
Abstract
Why are some diseases more stigmatized than others? And, has disease stigma declined over time? Answers to these questions have been hampered by a lack of comparable, longitudinal data. Using word embedding methods, we analyze 4.7 million news articles to create new measures of stigma for 106 health conditions from 1980 to 2018. Using mixed-effects regressions, we find that behavioral health conditions and preventable diseases attract the strongest connotations of immorality and negative personality traits, and infectious diseases are most marked by disgust. These results lend new empirical support to theories that norm enforcement and contagion avoidance drive disease stigma. Challenging existing theories, we find no evidence for a link between medicalization and stigma, and inconclusive evidence on the relationship between advocacy and stigma. Finally, we find that stigma has declined dramatically over time, but only for chronic physical illnesses. In the past four decades, disease stigma has transformed from a sea of negative connotations surrounding most diseases into two primary conduits of meaning: infectious diseases spark disgust, and behavioral health conditions cue negative stereotypes. These results show that cultural meanings are especially durable when they are anchored by interests, and that cultural changes intertwine in ways that only become visible through large-scale research.
Disease stigma can be devastating. People with stigmatized diseases may endure psychological and physiological harms, avoid diagnosis and treatment, lose relationships and jobs, and even face a shortened life expectancy (Link and Phelan 2001; Major and O’Brien 2005; Pescosolido and Martin 2015). These harmful effects have inspired theories about why stigmas emerge, why some diseases are more stigmatized than others, and whether disease stigma has declined over time (Kurzban and Leary 2001; Link and Phelan 2001, 2014; Pescosolido and Martin 2015; Phelan, Link, and Dovidio 2008). Yet our ability to empirically test these theories has been hampered by the lack of comparable data on how stigma varies across diseases over time. Additionally, while stigma theory emphasizes stereotypes that operate above the level of the individual, most existing health stigma data come from individual self-reports (Hatzenbuehler, Phelan, and Link 2013; Link and Phelan 2014; Link et al. 2004).
To advance the existing literature, we use word embedding methods to analyze 4.7 million news articles and measure the stigmatizing meanings linked to 106 diseases across four decades. In line with contemporary theories of stigma as a macro-level phenomenon, our text data directly measure publicly circulating ideas about different diseases. Measuring stigmatizing meanings at scale reveals patterns that would be difficult to detect in studies of single diseases, allowing us to test theoretical predictions about how meanings vary across diseases and over time.
Drawing on theories of stigma’s sources (Kurzban and Leary 2001; Phelan et al. 2008), we develop hypotheses about how stigmatizing meanings vary by type of health condition. Existing theories imply that conditions with behavioral symptoms (e.g., mental illnesses) and those that are perceived to be preventable by healthy behaviors (e.g., lung cancer) will be most marked by connotations of immorality and negative personality traits, because the stigma surrounding these conditions is driven by norm enforcement. Existing theories also suggest that infectious diseases will be constructed as more disgusting than noncommunicable diseases, because stigma for these conditions is driven by contagion avoidance. We find support for each of these predictions, lending credence to theoretical models of stigma’s sources.
Additionally, current scholarship contends that some diseases may have less stigma because they receive more advocacy or are more medicalized (Conrad and Schneider 1980; Corrigan et al. 2012; Phelan 2005). We find inconclusive evidence on the relationship between advocacy and stigma, and no support for the prediction that medicalization reduces stigma.
Finally, some scholars have argued that disease stigma has declined over time, perhaps due to increasing advocacy and medicalization (Gove 1982; Green 2009; Phelan and Link 1998). We find that stigmatizing meanings of disease have indeed declined, but only for physical illnesses. In the past four decades, stigma has transformed from a sea of negative connotations surrounding most diseases to two primary conduits of meaning: infectious diseases spark disgust, and behavioral health conditions cue judgment.
These results show that stigmatizing meanings are especially strong and durable when they are anchored by stigmatizers’ interests. They also reveal that the stigmas targeting various diseases change together, as opposed to each disease requiring its own stigma-reduction campaign. These findings highlight the power of interests in shaping cultural meanings and the interrelatedness of cultural changes—patterns that only become visible through large-scale research.
Stigmatizing Meanings Of Diseases
Goffman (1963:3) defined stigma as an “attribute that is deeply discrediting,” which leaves the bearer “tainted” and “discounted.” In theory, any human difference, including gender, race/ethnicity, or sexuality, can be subject to stigma (Herek 2007; Reskin 2012; Schur 1984). But most sociological stigma research has focused on health conditions such as mental illness, HIV/AIDS, epilepsy, and cancer (Pescosolido and Martin 2015). Just as health issues are central to stigma research, stigma is a central concept for health research, highlighted in work on the social construction of illness and social determinants of health (Conrad and Barker 2010; Hatzenbuehler et al. 2013). While recognizing the broad reach of the stigma concept, for theoretical and methodological clarity, we focus on the measurement of disease stigma. Limiting our focus to diseases allows us to test theories about the sources of disease stigma and to conduct interpretable multivariate analyses, as diseases are relatively comparable to each other as cases in regression models.
Scholars have elaborated a multi-step stigma process in which (1) differences between people are labeled; (2) these labels are associated with derogatory meanings or stereotypes; and (3) people distance themselves from stigmatized individuals, who then (4) experience status loss and discrimination (Link and Phelan 2001; Pescosolido and Martin 2015). Our study focuses on the second step in this process—the derogatory meanings or stereotypes associated with various diseases. Diseases are loaded with intricate webs of meaning, many of which are notoriously negative. For instance, people with depression may be perceived as lazy or self-indulgent (Link et al. 1999), and obesity and overweight may connote moral failing (Arseniev-Koehler and Foster 2022).
Such meanings have consequences for later stages of the stigma process. People who adopt stigmatizing views may discriminate against individuals with health conditions. People with health conditions are further harmed when they “self-stigmatize,” internalizing these negative views. Both discrimination and self-stigma can cause psychological and physiological harms (Link and Phelan 2001; Major and O’Brien 2005; Pescosolido and Martin 2015). Therefore, understanding how stigmatizing meanings vary across diseases and over time can illuminate social processes of discrimination and exclusion and help us better target stigma-reduction efforts.
Why are some diseases more stigmatized than others?
Theoretical work on disease stigma makes implicit predictions about which types of disease will be most burdened by which stigmatizing meanings and which factors might dampen a disease’s stigma. Yet because existing studies rarely compare more than a handful of diseases or time periods, these theories have not been comprehensively tested. In this section, we first discuss two theorized drivers of disease stigma—norm enforcement and contagion avoidance—and explore their implications for which stigmatizing meanings will target which types of diseases. 1 Second, we explore processes theorized to dampen disease stigma. Theories of stigmas’ drivers and dampeners help us identify four key stigmatizing meanings, which we will use to create our dependent variables: immorality, negative personality traits, disgust, and danger. They also yield independent variables that could explain why some conditions attract more stigmatizing meanings than others: behavioral symptoms, preventability, infectiousness, medicalization, and advocacy. 2
Stigma Driver #1: Norm Enforcement
Several theories suggest that disease stigmas arise when aberrant behaviors trigger norm enforcement. One line of work, which we call power theories, focuses on how stigma serves stigmatizers’ interests (Clouston and Link 2021; Link and Phelan 2014; Phelan et al. 2008). From this perspective, some stigmatizers seek to punish deviance and enforce conformity (Goffman 1963; Phelan et al. 2008). In parallel, evolutionary theories posit that humans evolved to reject people who are unpredictable or not “good potential social exchange partners” (Kurzban and Leary 2001:192; see also Neuberg, Smith, and Asher 2000).
Norm-enforcement models imply predictions about which stigmatizing meanings will target which types of disease. First, because rule-breaking is often considered immoral, aberrant behaviors may be attributed to immorality (Goffman 1963; Morone 1997; Phelan et al. 2008). People who break one rule may be viewed as incapable of moral action and liable to break others (Becker 1963). Second, when considering why people act the way they do, observers tend to attribute behaviors to stable personal characteristics and dispositions (Jones and Nisbett 1972). People may also overgeneralize, assuming that someone who is deviant in one way also has other undesirable characteristics (Becker 1963). Deviant behaviors may therefore be attributed to negative personality traits (Corrigan et al. 2003; Goffman 1963; Phelan et al. 2008). Finally, norm-breaking behavior may be construed as dangerous (Jones et al. 1984; Link et al. 1999; Pescosolido 2013). Thus, when norm-enforcement mechanisms create stigma, we would expect diseases to be marked by connotations of immorality, negative personality traits, and danger.
Which diseases will be targeted by norm-enforcement stigmas? In theory, any illness may be norm-violating because U.S. culture valorizes power, independence, productivity, health, and beauty (Grue 2016; Susman 1994; Yang et al. 2007). Illness can also cause other forms of deviance by preventing the fulfillment of social roles in the workplace or the family (Crandall and Moriarty 1995; Kurtz and Giacopassi 1975; Parsons 1958). Additionally, the “just world” hypothesis suggests that because observers want to believe bad things only happen to bad people, they may conclude that illnesses are caused by negative characteristics or blameworthy behaviors (Jones et al. 1984; Lerner 1971; Susman 1994; Wortman and Dunkel-Schetter 1979). Physical illnesses may therefore be indirectly viewed as norm-breaking when observers make particular inferences about their causes or consider their effects on the fulfillment of other roles.
However, norm-enforcement mechanisms should produce especially heightened stigma for conditions where the symptoms themselves are non-normative behaviors. Because people with behavioral health conditions such as addictions, eating disorders, and other mental illnesses exhibit aberrant behaviors by definition, observers can perceive them as norm-breaking without making any additional inferences. Norm enforcement should therefore be more directly linked to behavioral health conditions than to chronic conditions.
Indeed, research consistently documents high levels of stigma for mental illnesses and addictions (Corrigan, Kuwabara, and O’Shaughnessy 2009; Pescosolido 2013; Pescosolido et al. 2010), especially when the symptoms are visible non-normative behaviors (Perry 2011; Phelan et al. 2000). But only a few studies have compared stigmas for multiple behavioral health conditions to multiple chronic conditions. In a sample mostly composed of student respondents, Tringo (1970) found a rough hierarchy in which respondents desired the most social distance from people with mental illness and alcoholism, followed by tuberculosis, and then several chronic conditions. Later studies replicated a hierarchy in which mental illnesses and addiction were most stigmatized, followed by infectious diseases and chronic conditions. These studies sampled students at various levels of schooling and included overlapping but not identical lists of between 10 and 27 conditions. Their measures of stigma included desire for social distance (Albrecht, Walker, and Levy 1982; Thomas 2000), perceived responsibility for the condition (Albrecht et al. 1982), and perceived sick role legitimacy (Kurtz and Giacopassi 1975).
These studies support the claim that behavioral health conditions trigger more stigma. But because each study includes a relatively small number of diseases, they do not allow for multivariate or statistical tests of this claim. They also cannot explore links between behavioral health conditions and the specific stigmatizing meanings derived from norm-enforcement theory (immorality, negative personality traits, and danger).
In addition to behavioral health conditions, norm-enforcement stigmas may target conditions that are seen as preventable. Some theorists suggest norm enforcement comes into play primarily when behaviors are perceived as voluntarily chosen (Jones et al. 1984; Phelan et al. 2008). These predictions align with attribution theory, which suggests people are more stigmatized when they are believed to be responsible for their conditions (Rush 1998; Weiner, Perry, and Magnusson 1988).
Surveys and experiments confirm that participants react less sympathetically to vignettes in which individual people are described as responsible for their illnesses (Corrigan et al. 2003; Crandall and Moriarty 1995; De Ruddere and Craig 2016). Studies at the disease level show that lung cancer is more stigmatized than other cancers (Marlow, Waller, and Wardle 2015), and a disease’s stigma is correlated with its perceived controllability (Pachankis et al. 2018; Weiner et al. 1988). These studies suggest preventable diseases are more stigmatized, but they are limited because they do not examine links between controllability and particular stigmatizing meanings.
Stigma Driver #2: Contagion Avoidance
Disease stigma may also arise through contagion avoidance. Power theories argue that stigmatizers avoid people who exhibit signs of poor health, “keeping away” from them in an effort to stay healthy (Phelan et al. 2008). Evolutionary theories also posit an evolved impulse to avoid infectious disease (Jones et al. 1984; Kurzban and Leary 2001; Pachankis et al. 2018).
Contagion-avoidance models yield additional predictions about which meanings will target which types of disease. Stigmas motivated by contagion avoidance are expected to be largely marked by meanings of danger and disgust (Crandall and Moriarty 1995; Kurzban and Leary 2001; Phelan et al. 2008). Both norm-enforcement and contagion-avoidance stigmas may produce fear, but disgust is more exclusively linked to contagion-avoidance mechanisms.
Fear of contagion can target non-contagious conditions, however irrationally (Jones et al. 1984; Kouznetsova et al. 2012; Phelan et al. 2008; Sontag 1990). Prior work has documented this type of “symbolic contagion” for cancer (Wortman and Dunkel-Schetter 1979), skin diseases (Hong, Koo, and Koo 2008), and obesity (Park, Schaller, and Crandall 2007). Evolutionary theorists suggest an evolved disgust reaction to signs of infection might favor false positives (Kurzban and Leary 2001). But we should expect contagion-avoidance stigmas to be stronger for infectious diseases than for chronic conditions.
Thus, contagion-avoidance theory suggests that infectious diseases will be strongly marked by connotations of disgust and danger. Several studies have found that some infectious diseases tend to be more stigmatized than chronic conditions (although less stigmatized than behavioral health conditions) (Albrecht et al. 1982; Fife and Wright 2000; Pachankis et al. 2018; Tringo 1970). But these studies are limited by looking at only one or two infectious diseases, and by using general measures of stigma rather than connotations of danger and disgust in particular.
Stigma Dampeners: Medicalization and Advocacy
While norm enforcement and contagion avoidance are theorized to drive the stigma for certain diseases, other theoretical work suggests factors that dampen disease stigma. First, some scholars have suggested that medicalization and geneticization—approaching and understanding illnesses as medical or genetic issues, as opposed to sins or crimes—would reduce stigma, either by decreasing people’s perceived responsibility for their conditions or inspiring optimism that conditions can be cured through medical treatment (Conrad and Schneider 1980; Phelan 2005; cf. Zola 1972). By reducing blame, medicalization might dampen norm-enforcement stigmas, attenuating the connotations of immorality, negative personality traits, and danger that target behavioral health conditions and preventable diseases.
Empirical research on the link between medicalization and stigma has been inconclusive. This work has primarily focused on mental illness. For example, the 1996 and 2006 General Social Surveys included vignettes describing individuals with symptoms of depression or schizophrenia. In an analysis of the 1996 survey, Martin, Pescosolido, and Tuch (2000) found that respondents who attributed mental illness symptoms to genetics reported significantly less desire for social distance from the person in the vignette. Analyzing both survey years, Schnittker (2008) found that genetic explanations were associated with less desire for social distance from people with symptoms of depression, but not from people with symptoms of schizophrenia, as attributing schizophrenia to genes increased attributions of dangerousness. In another nationally representative survey, vignette language framing mental illness as genetic had no significant effects on blame or social distance (Phelan 2005).
Only a few studies have examined the relationship between medicalization and stigma for conditions beyond mental illness. Qualitative work suggests that attributing epilepsy and migraine to neurological differences failed to reduce stigma, and may have reified the perception that people with these conditions are fundamentally different from others (Dwyer 1992; Kempner 2014). However, exposure to news articles attributing diabetes to genetics increased respondents’ support for public research funding (Gollust, Lantz, and Ubel 2010). Thus, prior scholarship finds conflicting effects of medicalization on stigma depending on the disease and study context.
Second, in addition to medicalization, other research suggests disease advocacy can reduce stigma (Clair, Daniel, and Lamont 2016; Corrigan et al. 2012), and stigma reduction is often a key goal for disease advocacy groups (Best 2017, 2019). Advocacy could potentially target both norm-enforcement and contagion-avoidance stigmas. Empirical evidence for the relationship between advocacy and stigma is limited, with some studies suggesting a risk of backlash against protests (Corrigan et al. 2012). No existing studies have measured advocacy and stigma across large numbers of diseases, so these predictions have not been quantitatively tested.
Has disease stigma declined over time?
In addition to considering how stigma varies across conditions, we ask whether disease stigma has changed over time. Some scholars have argued that stigma has ceased “to pose a severe problem” (Gove 1982:290) and that people with mental illnesses have begun to enjoy broad social acceptance (Crocetti 1974; see discussion in Pescosolido and Martin 2015; Phelan and Link 1998). A more recent book asked whether we have seen the “end of stigma” (Green 2009).
Some scholars base their predictions about stigma declines on arguments that Western societies have become more tolerant of outgroups (Janmaat and Keating 2019; Sullivan 2004). For instance, Charlesworth and Banaji (2019) found that from 2007 to 2016, Americans’ attitudes around sexual orientation, race, and skin tone moved toward neutrality. These arguments imply that disease stigma has declined similarly across all conditions.
Alternatively, disease stigma could have declined because medicalization and disease advocacy have increased. Existing studies have documented increases in medicalization (Conrad 2005; Conrad and Schneider 1980) and disease advocacy (Best 2012, 2019), and existing theories suggest that medicalization and advocacy can decrease stigma (Clair et al. 2016; Conrad and Schneider 1980; Corrigan et al. 2012; Phelan 2005). Thus, we might expect to see disease stigma declines that are explained by increases in medicalization or advocacy. But no one has tested these predictions with quantitative data.
Health stigma researchers have responded skeptically to claims that stigma has declined or disappeared, noting that people with stigmatized diseases still suffer measurable psychological and physiological harms (Link and Phelan 2001; Pescosolido and Martin 2015). Furthermore, the mixed empirical evidence for the effects of medicalization on stigma, described earlier, weakens arguments that increased medicalization has reduced stigma. But we have too little longitudinal data to resolve the debate.
For a small number of conditions, researchers have painstakingly collected comparable quantitative data over time. They have found, for instance, that the 1990s saw dramatic declines in some measures of AIDS stigma (Herek, Capitanio, and Widaman 2002). In contrast, mental illness stigma remained remarkably stable (Angermeyer, Holzinger, and Matschinger 2009; Pescosolido et al. 2021; Pescosolido et al. 2010; Schnittker 2008; Schomerus et al. 2012). If anything, survey respondents in 1996 were more likely to associate mental illness with violence than they had been in 1950 (Phelan and Link 1998; Phelan et al. 2000).
These studies were possible because researchers carefully replicated earlier survey questions with similar populations and identical question wording. Due to the expense of collecting representative survey data, we lack comparable measures for hundreds of other potentially stigmatized conditions over time. While stigma theories emphasize the importance of historical circumstances in shaping stigma, few studies can detect the resulting changes over time (Earnshaw et al. 2022; Phelan 2005:308).
Media Texts Reveal Public Culture
To test theoretical predictions about how stigma varies across diseases and over time, we turn to news media. Whereas survey data are usually limited to questions about a few diseases, media texts allow us to create scalable and standardized measures of stigma across a wide range of diseases. Furthermore, because media texts are archived over decades, they offer insights into the past that are unattainable through contemporary self-report data collection.
Media data have another advantage: they allow for direct measures of publicly circulating meanings. Sociologists of culture distinguish between public culture external to individuals and personal culture inside people’s heads (Lizardo 2017; Simko and Olick 2020). In the case of stigma, public culture includes stereotypes expressed in published texts, and personal culture includes stereotypes endorsed by individual people. The two types of culture are related, but not equivalent. For example, news content responds to public sentiment, but it is also shaped by economic pressures, organizational structures, and broad cultural traditions (Peterson and Anand 2004; Schudson 2002).
When researchers try to summarize public culture by surveying individuals, the results can be misleading (Jepperson and Swidler 1994; Simko and Olick 2020). One important reason that macro-level stigma diverges from average levels of individual-level stigma is that not everyone’s ideas are equally influential. For Link and Phelan (2001:378), “what matters is . . . whose cognitions carry sufficient clout in social, cultural, economic, and political spheres to lead to important consequences for the group that has been labeled as different.” To measure which stereotypes “the culture recognizes and deeply accepts” (Link and Phelan 2001:376), we need macro-level measures of the stigmatizing meanings that circulate in the public realm.
These public meanings have important consequences. Although the literatures have developed independently, stigma researchers and cultural sociologists identify similar pathways through which publicly circulating cultural constructions influence people’s beliefs and actions. First, people may internalize public culture. Media texts can influence public views (Chong and Druckman 2007; McCombs and Valenzuela 2020). Stigmatizers do not develop their attitudes in a vacuum; rather, they internalize publicly circulating stereotypes (Link and Phelan 2001; Pescosolido and Martin 2015). When they do, the result is “endorsed stigma” (Pescosolido and Martin 2015). Second, whether or not they endorse them, people can use publicly circulating stereotypes to draw boundaries, devalue, discriminate, and make distinctions seem natural (Lamont and Molnár 2002). Thus, publicly circulating meanings can be a tool to carry out “enacted stigma” (Pescosolido and Martin 2015).
Third, public culture shapes people’s beliefs about what others think and how others will interpret their actions (Swidler 2013). It is therefore a determining factor in “perceived stigma” (Pescosolido and Martin 2015). For instance, when people are diagnosed with a mental illness, they suffer harm when they believe others look down on the mentally ill (Link et al. 1989). Similarly, stigmatized groups may perceive stereotypes as “a threat in the air” that causes anxiety and impairs academic performance (Steele 1997). These “ambient stereotypes” or “messages in the culture” (Link and Phelan 2014:26; Phelan et al. 2014:21) can cause harm even to people who never experience direct discrimination.
Even though many of stigma’s negative effects are theorized to come about through the broader cultural climate (Link and Phelan 2014), stigmatizing meanings about disease are rarely studied at the macro level. 3 Stigma research on health and medical conditions often focuses on micro-level feelings and interactions, underemphasizing macro-level social processes of discrimination and exclusion (Hatzenbuehler et al. 2013; Link and Phelan 2001; Link et al. 2004; Sayce 1998). Health stigma researchers typically use surveys and interviews rather than directly measuring publicly circulating meanings in cultural texts (Link et al. 2004). Studies of the effectiveness of anti-stigma campaigns are often conducted at the individual level, seeing if individual participants endorse less stigmatizing attitudes after being exposed to campaign materials, rather than measuring change at the societal level (Clair et al. 2016; Pescosolido and Martin 2015; Stuart, Arboleda-Flórez, and Sartorius 2012). In contrast, we turn to media texts to measure the cultural constructions of diseases over time.
Data And Methods
Choosing and Classifying Diseases
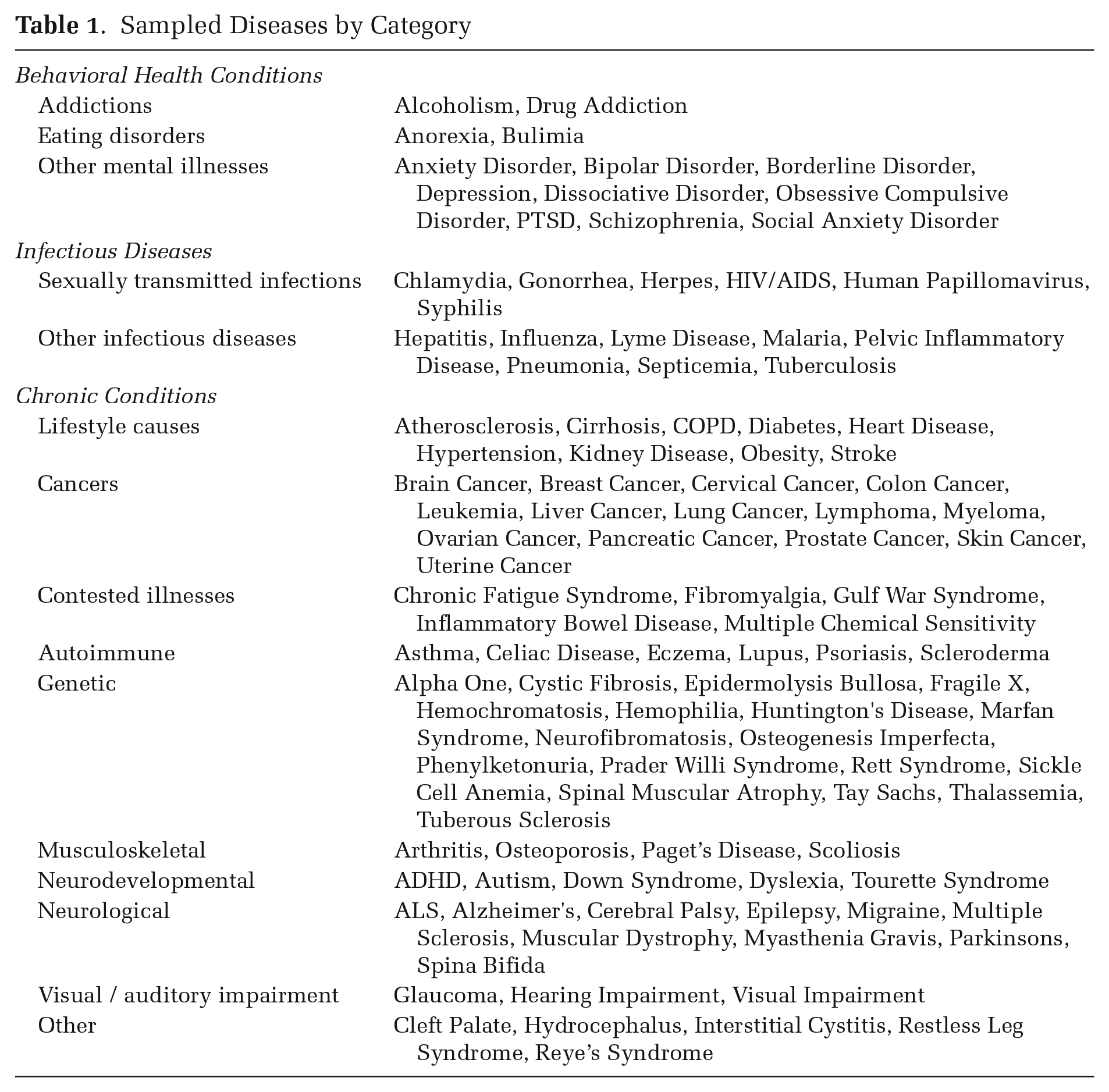
In choosing diseases for our study, we began with a list of 92 health conditions from Best (2019), which included major causes of death and disability and also rarer conditions that attracted substantial amounts of advocacy, medical research funding, or public attention. We added 24 conditions that were especially relevant to the study of stigma, including several mental illnesses, addictions, and sensory impairments. Beginning with this list of 116 diseases, we excluded 10 diseases that appeared too infrequently in our text data for stable embeddings. 4 The remaining 106 diseases include 13 behavioral health conditions, 14 infectious diseases, and 79 chronic conditions (see Table 1).
Sampled Diseases by Category
Sampling and Cleaning Text Data
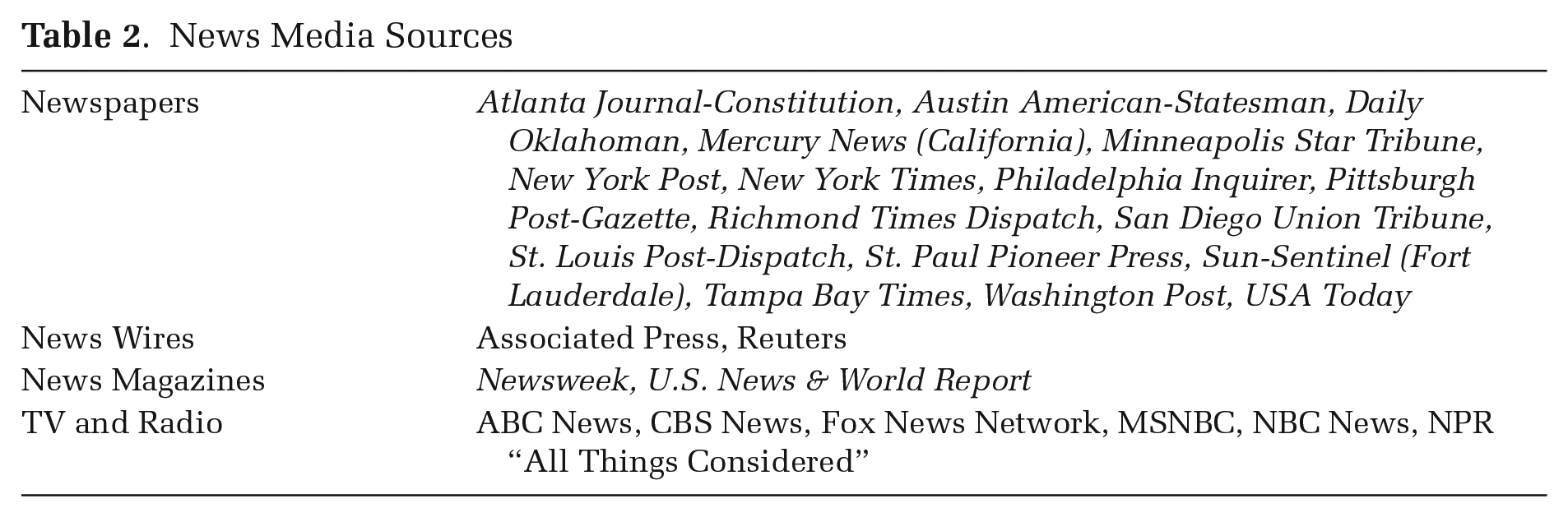
To develop comprehensive measures of the public meanings associated with different diseases, we sought out high-circulation news media outlets with varying ideological leanings in various parts of the United States. We collected data through LexisNexis, which archives many top media outlets and offers bulk downloading through an API to researchers from subscribing institutions. We first selected newspapers that were available in the LexisNexis API and appeared on one of several lists of the top-50 newspapers by circulation (infoplease.com 2007; Wikipedia 2019; Yahoo Finance 2017). This yielded a list of 17 newspapers from all regions of the country, including three of the top five papers (USA Today, the New York Times, and the New York Post). We added two major newswires (Reuters and the Associated Press) and two mainstream news magazines (U.S. News & World Report and Newsweek). Finally, we included transcripts of news broadcasts from three mainstream broadcast networks (NBC, ABC, and CBS), National Public Radio’s “All Things Considered,” and two partisan TV networks (Fox News and MSNBC), for a total of 27 news sources (see Table 2).
News Media Sources
Our subscription to the LexisNexis API imposed limits on the number of downloads per day, making it infeasible to download the entire text from each media outlet. Instead, we selected a sample that included approximately half the available articles from the selected publications, chosen to capture a wide range of articles while including the most relevant text for mapping disease stigma. We downloaded all news articles published by these outlets that referred to any of an intentionally broad list of health-related words. Our 166 search terms included various names for all the diseases of interest; broader terms including disorder, disease, syndrome, illness, and death; and a list of symptoms and aspects of life that are often medicalized, including sadness, sleep, and sex. We used regular expressions to search for multiple possible grammatical forms of these terms. Even for this sample, it took seven months to download our corpus due to the API limits. This process yielded a total of 4,711,524 articles from 1980 to 2018. To analyze these data across time, we divided the articles into three-year periods, beginning with 1980 to 1982. 5 We list the number of words and articles per time period in Table 3.
Number of Words and Articles Per Time Period
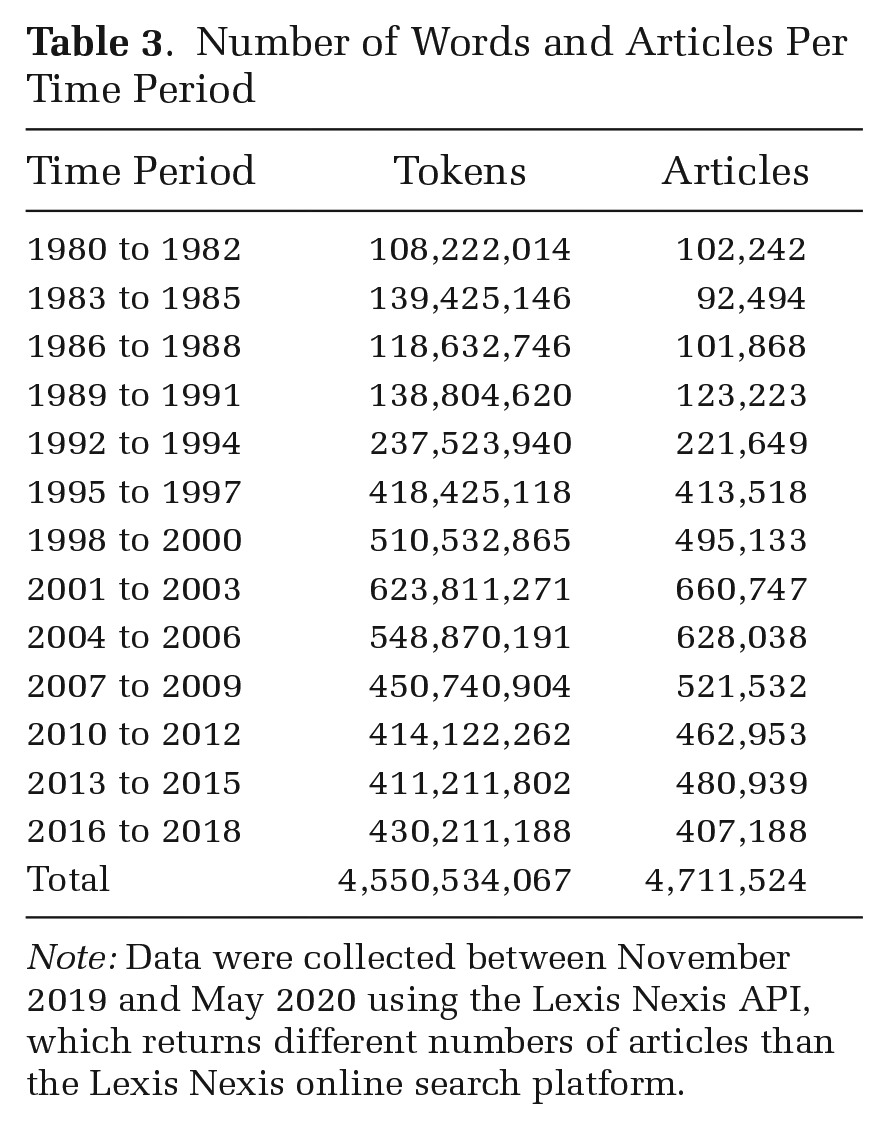
Note: Data were collected between November 2019 and May 2020 using the Lexis Nexis API, which returns different numbers of articles than the Lexis Nexis online search platform.
We took several steps to clean our text data. First, we combined multiple names for each disease into a single reconciled term. For example, all references to diffuse myofascial pain syndrome, fibromyositis, fibrositis, and FMS were replaced with “fibromyalgia” so we could track changes in the meanings associated with this disease, regardless of the term used to describe it. Second, we took steps to address the fact that certain words have multiple meanings. For example, we distinguished between references to depression as a mental illness and a financial crisis, stroke as a health event and a sports swing, and alcoholic as a description of a person or a drink. In some cases, we used regular expressions to perform this disambiguation (e.g., AIDS indicates a health condition, and “aids” is a verb; MS-13 refers to a gang and not multiple sclerosis; non-alcoholic describes a beverage and not a person with an alcohol use disorder). We also used the Lesk disambiguation algorithm as implemented in Python (Lesk 1986). This algorithm uses a word’s context in the data (e.g., whether “depression” was discussed in the context of health or finances) to disambiguate various potential meanings of a word. Finally, we removed punctuation, lowercased all text, and converted two- and three-word phrases into single terms, such that phrases like “New York” would be processed by Word2Vec as a single word (i.e., “New_York”). Additional details on text preprocessing are in the online supplement.
Measuring Stigma Using Word Embeddings
To analyze traces of stigma in text at scale, we used a computational text analysis approach called word embedding, which maps each word to an N-dimensional vector based on the contexts in which the word appears. 6 To create these word-vectors, we used the popular approach Word2Vec with Continuous-Bag-of-Words (Word2Vec-CBOW), which temporarily “hides” each word in the corpus, then tries to predict the hidden word by examining the words immediately before and after it (Mikolov et al. 2013). The algorithm learns from its mistakes, updating the word-vectors so it would be more likely to guess the correct word if it were to see this excerpt again.
To get a sense of the information the algorithm uses, imagine you are trying to guess the central word in the following excerpts, each of which appeared in our corpus in 1994. First, here are two excerpts describing what we will call condition A:
1: . . . turns describing what it is like when Mom is a [
2: . . . controversial this year it seems, which is substance_abuse, alcoholism or [
As the algorithm makes guesses about the hidden word, it might pick up on the fact that A is a condition humans can suffer from, A harms people’s children, A is related to addiction, and payments related to A are controversial.
In a high-quality word embedding, words that occur in similar contexts appear close together in the embedding space. For excerpt 1, you might have felt torn between guessing drug abuse or alcoholism; these two conditions would have similar vectors because they tend to appear in similar contexts. In fact, Condition A is drug addiction (“substance abuser” in excerpt 1, and “drug abuse” in excerpt 2). 7
Next, consider two windows around Condition B:
3: . . . we’ll offer you a glimpse into a state-of-the-art experiment in [
4: . . . farewell, an unspoken one, was because Joy was dying of
Here, we learned that B is something that requires treatment, B is the subject of scientific advances, and B affects individual people who must say sad farewells. Condition B is breast cancer. In excerpt 3, the discussion of radiation, chemotherapy, and scientific research might have led you to guess skin cancer instead; its vector would be similar to the vector for breast cancer.
The vectors for drug abuse and breast cancer would share some similarities, as both are medicalized conditions that can affect human beings. But their meanings diverge in other ways; for example, these excerpts and others like them might imply a link between drug addiction and immorality, and between breast cancer and morality.
These differences and similarities between word-vectors often have substantive meaning (Mikolov et al. 2013). For example, subtracting the word vector for “moral” from “immoral” can yield a vector representing the relational concept of morality. These substantively meaningful vectors, operationalized by drawing lines between clusters of words with opposite meanings, are called semantic dimensions. As we will describe, we extracted semantic dimensions for the stigmatizing meanings we derived from stigma theory: immorality, negative personality traits, disgust, and danger. 8
Training Bootstrapped Word Embeddings
We implemented Word2Vec-CBOW in the Python package Gensim (Řehůřek and Sojka 2010). Tests for selecting hyperparameters, described in the online supplement, favored a context window at 10 words before and after each target word and 300-dimensional vectors, matching previous work (Mikolov et al. 2013).
Word embeddings may be unstable when they are overly influenced by the inclusion of individual documents. To overcome this instability, following Antoniak and Mimno (2018), we trained 25 bootstrapped embeddings in each of the 13 time periods, for a total of 325 embeddings. To create each bootstrapped embedding, we randomly resampled articles in the time window with replacement until the new sample was the same size as the original. To prevent Word2Vec from learning low-quality word-vectors, and to avoid stigma scores that were overly influenced by individual news articles, we only include a disease/time period in our analyses if the disease name appeared at least 50 times in each of at least 20 of 25 bootstraps. Each variable (e.g., a disease’s score for disgust in the 1980 to 1982 time period) is the mean across all bootstrapped embeddings in which the disease name appeared at least 50 times. We use these bootstraps to create confidence intervals for Figures 3 and 4.
To ensure our final trained embeddings were of sufficiently high quality, we compared cosine similarities from our models to human-rated similarities between words from SimLex-999 (Hill, Reichart, and Korhonen 2015). The mean Spearman correlation between human-rated similarities and cosine similarities across our models was .36 (SD = .02), and all p-values were less than .0001, comparable to other published models (Hill et al. 2015). See the online supplement for further details on our validation procedures.
Dependent Variables: Operationalizing and Validating Stigma Dimensions
We set out to operationalize four stigmatizing meanings derived from existing theory: immorality, negative personality traits, disgust, and danger. For each of these stigma dimensions, we selected groups of “anchor words” that we expected to find at the dimension’s two poles. For example, anchor words for one side of the disgust dimension included repulsive, disgusting, and gross, whereas anchor words for the other side included appealing, captivating, and enticing. We averaged the word-vectors for the stigmatizing pole (e.g., disgust) and subtracted the averaged word-vectors for the non-stigmatizing pole (e.g., attractiveness). This yielded a vector corresponding to the stigma’s meaning—for example, a line from disgusting to attractive. The online supplement explains how we selected anchor terms and validated our dimensions.
We then measured each disease’s position in relation to each stigma dimension using cosine similarity. 9 A more positive score suggests the disease lies closer to the stigmatized pole of the dimension (e.g., immorality), and a more negative score suggests the disease lies closer to the non-stigmatized pole of the dimension (e.g., morality). We standardized each disease’s score against the scores for all other vocabulary words in the embedding for that time period. 10 The final scores can be interpreted as the number of standard deviations more (or less) stigmatized a word is compared to the average word in the vocabulary. Thus, a disease with a disgust score of two is two standard deviations closer to “disgusting” than the average word in the corpus in that time period. A disease with a disgust score of negative .5 is half a standard deviation closer to “attractive” than the average word.
We took several steps to validate these dimensions and stigma scores. First, we tested how well our dimensions classified words that we expected to be positioned at one or the other end of each dimension (e.g., as disgusting or enticing); accuracy rates ranged from 89 to 95 percent. Second, to assess the face validity of our dimensions, we examined the words in the vocabulary that mapped closest to each pole of each dimension across various time points, finding that their meanings aligned with our stigma concepts. Third, we drew on Pachankis and colleagues’ (2018) survey of stigma experts. This study, the most extensive comparison of stigma across conditions to date, measured the stigma of 93 conditions by surveying experts (authors of highly-cited stigma publications). 11 Conditions’ scores on three of our stigma measures were positively correlated with the stigma experts’ ratings of social distancing, with Spearman correlation coefficients of .36 (disgust), .54 (negative traits), and .60 (immorality); all p-values < .01. In addition to social distance, Pachankis and colleagues asked about several specific stigmatizing meanings. Our measures of immorality and disgust were correlated with parallel rankings by the experts in Pachankis and colleagues’ study, with Spearman correlation coefficients of .55 (p < .0001) and .46 (p < .0001), respectively. (Pachankis and colleagues did not include a parallel measure for our negative traits dimension.)
In contrast, our danger dimension had weaker Spearman correlations with the Pachankis ratings for social distance (.30, p < .05) and dangerousness (.24, p < .10). We concluded that our danger dimension may have conflated two ways in which diseases are constructed as dangerous: people with a disease may be described as dangerous to others (e.g., a perceived risk of violence), or a disease may be dangerous to people afflicted with the disease (e.g., a fatal disease). Given this ambiguity and the relatively weak correlations with human rankings, we decided to exclude the danger dimension from our analyses. We provide results for danger only in the online supplement, and we suggest these results be interpreted with caution.
Because one of our goals is to observe changes in disease stigma, we need to be confident that our stigma dimensions are capturing the same concepts over time. We standardized all stigma scores within time periods so that if media texts have generally become more or less tinged by connotations of disgust, immorality, or negative personality traits over time, we would not falsely conclude that these patterns were specific to diseases. 12 We also explored the possibility that the meanings of our dimensions might have changed over time. First, we examined the most similar words to each pole of each dimension in the first, middle, and last time periods and concluded they captured similar clusters of meanings. Second, we selected a batch of words related to homicide, which we expected to have consistently high stigma scores over time. These terms all had stable, high scores on all three stigma dimensions over time, increasing our confidence that our dimensions were picking up stable stigmatizing meanings. Additional details on all validation steps are available in the online supplement.
Before creating our final dependent variables, we asked whether our three validated stigma dimensions (immorality, negative personality traits, and disgust) captured distinct or overlapping meanings of disease. Diseases’ disgust scores were positively but not overwhelmingly correlated with their immorality and negative traits scores (r = .61 and .63, respectively). Diseases’ immorality and negative traits scores were extremely highly correlated (r = .86), suggesting a close relationship between these two dimensions of disease stigma. This connection makes sense, given that both stigmatizing meanings are theorized to result from norm-enforcement mechanisms. Because of their empirical correlation and theoretical connection, we averaged diseases’ scores for immorality and negative traits to create an index we call judgment. The index has extremely high Cronbach’s alpha (.911) and Spearman-Brown coefficients (.927), suggesting the scale is reliable. Our final dependent variables, therefore, are judgment and disgust.
Independent Variables
Next, we operationalized independent variables to explore why some diseases are more stigmatized than others and how these patterns vary across time. From norm-enforcement theory, we derived the hypothesis that behavioral health conditions would be most marked by judgment. We therefore distinguish behavioral health conditions (addictions, eating disorders, and other mental illnesses) from physical illnesses. The phrase “behavioral health” is sometimes used broadly, including any behaviors that can affect people’s health (e.g., smoking or exercise) (Matarazzo 1980). We use “behavioral health conditions” more narrowly to describe conditions marked by non-normative behaviors: addictions, eating disorders, and other mental illnesses (University of Massachusetts Global n.d.).
Norm-enforcement theory also suggests diseases will be targeted by judgment when people are believed to be responsible for their conditions. We initially operationalized an embedding-based measure of culpability, but it did not pass validation tests. Instead, we draw on Phelan and colleagues’ (2004) measures of how preventable dozens of diseases are. We expect that when a disease can be prevented by changing behaviors (e.g., by avoiding smoking), people suffering from the disease will be perceived as more responsible for their condition. These scores range from 1 (least preventable) to 5 (most preventable). 13 These measures were available for 31 of the diseases in our study.
Contagion-avoidance theory suggests that infectious diseases will be marked by connotations of disgust. To test this theory, we distinguish infectious diseases from chronic illnesses and behavioral health conditions.
Next, we operationalized variables predicted to reduce stigma. Medicalization captures the extent to which a disease is discussed in the context of medicine and is operationalized as the cosine similarity between a disease and the average of 16 word-vectors about medicine (e.g., doctor, prescription, pharmacology, medicine, and medication), standardized within time periods.
Advocacy is a measure of nonprofits and lobbying expenditures targeting each disease. This variable draws on data from Best (2019), which we supplemented with additional data on addictions, auditory and visual impairments, and several mental illnesses. Drawing on IRS data compiled by the National Center for Charitable Statistics, we used organizations’ names to identify charities targeting each disease and track the lobbying expenditures they reported to the IRS. 14 We collected additional data on lobbying expenditures from the Senate Lobbying Disclosure Act Database. We used these data to calculate (1) the number of nonprofits targeting a given disease in a given time period, and (2) their total lobbying expenditures, adjusted for inflation. 15 We standardized the nonprofits and lobbying variables with respect to other diseases in the time period. A score of 1 indicates that, on average, a disease had 1 standard deviation more nonprofits or lobbying than other diseases in that time period. We then averaged them to create a single advocacy index. This index has a Cronbach’s alpha of .82 and a Spearman-Brown coefficient of .83. For details on these data, see Best (2019:174–78). Advocacy data are only available from 1989 to 2013.
Time is our next independent variable. As noted earlier, we segmented our data into three-year time periods. Our analyses include a linear time trend (a running count of time periods: 1980 to 1982 = 1, 1983 to 1985 = 2, through 2016 to 2018 = 13) to examine whether stigma has declined across time.
Embedding scores can be influenced by the frequency with which a term appears in the corpus (Loon et al. 2022). We therefore include a control variable, word count. This variable is a count of the number of times the disease was mentioned in the corpus, standardized within time periods. This variable’s mean was zero, indicating that the mean word count for diseases in our study equaled the mean word count for all words in the corpus. Table 4 presents descriptive statistics for all variables used in the analysis.
Descriptive Statistics
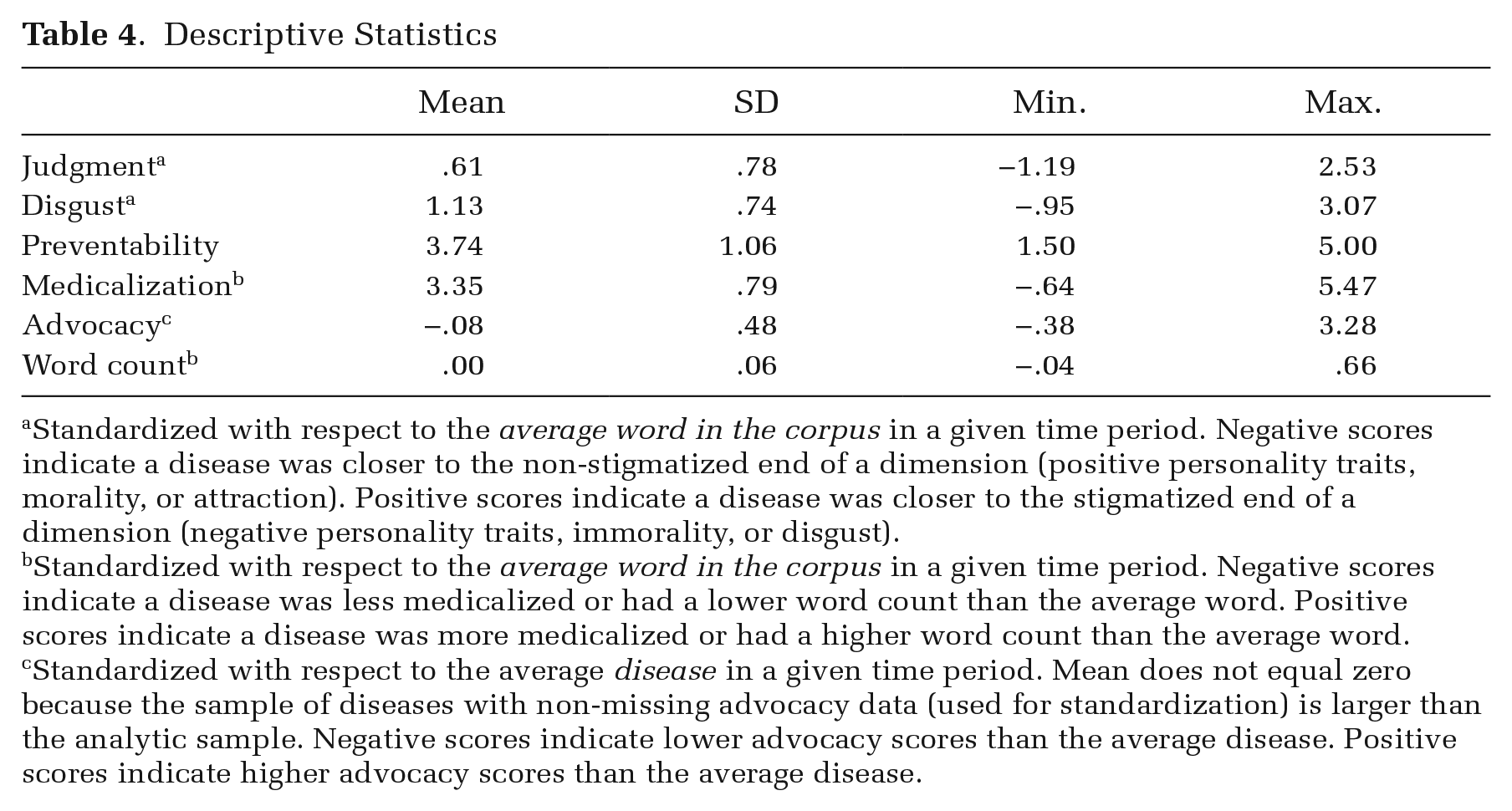
Standardized with respect to the average word in the corpus in a given time period. Negative scores indicate a disease was closer to the non-stigmatized end of a dimension (positive personality traits, morality, or attraction). Positive scores indicate a disease was closer to the stigmatized end of a dimension (negative personality traits, immorality, or disgust).
Standardized with respect to the average word in the corpus in a given time period. Negative scores indicate a disease was less medicalized or had a lower word count than the average word. Positive scores indicate a disease was more medicalized or had a higher word count than the average word.
Standardized with respect to the average disease in a given time period. Mean does not equal zero because the sample of diseases with non-missing advocacy data (used for standardization) is larger than the analytic sample. Negative scores indicate lower advocacy scores than the average disease. Positive scores indicate higher advocacy scores than the average disease.
Statistical Analyses
We constructed a dataset with one observation for each disease in each three-year time period. For instance, the line of data for schizophrenia in 2010 to 2012 includes schizophrenia’s scores for judgment and disgust, the level of advocacy targeting schizophrenia, and a dummy variable indicating that schizophrenia is a behavioral health condition.
To account for the hierarchical structure of the data (diseases observed in multiple time periods), we use linear mixed-effects regression models with judgment and disgust as dependent variables. Mixed-effects models are appropriate for our repeated measures data because they allow for correlation within diseases across time (Rabe-Hesketh and Skrondal 2008). We include a random intercept for each disease to account for unmeasured disease-level variation in stigma scores. The model for the stigma score yij of disease j in time period i is

where x1ij through xpij are covariates,
The models in Table 6 include a linear time trend. As a robustness check, the online supplement presents results from models that also include a quadratic time trend and random slopes that allow the time effect to vary across diseases. Results are substantively similar. Because we do not have an explicit scientific interest in estimating between-disease variation in time trends, to ease interpretation of the models, we do not include random slopes in the models presented in the main text.
Medicalization and advocacy vary both within and between diseases, so we tested whether their within- and between-disease effects differed (Rabe-Hesketh and Skrondal 2008). We found significant differences for the advocacy coefficients. We separate out these between- and within-disease effects by including two advocacy variables in our regression models: the disease’s mean level of advocacy across time periods and deviation from the disease-specific mean in a given time period. This analytic strategy allows us to model within-disease effects as in a fixed-effects model, while also including covariates that are constant within diseases (Bell, Fairbrother, and Jones 2019).
In all models, positive coefficients indicate that an independent variable is associated with higher levels of stigma. All figures present raw data, not estimates from regression models.
Results
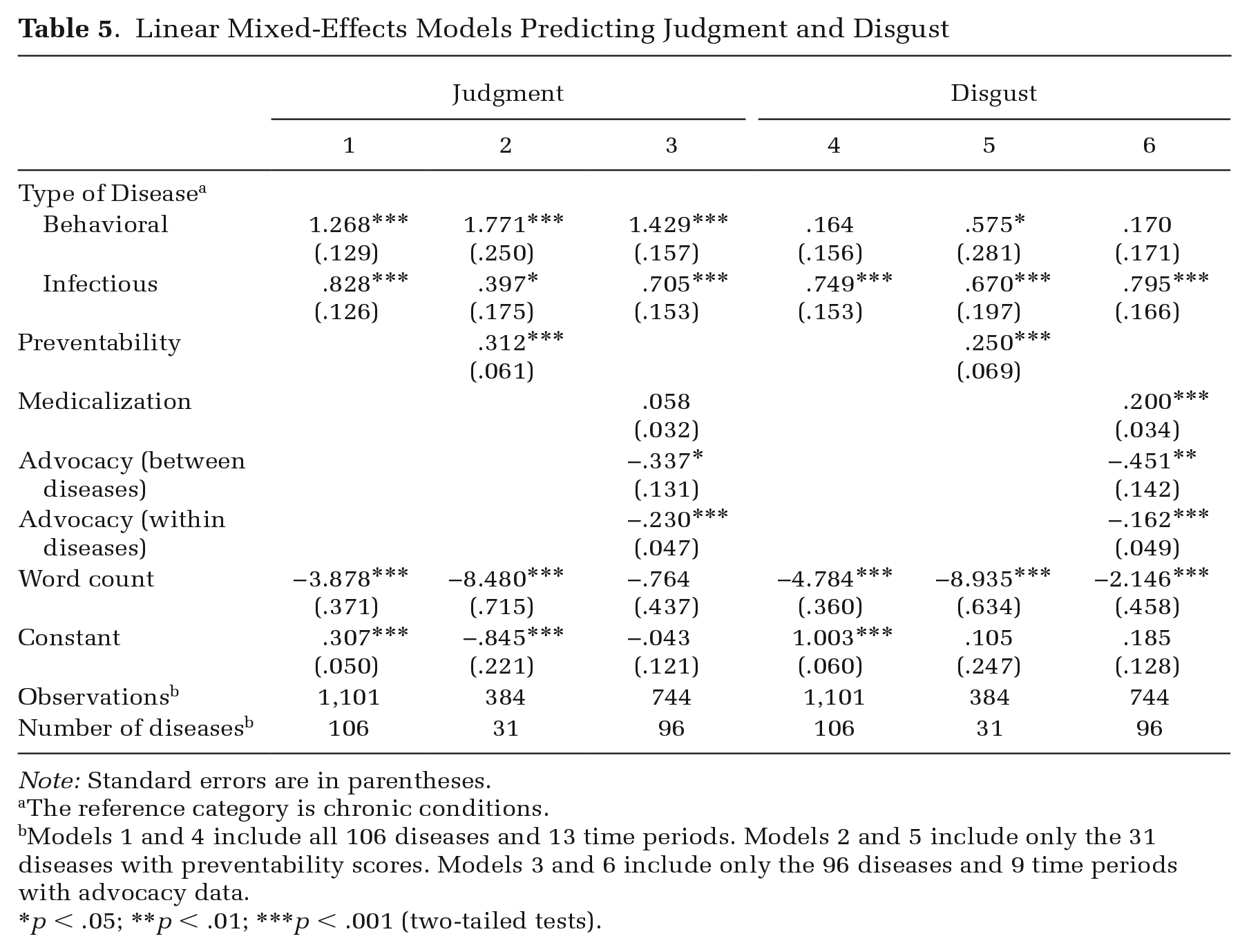
In the following sections, we begin by testing predictions about how stigmatizing meanings vary across diseases. Table 5 shows results of linear mixed-effects regressions predicting diseases’ judgment and disgust scores. Some models in Table 5 include fewer diseases and time periods due to limited availability of data on preventability (Models 2 and 5) and advocacy (Models 3 and 6). Thus, changes in coefficients from one model to the next reflect not only the inclusion of additional variables, but also the changing analytic sample. Figures 1 and 2 show behavioral, infectious, and chronic diseases’ mean judgment and disgust scores during the three most recent time periods (2010 to 2018). 16 Within groups, individual diseases are sorted from most to least stigmatized. Next, we ask how disease stigma has changed over time. Table 6 shows results of linear mixed-effects regressions predicting judgment and disgust scores over time, and Figures 3 and 4 show time trends in judgment and disgust scores.
Linear Mixed-Effects Models Predicting Judgment and Disgust
Note: Standard errors are in parentheses.
The reference category is chronic conditions.
Models 1 and 4 include all 106 diseases and 13 time periods. Models 2 and 5 include only the 31 diseases with preventability scores. Models 3 and 6 include only the 96 diseases and 9 time periods with advocacy data.
p < .05; **p < .01; ***p < .001 (two-tailed tests).
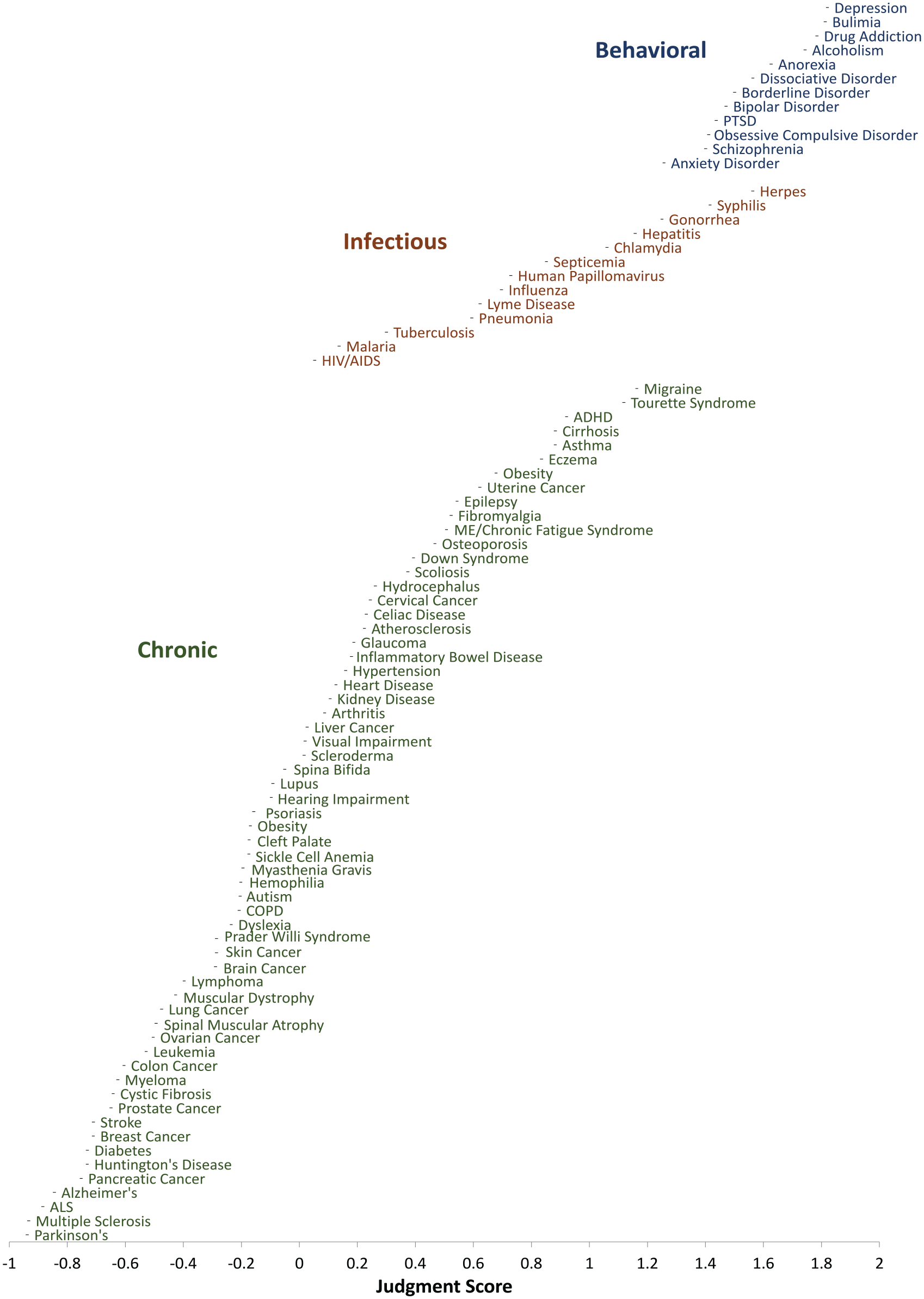
Judgment Scores for Behavioral, Infectious, and Chronic Diseases, 2010 to 2018
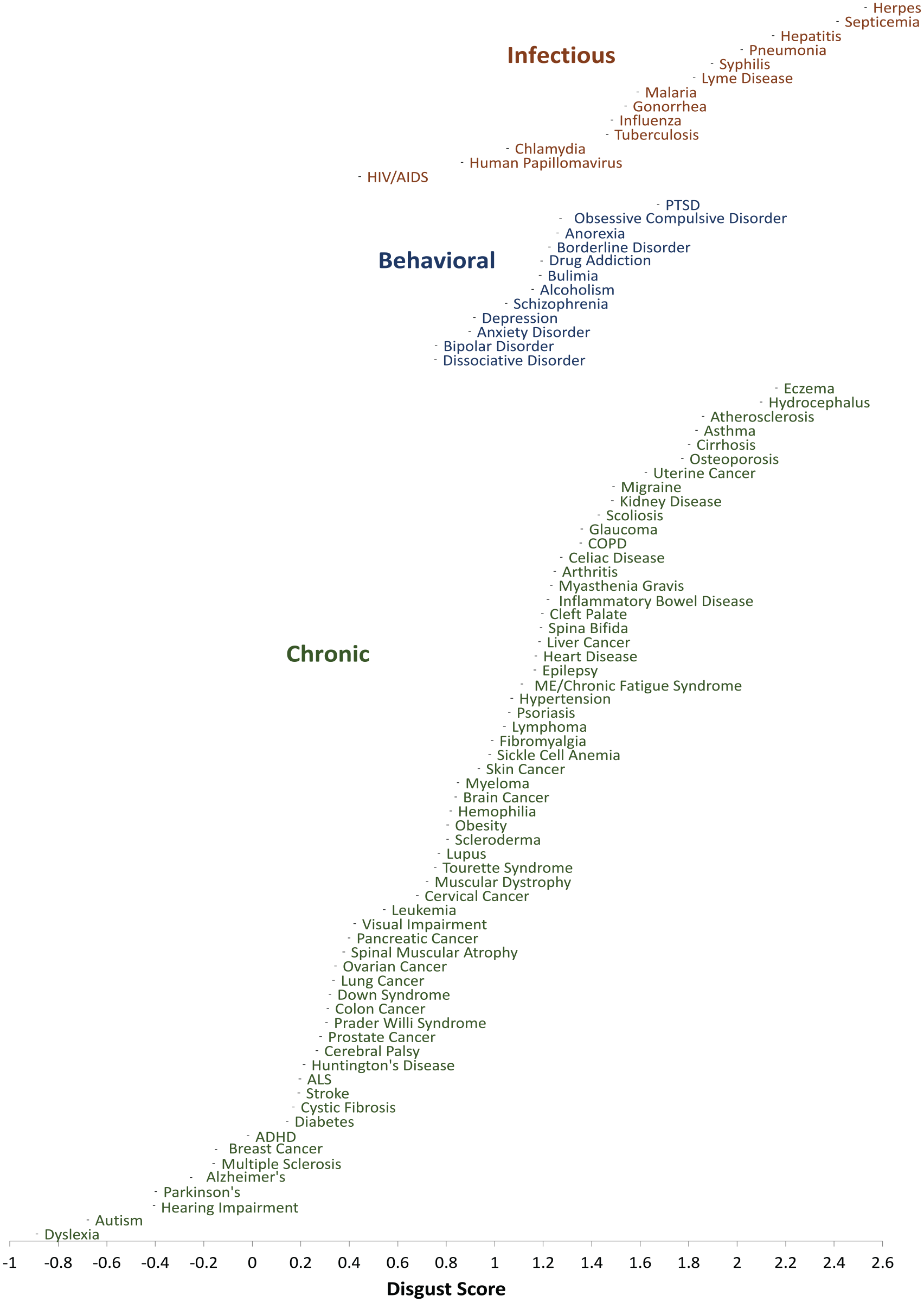
Disgust Scores for Infectious, Behavioral, and Chronic Diseases, 2010 to 2018
Linear Mixed-Effects Models Predicting Judgment and Disgust Over Time
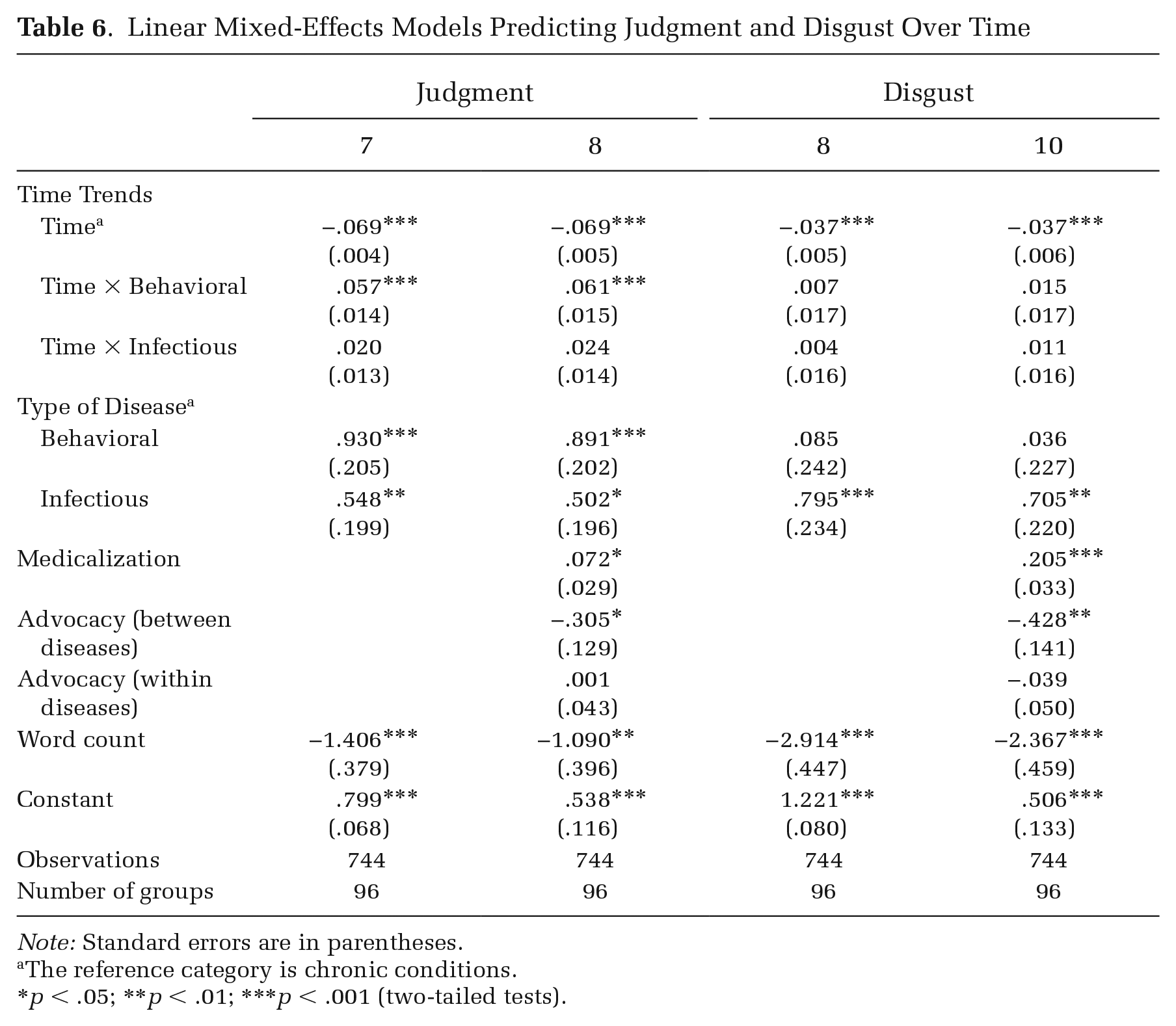
Note: Standard errors are in parentheses.
The reference category is chronic conditions.
p < .05; **p < .01; ***p < .001 (two-tailed tests).
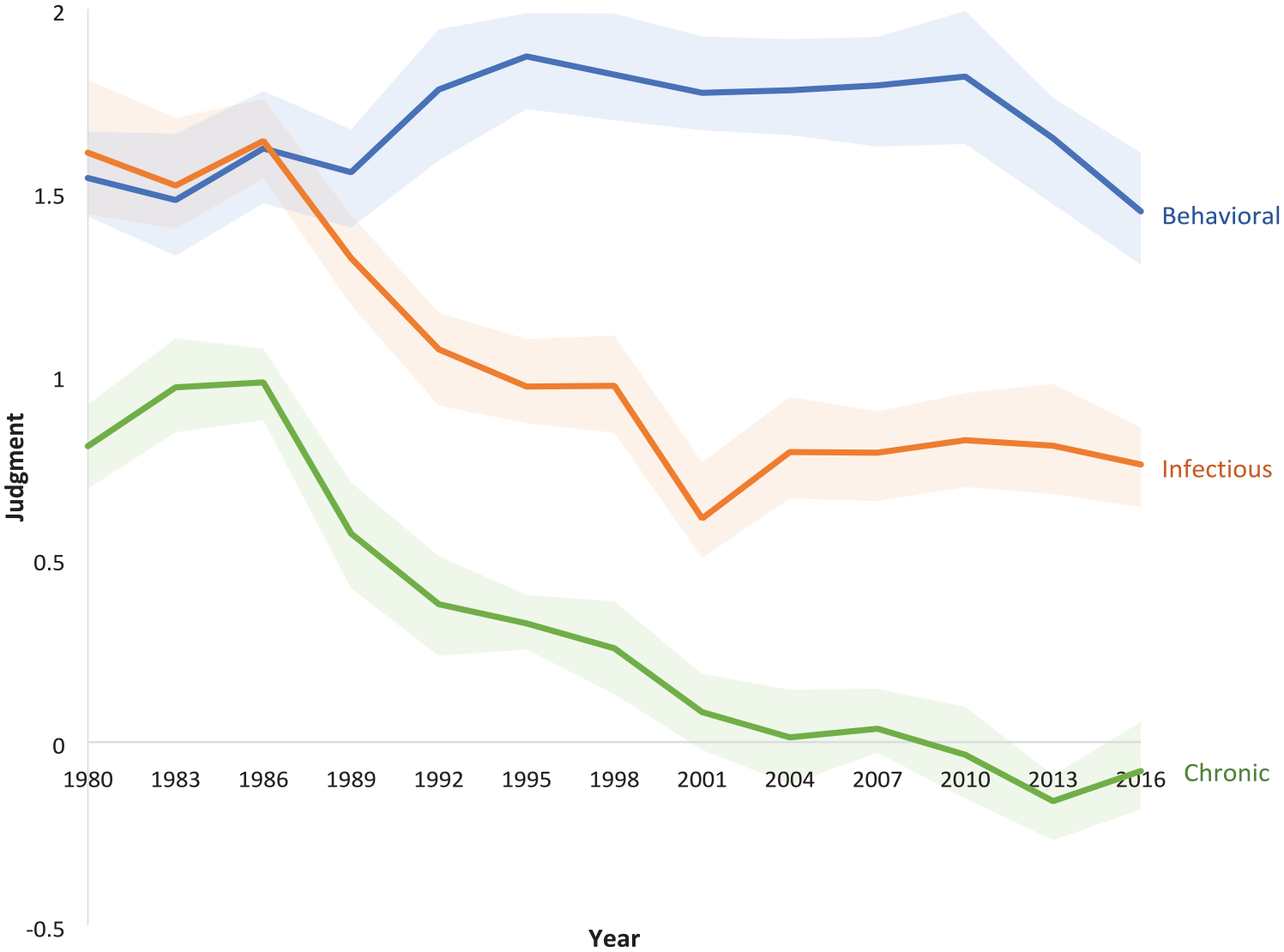
Judgment Scores for Behavioral, Infectious, and Chronic Diseases over Time
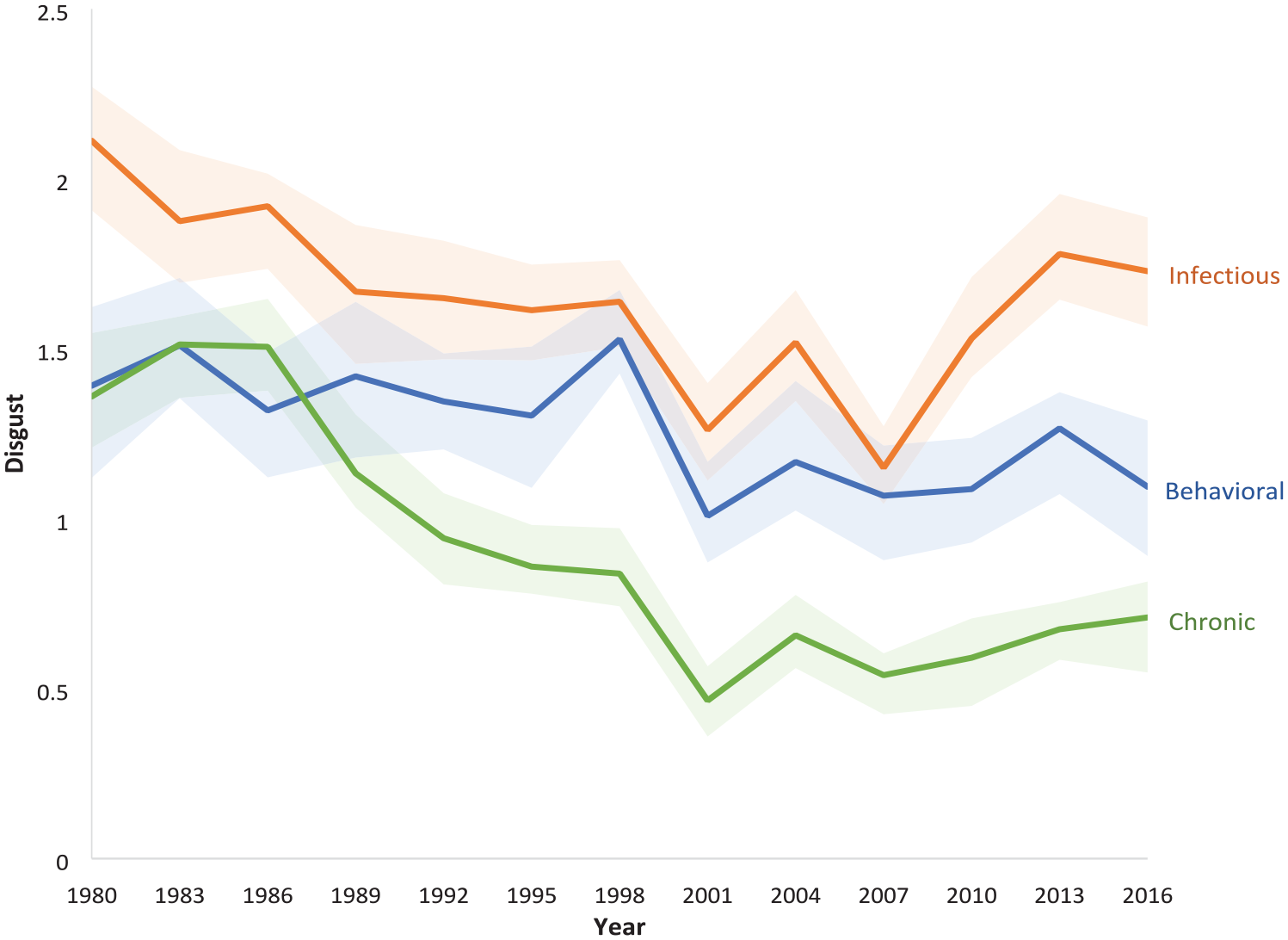
Disgust Scores for Behavioral, Infectious, and Chronic Conditions over Time
Testing Implications of Norm-Enforcement Theories
Norm-enforcement theories imply that behavioral health conditions will attract connotations of judgment (immorality and negative personality traits). Indeed, behavioral health conditions cluster together at the top of Figure 1: each of the 12 diseases in this category is, on average, at least 1.2 standard deviations more linked to judgment than the average vocabulary word in the corpus. Among all other diseases in our study, only syphilis and herpes attract more judgment than the least stigmatized behavioral health condition (anxiety disorder).
While behavioral health conditions are in a class of their own, looking at the most stigmatized infectious and chronic conditions provides further evidence for the role of non-normative behaviors in driving judgment. The infectious diseases that score most highly for judgment are all sexually transmitted, and therefore may be targeted by moralistic judgments about non-normative sexual behavior. Among chronic conditions, we observed especially high levels of judgment targeting Tourette Syndrome, which has behavioral symptoms, and migraine, which is known to evoke negative stereotypes and suspicions of malingering (Kempner 2014).
Regression analyses confirm that the link between behavioral health conditions and judgment is statistically significant. In Models 1 through 3 in Table 5, behavioral health conditions have significantly higher judgment scores than do chronic conditions (the reference category). Infectious diseases also have heightened links to these stigmatizing connotations, but the coefficients are much smaller than those for behavioral health conditions.
The links between behavioral health conditions and judgment become even clearer when we examine words with similar connotations. 17 For instance, in the 1998 to 2000 time period, three of the 10 non-disease words closest to bipolar disorder were “con_man,” “convicted_felon,” and “defiant.” Four of the ten non-disease words closest to alcoholism were “ex-con,” “aimless,” “underworld,” and “womanizing.” These semantic neighbors highlight behavioral health conditions’ cultural links to deviant social roles, negative personality traits, and moral judgment.
Norm-enforcement models also predicted that preventable diseases would attract more judgment because people with these diseases are often blamed for their conditions. The positive and significant preventability coefficient in Model 2 in Table 5 confirms that more preventable diseases had stronger connotations of judgment. The effect is sizeable; each one-point increase in a disease’s preventability score (on a scale from 1 to 5) is associated with a .31 standard deviation increase in a disease’s judgment score. The patterns in Figure 1 illustrate these trends. For instance, among cancers, uterine, liver, cervical, and skin cancers attract the most judgment, likely due to their perceived controllability by avoiding sun exposure, drinking, and HPV infection. The relatively high levels of judgment targeting sexually transmitted infections could also be linked to perceived personal responsibility for these conditions. 18
Because our data allow direct comparisons across diseases, we can put these different sources of stigma in perspective. While blame for controllable conditions does seem to increase judgment, it does not produce stigmas as severe as those targeting addictions, eating disorders, and other mental illnesses (see Figure 1). The most judgmental language is reserved for conditions in which the symptoms are non-normative behaviors.
Testing Implications of Contagion-Avoidance Theories
Contagion-avoidance theories imply that infectious diseases will arouse disgust. Figure 2 shows infectious, behavioral, and chronic diseases’ disgust scores for 2010 to 2018. Infectious diseases appear at the top because, as predicted, their mean levels of disgust were higher than either of the other disease categories. Models 4 through 6 in Table 5 further confirm this prediction: infectious diseases’ disgust scores are significantly higher than those for chronic conditions (the reference category). All else equal, infectious diseases’ disgust scores are predicted to be between .67 and .795 standard deviations higher than those of chronic diseases. In contrast, in most models, behavioral health conditions’ disgust scores are not significantly different than those for chronic diseases. 19 We did not hypothesize a link between preventability and connotations of disgust, but preventability does have a significant and positive coefficient in Model 5.
Testing Theories about Stigma Dampeners: Medicalization and Advocacy
We find no support for the theorized link between medicalization and reduced stigma. In fact, diseases that are discussed in a more medicalized context tend to attract more judgment and disgust than do other diseases (see Table 5, Models 3 and 6). These patterns may stem from the fact that all the diseases in our sample are quite medicalized; we are not comparing conditions viewed as medical issues to those viewed as sins or crimes (e.g., adultery or homicide). Additionally, diseases may end up with lower medicalization scores because they have been constructed as poignant afflictions or philanthropic causes and therefore appear in human-interest stories or requests for donations in obituaries. More stigmatized diseases might only appear in medical-related contexts.
Other scholars have suggested that disease activism might ameliorate stigma. Because we observe different effects of advocacy within and between diseases in some models, we separate out these two patterns (see Table 5, Models 3 and 6). The mean advocacy variable shows that diseases with higher average levels of advocacy across time tend to attract less judgment and disgust. A disease that, averaged across time periods, had one standard deviation more nonprofits and lobbying than another disease would be predicted to have a third of a standard deviation lower judgment score and a .45 standard deviation lower disgust score.
This between-disease association between advocacy and stigma could arise because some other characteristic (e.g., severity or genetic causes) predisposes diseases to more advocacy and less stigma. To control for unmeasured disease characteristics, we can compare each individual disease’s levels of advocacy and stigma across time. The within-disease advocacy variable, which is lagged by one time period, is equivalent to a coefficient from a fixed-effects model. It shows that diseases tend to have lower scores for judgment and disgust following years in which they had more nonprofits and lobbying. Together, the findings from Models 3 and 6 initially suggest that advocacy can ameliorate disease stigma.
However, the within-disease association between advocacy and stigma arises because advocacy tended to increase and stigma tended to decrease over time for many diseases. When we include linear time trends in the models, the within-disease advocacy coefficients become small and non-significant (see Table 6, Models 8 and 10). We still observe strong evidence that diseases that attract more advocacy tend to have lower levels of stigma. But in the time period we studied, we cannot attribute diseases’ stigma declines to the previous year’s activism.
In addition to medicalization and advocacy, our models also include a variable denoting how often the disease name appeared in the corpus. In most models, word count has a large, negative, statistically significant relationship with stigma. These coefficients could indicate a causal effect in which open discussions of a disease decrease stigma, or less stigmatized diseases attract more media coverage. But they could also be artifacts of the tendency for more frequently appearing words to be coded more positively in embedding models (Loon et al. 2022). Our analysis cannot distinguish between these possibilities.
Stigma’s Trajectory Over Time
Figures 3 and 4 show time trends in judgment and disgust for behavioral, infectious, and chronic conditions. 20 The shaded areas are bootstrapped confidence intervals. 21 Existing theories suggest a universal decline in stigma, possibly explained by increases in medicalization or advocacy. We do see some stigma declines over time, but not the ones predicted by theory.
One departure from theoretical predictions is that the declines in stigma were not universal, but were limited to physical illnesses. In the 1980s, there were relatively small differences in the mean levels of judgment and disgust targeting behavioral, infectious, and chronic conditions. But across the decades, stigmatizing meanings declined dramatically for chronic conditions, and infectious diseases attracted substantially less judgment (see Figures 3 and 4). The declines in stigmatizing meanings for chronic conditions were statistically significant. Because the models in Table 6 include interactions between time and both behavioral and infectious conditions, the time main effects show the trends for chronic diseases.
The most stable stigmatizing connotations are the ones centrally predicted by theories of stigma’s drivers. The links between behavioral health conditions and judgment, predicted by norm-enforcement theory, were remarkably stable over time (see Figure 3). Since the 1980s, mental illnesses and addictions have been, on average, 1.5 standard deviations more associated with judgment than the average word in the corpus. In Models 7 and 8 (Table 6), the effect of the interaction between behavioral health conditions and time cancels out virtually all of the time main effect, which highlights the fact that their stigmatizing meanings did not decline. Contagion-avoidance theory predicted strong links between infectious diseases and disgust. Consistent with this prediction, the link between infectious diseases and disgust remained particularly strong over time (see Figure 4).
Chronic conditions can also be subject to norm-enforcement and contagion-avoidance stigmas, but these pathways are less direct. The high level of disgust targeting many chronic conditions in the 1980s lends credence to the idea that contagion myths or evolved disease avoidance mechanisms allowed the stigma of infectious disease to indirectly target chronic conditions (Jones et al. 1984; Kurzban and Leary 2001; Phelan et al. 2008; Sontag 1990; Wortman and Dunkel-Schetter 1979). The associations with judgment suggest chronic diseases had denigrating implications for personhood, either because of the norm violation of illness or the belief that the world is just, and therefore unlucky people must be flawed in some way (Crandall and Moriarty 1995; Lerner 1971; Susman 1994). These stigma mechanisms are less direct than those targeting infectious diseases and behavioral conditions. They rely on symbolic or imagined contagion risk, and norm violation through the neglect of other duties rather than specifically proscribed behavior. They may therefore have been more amenable to change.
In another departure from theoretical predictions about stigma’s trajectory over time, we found no evidence that the stigma declines we observed were driven by changes in medicalization or advocacy. In Table 6, to allow for comparison of coefficients across Models 7–8 and 9–10, we limit all four models to disease years with advocacy data available. Adding the medicalization and advocacy variables to Models 8 and 10 has no effect on the time coefficients when compared to Models 7 and 9, respectively. Thus, the parallel stigma declines that we observed for dozens of chronic conditions cannot be attributed to individual diseases’ changing levels of medicalization or advocacy.
Discussion
This study tracked the stigmatizing meanings targeting more than 100 diseases across four decades to reveal how stigma varies across diseases and changes over time. The results elaborate, and in some cases challenge, prior theoretical work on disease stigma. Our findings highlight the promise of combining computational methods with traditional social science data and offer insights into how cultural meanings change.
Explaining Variation in Stigmatizing Meanings
Drawing on theoretical work on the drivers of stigma, we predicted that behavioral health conditions and preventable diseases would be marked by stigmatizing meanings linked to judgment, and that infectious diseases would spark disgust. We confirm these predictions, lending new empirical support to theories that norm enforcement and contagion avoidance drive disease stigma. In contrast, our results challenge theories about factors that ameliorate stigma. We find no support for the hypothesis that medicalization reduces stigma, and only limited evidence for a relationship between advocacy and stigma.
These findings elaborate prior work documenting a hierarchy of stigma across conditions (Thomas 2000; Tringo 1970) and connect it to theoretical work on stigma drivers. Using a relatively small number of diseases, these earlier studies found that behavioral conditions were most stigmatized, followed by infectious diseases and chronic conditions. Across a larger number of diseases, we corroborate these findings for judgmental meanings, but we see a different hierarchy for disgust, with infectious diseases scoring highest. These patterns suggest that stigmatizers’ motivations to enforce norms and avoid contagion create distinct hierarchies of stigmatizing meanings.
In our study, stigmatizing meanings were the dependent variables. Future research could use our measures of stigmatizing meanings as independent variables and document their effects on lived experiences. Stigma theory suggests that these meanings shape the degree to which members of the public endorse stereotypes and the amount of discrimination affected individuals expect to face (Link et al. 1989; Link and Phelan 2014; Pescosolido and Martin 2015), but our study did not capture these downstream effects. Studies of these effects could build on our multidimensional stigma measures, as connotations of negative personality traits, immorality, and disgust may have different consequences. For example, people whose diseases are constructed as immoral might face more discrimination, and people with diseases viewed as disgusting might face more social distancing.
Understanding Stigma Change
The links between diseases and meanings that theorists describe as directly serving stigmatizers’ interests have been remarkably stable over time. Evolutionary and power theories suggest that some stigmas emerge when stigmatizers benefit from enforcing norms. In line with these theories, behavioral health conditions are consistently marked by judgment across time. Both theories suggest that other stigmas emerge when stigmatizers are motivated to avoid contagion. Indeed, we find that infectious diseases are most strongly linked to disgust across time. For these especially entrenched stigmas, it might be fruitless to try to dislodge the stigmatizing meanings. Advocates might instead prioritize blunting their effects (e.g., through laws prohibiting discrimination in housing, the workplace, or insurance reimbursement).
The links between diseases and stigmatizing meanings that were less anchored in stigmatizers’ interests were less stable over time. Chronic conditions can be subject to secondary norm enforcement because illness itself can be perceived as norm-breaking, and because observers may assume bad things happen to bad people. Chronic conditions may also be viewed as symbolically contagious. These indirect stigma mechanisms, which have fewer direct benefits for stigmatizers, may help explain why chronic diseases were initially marked by judgment and disgust. However, chronic diseases shed these stigmatizing connotations by the end of our time period.
Our data cannot conclusively reveal why symbolic contagion and secondary norm-breaking became less linked to chronic diseases, but we suggest two possibilities. First, these indirect stigma mechanisms might be less likely to target diseases now that physical health is discussed more openly. In the second half of the twentieth century, Americans became more knowledgeable and empowered about their health and less reluctant to discuss death and dying (Lester 1993; McKinlay and Marceau 2002). Given that contact with stigmatized people is one of the most powerful ways to reduce stigma (Corrigan et al. 2012), people “coming out” as having chronic diseases may have helped decrease chronic illness stigma. Second, indirect stigma mechanisms may have weakened overall. Increasing scientific literacy might have made people less concerned about infection by any non-infectious characteristic, and people may have become less likely to blame others for any type of misfortune. This possibility aligns with contemporary research showing that rather than blaming victims, observers tend to view victims of wrongdoing as particularly moral (Jordan and Kouchaki 2021). Future research including non-disease stigmas could help distinguish between these two possible explanations for the declining stigma of chronic disease.
Either way, the parallel declines in the stigmas for most chronic conditions suggest that cultural changes intertwine. Most previous studies of how disease stigma changes over time have focused on one disease (e.g., AIDS) or disease category (e.g., mental illness), often asking whether advocates for a particular condition can successfully destigmatize it (Clair et al. 2016; Stuart et al. 2012). Prior work has discussed the relationship between cultural openness about illness and stigma one disease at a time, describing, for instance, how Republican women’s disclosures of breast cancer diagnoses decreased breast cancer stigma (Kedrowski and Sarow 2007). In line with this previous work, our regression analyses used the disease as the unit of analysis and asked, for instance, whether diseases with larger advocacy campaigns saw larger stigma declines. But disease-specific variables could not explain the declines in chronic disease stigma over time. The fact that stigma declined in parallel for so many conditions suggests that these processes did not occur separately for each disease. These broader changes, in which related cultural constructions shift together, only become visible when we study many conditions at once.
Studying Cultural Meanings Using Text Data
Contemporary theories of stigma recognize the importance of publicly circulating meanings, which are disproportionately influenced by people with power, and are therefore distinct from the beliefs espoused by individuals. Publicly circulating meanings matter because they can shape public views (endorsed stigma), provide frameworks for discrimination (enacted stigma), and transmit messages about the stigma people can expect to face (perceived stigma). Large, longitudinal corpora and novel methods for capturing meaning in text offer new opportunities to study publicly circulating meanings at scale.
When using text-based measures of cultural meanings, it is important to remember that media texts are not direct reflections of public opinion, and that types of media text are not interchangeable. Media texts can shape and be shaped by public opinion, but they are also influenced by organizational structures, legal constraints, and business interests (Peterson and Anand 2004; Schudson 2002). Therefore, text data should not replace survey- and interview-based measures of endorsed, enacted, and perceived stigma. We should also conduct studies using a variety of text sources. For this study, we drew exclusively on news media, which are available across decades and can provide insight into how cultural constructions change over time. But as a relatively elite discourse subject to specific professional standards and commercial imperatives, media data might miss stigmas that would become apparent in other types of text. Future studies might analyze language in patients’ medical records to learn about doctors’ prejudice or turn to social media to study popular culture. Purposefully selecting texts that speak to research questions, rather than using preexisting corpora, will help researchers avoid the concerns about genre balance that have cast doubt on other attempts to use texts to observe cultural change over time (e.g., Schmidt, Piantadosi, and Mahowald 2021).
Since one advantage of text analysis is the chance to measure public culture as something distinct from personal culture, we may need new ways to validate word embeddings. Previous studies have used measures of personal culture (e.g., human-rated similarities between words) as the gold standard for validating word embedding models (e.g., Caliskan, Bryson, and Narayanan 2017; Kozlowski, Taddy, and Evans 2019). But divergences between word embeddings and survey data do not always indicate problems with embedding models. They may also indicate real differences between public and personal culture (Lizardo 2017).
New ways to validate word embeddings could also strengthen our confidence in embedding-based measures of change over time. In this study, we could only validate our stigma scores against human ratings for the most recent time period. This limitation reflects a broader challenge for text analysis of historical data. Learning about past time periods when survey data are unavailable is a key motivation for text analysis, but the lack of ground truth on stigma in historical time periods makes it challenging to validate retrospective results.
Conclusion
Our work responds to calls to measure cultural meanings quantitatively and model their relationships to social structures (Mohr 1998). Cultural sociologists emphasize meanings and categorizations but rarely measure them quantitatively (Bail 2014; Mohr et al. 2020; Mohr and Ghaziani 2014). Recent studies have shown the promise of word embeddings to measure cultural constructions (Boutyline, Arseniev-Koehler, and Cornell 2023; Kozlowski et al. 2019), but these studies tend to analyze culture as a separate realm, exploring how cultural dimensions evolve and intersect with each other without analyzing their links to other variables. 22 We expand on such previous studies by analyzing the relationships between cultural constructs and other variables, illustrating new ways to incorporate embedding scores into traditional social science analyses and regression frameworks.
This study focused on the case of disease stigma, but insights from our work may help explain variation and change in other cultural meanings. Our results reveal that cultural meanings vary together in ways that are invisible in studies of single cases, highlighting the importance of large-scale studies. Our results also suggest that cultural meanings are especially strong and durable when they directly benefit powerful groups. Disease stigmas persist when they serve stigmatizers’ interests in enforcing conformity and avoiding infection; in other contexts, stigmas may persist because they facilitate economic exploitation or consolidate political power. We observed dramatic declines in chronic disease stigma with the potential to markedly improve people’s lives. But the entrenched stigma targeting behavioral health conditions and infectious diseases reminds us that some damaging cultural meanings are especially resistant to change.
Supplemental Material
sj-pdf-1-asr-10.1177_00031224231197436 – Supplemental material for The Stigma of Diseases: Unequal Burden, Uneven Decline
Supplemental material, sj-pdf-1-asr-10.1177_00031224231197436 for The Stigma of Diseases: Unequal Burden, Uneven Decline by Rachel Kahn Best and Alina Arseniev-Koehler in American Sociological Review
Footnotes
Acknowledgements
We are grateful to John Pachankis and colleagues for graciously sharing their survey data on stigma, which we used to validate our text-based measures. We are also thankful to Andrei Boutyline, Hana Brown, Josh Errickson, Joanna Kempner, participants in the Measuring and Modeling Culture workshop at the University of Michigan, participants in the Culture Workshop at the University of Notre Dame, the editors of ASR, and three anonymous reviewers for insightful feedback on our manuscript. Previous versions of this article were presented at the UC-San Diego Division of Biomedical Informatics, the UC-San Diego Department of Sociology, the UCLA Department of Sociology, and the Northwestern University School of Management.
Funding
During her work on this project, Alina Arseniev-Koehler was supported by a National Library of Medicine Training Grant (NIH grant T15LM011271) and the National Science Foundation Graduate Research Fellowship (grant number DGE-1650604). Any opinion, findings, and conclusions or recommendations expressed in this material are those of the authors(s) and do not necessarily reflect the views of the National Science Foundation.
Data Sharing
Replication files and instructions for accessing data can be found at https://github.com/arsena-k and ![]() .
.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.