outcomes like low birthweight and preterm birth to guide the timing of our interventions, the fourth component. PFD payments do affect fertility rates (Cowan and Douds 2022), suggesting health and social processes inhibiting childbearing are altered by cash of this amount, but the processes resulting in poor outcomes once pregnancy begins may need intervention at an earlier time or of a different resource.
We do not detect marked changes in newborn health, but neither do scholars of other interventions (Almond et al. 2011; Hamad and Rehkopf 2015; Hoynes, Page, and Stevens 2011; Markowitz et al. 2017; Strully et al. 2010). We can speculate as to the cause of the small differences between studies—perhaps it was the mode of delivery or the nature of the control group. But what is abundantly clear is that the suite of interventions used in the United States does little to move the needle on newborn health. There is room for improvement, as other nations have proven (Blencowe et al. 2019; Ohuma et al. 2023), but such improvement would likely require interventions of a magnitude not yet seen in the United States.
Newborn health has lifelong consequences, and inequalities at this stage snowball over the life course. Identifying interventions to reduce these inequalities is of vital importance, and theory is a critical element of this process. That we cannot identify why the PFD failed to improve newborn health, or whether changing the resource amount or the timing of the intervention would be successful, highlights the need for more theorizing to “understand the relationship of socioeconomic factors to health in terms of the causes and consequences of specific forms of disease and biological function” (Herd et al. 2007:225). Theory helps us understand the social world, but we also need theory to understand how to change the world. Our key theories about the causes of health inequalities at this point are well supported. Now, we must move beyond explaining that socioeconomic resources matter to understanding how and when they matter—or not. We need to do this to ascertain what health problems require what intervention tool. If we are to inform social policy, we must make this shift.
Lastly, although we do not find appreciable effects of cash payments made during pregnancy on birth outcomes, such interventions may have other important benefits. For instance, receiving additional cash during pregnancy may reduce economic stress and improve birthing parents’ own physical or mental health outcomes. The cash may reduce the financial strain of pregnancy, labor, and delivery, reducing medical debt.
Cash interventions may also provide needed resources for pregnant people to exit unsafe relationships or living situations. These outcomes or others would be meaningful benefits of a cash intervention and potential improvements to reproductive autonomy, even if infants’ health at birth is not improved. However, our findings suggest that if the policy goal is to improve infant health at birth, then alternative interventions are needed.
Footnotes
Appendix
The full model specification for the model creating weights to account for fertility effects is as follows:
Acknowledgements
We received helpful feedback from Florencia Torche, Philip N. Cohen, Stephen Morgan, Andrew Gelman, Michael Hout, Paula England, Jeff Manza, Kenneth Wachter, Molly Martin, Tim Bruckner, Deborah Karasek, Eddie Hunsinger, Lawrence Wu, Siwei Cheng, Amanda Geller, Brad Hershbein, Alex Barnard, Michael Esposito, Ethan Raker, Jenna Johnson-Hanks, and Erica Hobby, as well as participants of the Population Association of America 2019 annual meeting, the Interdisciplinary Association of Population Health Science 2019 annual meeting, the Guttmacher Institute seminar series, the Texas A&M Sociology Colloquium, the NYU Wagner Speaker Series, and the University of Maryland Population Center Speaker Series. We thank the editors and anonymous reviewers for their feedback. We received research assistance from Anne Kou, Jessica Kalbfeld, Samantha Cunningham, Talya Nevins, and Ruby Steedle. We also thank Andy Katzman, Nathan Simon, Jonah Nissim, and Clay Wyndham-Douds.
Authors’ Note
This article builds off of previous work by the authors about the Alaska Permanent Fund, specifically, Cowan and Douds (2022). Table 1 and ![]() in this article are drawn from this previous article.
in this article are drawn from this previous article.
Funding
This work was supported, in part, by the Economic Security Project and the Cash Transfer Lab.