
Abstract
Over the last 80 years revolutionary developments in North America have sought to modify or update perceived limitations in Freud’s clinical technique. The question asked in this paper is how to know whether any suggested modifications enhance or undermine what Freud argued was the core of psychoanalysis. Deploying a new clinical theoretical framework for comparing the ways psychoanalysts work, published clinical material is examined to explore the empirical support for Kohut’s revolution as an exemplar of how to consider other changes such as the relational “turn.” Evidence is presented to suggest that Kohut’s clinical shift from the Freudian core was based on assumptions of which Kohut was not aware. The problem that concerned him may not have derived from the core components of Freud’s theory or clinical procedure, but rather from how he understood and put them into practice. The paper concludes by suggesting that we routinely review the suppositions about the analytic situation and the data we use to draw inferences that are implicit in our clinical work, particularly if we find ourselves in an impasse. This may help us to strengthen our discipline rather than propose a new “modern” clinical psychoanalysis throwing the baby out with the bathwater.
There have been, over the last 40 years, revolutionary developments in North America seeking to modify or update perceived limitations in Freud’s clinical technique. Early critics were White, Sullivan and Horney. Then, within the American, Kohut emerged with new ideas, to be followed by the current wave of relational approaches.
The question asked in this paper is how to know whether suggested modifications (like Kohut’s) enhance or undermine what Freud argued was the core of psychoanalysis—namely the assumption that there are unconscious mental processes, a theory of resistance and repression, and an understanding of the importance of irresolvable unconscious conflicts originating in infantile sexual experience and the challenges referred to as the Oedipus complex (Freud, 1923/1955b, p. 247; see below)
My argument, based on the published material available to understand the clinical support for Kohut’s revolution (offered as an exemplar of how to consider other changes that have followed), is that Kohut’s clinical evidence for shifting away from the Freudian core was much weaker than he supposed. To a significant extent it seems to have been based on assumptions about how to do psychoanalysis that have obscured our appreciation of the very real issues his revolution was trying to address.
Deploying a new clinical theoretical framework for comparing the ways psychoanalysts work, I argue that we now have available to us a clinical (rather than abstract theoretical) way to compare what we can glean about the differences between Freud’s clinical position and any new proposals, allowing them to be better evaluated. My argument has four components.
A necessary requirement, if we are to assess the implications of modifications to Freud’s core clinical and theoretical thinking, is a comparative clinical framework able to highlight core differences in the way analysts practice in sessions and their implications.
The comparative framework that my colleagues and I have developed over the past 20 years (Tuckett et al., 2024), was designed to fit that purpose. To illustrate two aspects of it, namely, how to notice differences in suppositions that psychoanalysts put into practice both about the analytic situation and what data to rely in to infer unconscious content, I compare abbreviated descriptions of clinical work by Kurt Eissler and Wilfred Bion.
Heinz Kohut’s (1979) paper “The Two Analyses of Mr. Z” is used to show how Mr. Z’s first analyst’s way of approaching the analytic situation (K1) was in fact very similar to the way it was approached by Mr. Z’s second analyst (K2), as indeed by Eissler. Noting the similarity of Mr. Z’s two analysts, while at the same time noting their difference from other possible approaches, creates an alternative hypothesis. It is that Kohut misidentified the problem. Rather than the radical change in theory and technique that Kohut advocated (which without question requires a rejection of core aspects of Freud’s theories and techniques), could we suppose the real issue was how the analytic situation was handled? The alternative hypothesis, perhaps, is more plausible insofar as we now know that whereas K1 is Kohut’s representation of his own training analyst at work, K2 was an imaginary analyst created to suggest how things could have gone better.
The comparative framework also reveals Freud’s core suppositions about the analytic situation more clearly than before, as seen in his then revolutionary presentations of his Dora and then Ernst (the Rat Man) cases. In Dora’s case Freud’s approach failed. In Ernst’s case he at first struggled to convince his patient to believe in his interpretations, just as he had with Dora. But then he shifted his suppositions in a way that he believed allowed both his patient and himself to become convinced.
Bergmann (2004) argued that those of Freud’s dissidents who tried to change his core ideas often had reason to do so based on severe and very real personal discontent with their own experiences of psychoanalysis. Discontent and disappointment are serious states that could be expected to create a fully justified motivation for change. However, the argument in this paper is that Kohut’s theoretical and clinical shift away from psychoanalysis and toward the analysis of the self, a shift perhaps gaining momentum currently, might have been the result of a misunderstanding. The problem he was trying to expose may not have derived from the core components of Freud’s theory or clinical procedure, but rather from how they were being understood and put into practice via the treating analyst’s suppositions about the analytic situation. I conclude by suggesting that we might all benefit from reviewing the suppositions implicit in our clinical work, particularly If we find ourselves in an impasse. This may help us to strengthen our discipline rather than inventing a new kind of modern clinical psychoanalysis that throws out the baby with the bathwater.
Comparative Study
Freud (1923/1955b) stated that psychoanalysis
is the name (1) of a procedure for the investigation of mental processes which are almost inaccessible in any other way, (2) of a method (based upon that investigation) for the treatment of neurotic disorders and (3) of a collection of psychological information obtained along those lines, which is gradually being accumulated into a new scientific discipline. (p. 235)
The findings derived from the procedure that formed the cornerstone of psychoanalysis were “the assumption that there are unconscious mental processes, the recognition of the theory of resistance and repression, [and] the appreciation of the importance of sexuality and of the Oedipus complex.” These constituted “the principal subject-matter and the foundations of its theory.” “No one,” he wrote, who cannot accept them all should count himself a psycho-analyst” (p. 247).
As time has gone by, Freud’s ideas, as received within the discipline, have been elaborated, refined or sometimes rejected along two main paths—theoretical and clinical.
The theoretical path has often been the one taken by North American scholars (Foehl, 2010). But, in this contribution I am concerned with exploring the revolution in American psychoanalysis from the viewpoint that conclusions about the unconscious problems individual patients appear to suffer must rest on the hypotheses that psychoanalysts construct and believe they can validate from the data in the consulting room. To emphasize the obvious, consulting room data derive in a circular fashion from a combination of the psychoanalysts’ (conscious and unconscious) preconceptions with the details of each individual patient’s biography and current life experience as revealed through a patient’s associations and responses remembered and interpreted by their analysts in sessions. Like data in every other social field, they are constructed by the observer-participant. The point to emphasize is that this means that the data are determined in part by what the patient brings but also, crucially, by the suppositions their psychoanalyst puts into practice when they are with them as together patient and analyst “make” the sessions. Although every psychoanalyst at some level knows all this, in effect, debates have mostly ignored it—perhaps because psychoanalysts have so far struggled to feel confident that they can develop a reliable peer reviewed research culture able to resolve debates based on meaningful human science methodologies but rejecting narrow empiricism (see Denis, 2008).
The comparative clinical framework that my colleagues and I have evolved over the last 20 years and which I will shortly introduce cannot overcome the constructive element in psychoanalytic data, such as the constructions I will discuss made by Eissler, Bion and later Kohut and Freud below. However, it turns out that if we use the new framework, which focuses on differences in the core suppositions that can be inferred from studying the practice of different analysts, and then relate these to the new theories they put forward, we gain insights into the source of new theories and techniques which appear reliable.
To set out the comparative framework I begin by summarizing two published clinical accounts—from Kurt Eissler and Wilfred Bion.
Kurt Eissler (1953)
Kurt Eissler (1953) described what was at that time an orthodox North America approach clearly.
A patient is informed of the basic rule and of his obligation to follow it. He adheres to it to the best of his ability, which is quite sufficient for the task of achieving recovery. The tool with which the analyst can accomplish this task is interpretation, and the goal of interpretation is to provide the patient with insight. Insight will remove the obstacles which have so far delayed the ego in attaining its full development. The problem here is only when and what to interpret; for in the ideal case the analyst’s activity is limited to interpretation; no other tool becomes necessary. (p. 108, italics added)
He provides an example.
A patient of superior intelligence . . . filled long stretches of his analysis with repetitive complaints about trivial matters regarding his wife. He did not show any understanding of the obvious fact that the discrepancy between the intensity of his complaints and the triviality of their content required a discussion and explanation. One day the patient reported, somewhat abruptly, that he enjoyed his wife’s doing the very things he had always complained of and that he knew how secretly to manipulate situations in such a way as to make his wife act the way he had considered so obnoxious and which gave him occasion to be cold and unfriendly to her. (Eissler, 1953, pp. 138–139)
In his paper, Eissler (1953) explains how what he is struck by in this material, what he “listens to” or “attends to” to infer its unconscious meaning, is what he pictures as his patient’s hidden but repetitive sadistic impulse to be unfriendly and cold to his wife.
Based on the sense he made of what he was hearing, Eissler reports that he saw the cause of this repetitive marital problem as the unconscious sadistic pleasure the patient gained from his behavior with his wife without having to feel guilty. He intervened to explain to his patient, as he put it, what he was doing with his wife. He goes on to tell us that his patient at first acknowledged this interpretation and that in further associations, his patient volunteered that really he had known this for a long time and, according to Eissler (1953), now “showed some understanding of the uncanny sadistic technique with which he maneuvered his wife into the situation of a helpless victim without giving her an opportunity of defending herself” (p. 139). At the same time, he still “tried to prove to himself and to the analyst that he was not cruel, but that he deserved pity owing to his wife’s deficiencies.”
As sessions continued, Eissler (1953) noted that his patient continued “to present himself as injured and unjustly treated by fate in being married to an allegedly unsatisfactory partner.” So now he suggested to his patient that he was trying to assuage his feelings of guilt toward his wife.
But this idea was not accepted by the patient.
He could not understand it; he could not follow me; and he insisted upon the validity of his complaints, although he had just agreed that he himself secretly induced his wife to behave in the manner about which he habitually complained to me the following day. (Eissler, 1953)
Eissler presented the case as an example of the problems of “resistance” and I hope my brief summary will encourage further study. In the paper we learn no more about the outcome or about any additional ways of thinking about the situation or how Eissler conducted sessions.
Wilfred Bion (From “The Imaginary Twin,” 1950/2014)
This second vignette from a European Kleinian analyst is presented not to suggest it is a better way of working but to provide material to illustrate how the new comparative framework can highlight consequential differences in the suppositions analyst put into practice in sessions. 1
Brian was referred to Bion by a colleague who had concluded, after trying to treat him, that perhaps the best approach was a leucotomy.
Bion reports how the initial interview was lively enough to suggest Brian was in touch with his difficulties. However, 2 years after beginning psychoanalysis Bion and his patient had both begun to be overwhelmed by an increasing sense of pointlessness and listlessness.
As Bion reported, for a time, “my interpretations were meeting with stubborn indifference” as if “I was just a parent issuing ineffectual exhortations and warnings to a refractory child.” However, gradually Bion nonetheless began to notice something about the way Brian seemed to experience the analysis as turn-taking. He observed how he introduced regularly spaced pauses as if he was saying “Go on; it’s your turn” (Bion, 1950/2014, pp. 56–57).
Gradually, Bion (1950/2014) realized he was experiencing a dilemma: “If I broke the rhythm there was anxiety or irritability; if I continued to give my interpretations, which it now became clear he both invited and expected, there emerged a sense of having reached a dead-end” (p. 57).
Helpfully, at this point Brian arrived for a session to say he wondered if the treatment should be stopped.
Bion’s (1950/2014) response was rather calm and neutral. “Although estimations of progress in analysis were difficult to make,” he said, “there was no reason why they should not both accept Brian’s evaluation as correct.” At the same time, he suggested, “Before we pass on to consider what should be done about it, we need to know what is meant by treatment.” “It might mean psychoanalysis,” he elaborated,
in which case it would appear that some other method of approach to his problems would have to be sought [or] perhaps [a] more obvious meaning would be, psychoanalysis as practised by myself, in which case the remedy would lie in a change of analyst rather than a change of method.
However, there was yet another possibility.
We had already had reason to suppose that alleviation of symptoms was sometimes achieved by factors incidental to analysis; for example, the sense of security obtained from feeling there was someone to go to. It was possible that he was unconsciously referring to some factor of that kind. (p. 57)
Brian was silent. . . . After a prompt from Bion asking what might be on his mind, Brian revealed that it was “A woman with rheumatic pain.” “She’s always complaining about something or other and I thought that she’s very neurotic,” he continued, “I just advised her to buy some amytal and packed her off” (Bion, 1950/2014, p. 59).
Bion (1950/2014) recounts that for him this association “conjured up” Brian’s unconscious picture of what was, and had been, going on and how Brian was feeling about Bion. He was experiencing a constant picture of someone (Bion) complaining at him who needed to be given a sedative to calm down and stop bothering him.
So, this was what Bion (1950/2014) interpreted: “you feel me to be someone who makes interpretations which are vague complaints to, which, consequently it seems you need pay scant attention.” Later, he elaborated by suggesting he supposed this was why Brian’s associations were so often, many of them, “stale associations employed more for the soporific effect they shared with amytal than for their informative value.” He added that he thought they were designed to keep his analyst employed “without bothering him.”
Brian’s response to this comment was striking. His voice changed and in a depressed tone he said he felt tired and unclean. It was “as if,” writes Bion (1950/2014), “in a moment, I had in front of me, unchanged in every respect the [needy and desperate] patient as I had seen him at the first interview” (p. 59).
As with Eissler’s paper, reading the whole of Bion’s account will be worthwhile. He traces how after this understanding, Brian’s participation gradually changed and further associations and interpretations eventually allowed what Bion (1950/2014) calls a “reinvestigation” of Brian’s unconscious beliefs about his experience of being with Bion and other people. (In fact, as it turned out Brian unconsciously believed that at any moment Bion and he could become deadly rivals in terrifying ways. Consequently, his behavior in sessions was defensive, as in his life. His unconscious beliefs had meant he could get little from either.)
Surfacing Suppositions 1: The Analytic Situation
In his paper on transference, Freud (1912/1958) wrote,
It must be understood that each individual, through the combined operation of his innate disposition and the influences brought to bear on him during his early years, has acquired a specific method of his own in his conduct of his erotic life—that is, in the preconditions to falling in love which he lays down, in the instincts he satisfies and the aims he sets himself in the course of it. This produces what might be described as a stereotype plate (or several such), which is constantly repeated—constantly reprinted afresh—in the course of the person’s life . . . the peculiarities of the transference to the doctor, thanks to which it exceeds, both in amount and nature, anything that could be justified on sensible or rational grounds, are made intelligible if we bear in mind that this transference has precisely been set up not only by the conscious anticipatory ideas but also by those that have been held back or are unconscious. (pp. 99–100)
Figure 1 represents this general theory of transference graphically. 2 X, an unconscious template, is hypothesized to create repetitive experience both in a patient’s life and, therefore, necessarily in their analysis.
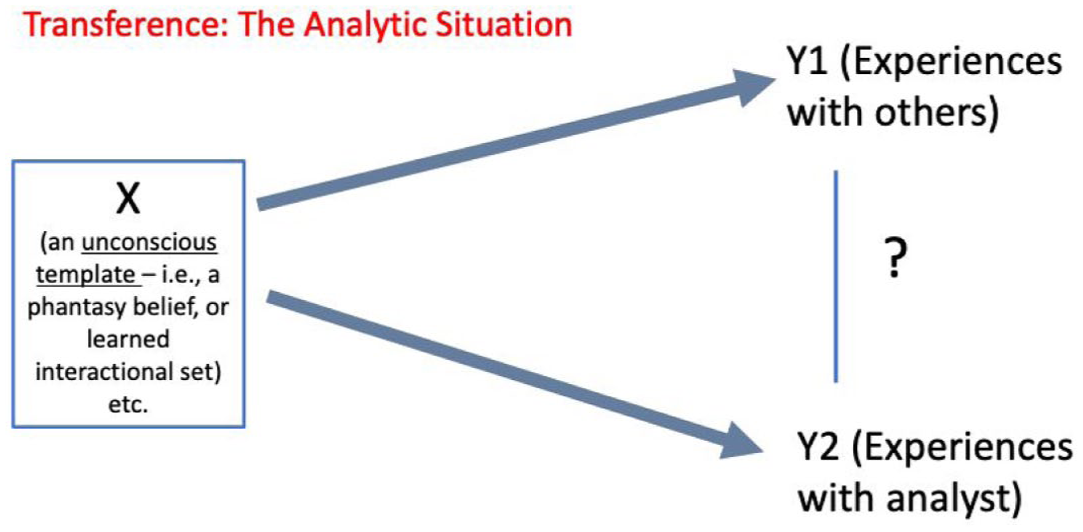
Transference: The Analytic Situation.
The two psychoanalysts, Eisler and Bion, can be said to practice in an “analytic situation” in which the patient’s transference template “X” is revealed. One way of comparing their approach is by asking how they seem to suppose that happens.
In iterative research trying to make sense of several hundred psychoanalytic sessions and through examining Freud’s and other’s published work, Tuckett et al. (2024) identified four types of supposition evident in the way psychoanalysts suppose “X” comes to be revealed. Each of the types are conceived as “ideal types” in Max Weber’s sense—abstractions used methodologically to differentiate meaningful empirical tendencies not necessarily encountered in pure form. Each type is denoted by a metaphor: Theater, Immersive Theater, Cinema and Dramatic Monologue.
To determine which type best describes a particular analyst’s work requires that we examine their account of their sessions and try to answer two questions:
Table 1 delineates the four types of supposition that are possible when these two variables (timing and participation) are combined. The horizontal rows differentiate “In whom was X visible,” distinguishing analysts who seemed to suppose the unconscious script laid down in the past could become visible by noticing consequences in themselves—for example that they were getting indifferent or sleepy or irritated and came to see this as the outcome of a response in them to their patient—or not. The vertical columns differentiate whether X appears to have been supposed to be visible right now or just more generally.
Suppositions About the Analytic Situation
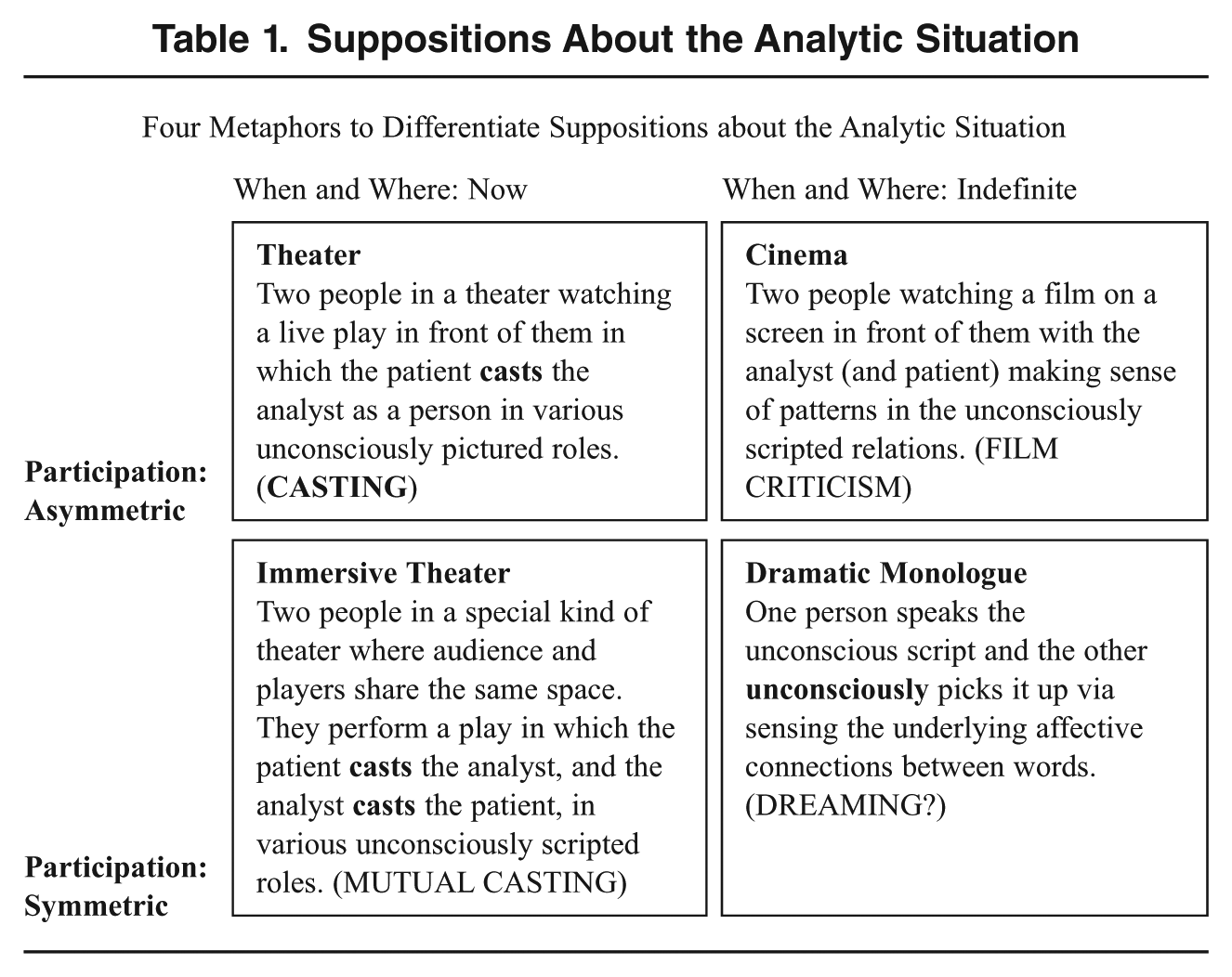
This new framework does not aim to establish a hierarchy of practice. All four types of supposition are empirically associated with successful psychoanalytic practice as evident in any careful review of published work and the sessions presented in our workshops. Rather, the point is that different sets of suppositions logically suggest different vulnerabilities, as will be elaborated below. What matters, therefore, is not whether working with one set of suppositions is better or more correct than another, but the different questions that each one raises.
If we now use the four metaphors to compare the work of Eissler and Bion described above, differences surface rather more precisely. 3
First, what Eissler tells us suggests that he supposes the analytic situation is revealed as in a “cinema.” He describes how his patient associates to events, memories, feelings and happenings and how he follows those associations so as to infer the underlying (latent) plot being depicted in the script. It is as if the associations form a film projected on the consulting room wall offering the possibility for illuminating critical commentary from Eissler or his patient.
Specifically, Eissler identifies an unconscious plot that he thinks is repeated within the associations. It is that his patient is unconsciously stuck maneuvering himself with his wife into a constant state of complaining about how badly he is treated—an activity believed in some way to enact and repeat his childhood solution to infantile sexual conflicts and anxieties and his own way of secretly enjoying himself despite his misery.
We do not know, of course, if we could question him, whether Eissler would agree that he supposed the analytic situation to be, as we characterize it, “cinema.” Nor if he thought the same pattern was being reproduced in the sessions with him via the patient’s casting or even maneuvering him into the role of “wife. But the evidence of what he does and does not tell us points in the Cinema direction. He mentions no details that suggest that he ever wondered if what was happening in the sessions could be explained by, for instance, his patient “casting” 4 his analyst into the role of complaining nag and somehow manipulating him just as he did his wife—which would suggest “theater.” Nor (if his suppositions were conceived as Immersive theater) whether Eissler ever felt the sort of frustration or desire for revenge that might have fitted in with such casting.
As with Eissler, we must also guess Bion’s suppositions based on what he does and doesn’t tell us. From the point of the new framework, differences with Eissler quickly become apparent. Bion reports, for instance, what he believed to be both his patient’s and his own feelings in the sessions. He informs us, for example, about how he thought his interpretations in sessions led him to wonder if he “was just a parent issuing ineffectual exhortations and warnings to a refractory child” and also how he felt trapped in a journey to a “dead end.” Then when Brian associated to the “woman with rheumatic pain . . . always complaining . . . [whom the patient] just advised . . . some amytal and packed . . . off,” Bion understood Brian as casting him in the same way. Consequently, Brian needed to protect himself in the same way. The detail alerts us to depict Bion’s view of the analytic situation as what we characterize as “theater”—that is, as a place where “X,” the template becomes visible via signs of the way the analyst is unconsciously experienced in sessions. In fact, as elaborated in Tuckett et al. (2024), what Bion tells us about how he came to recognize how he got drawn in and trapped by his own casting of Brian as fragile, actually suggests “immersive theater.” 5
Surfacing Suppositions 2: What Data are used to Infer Unconscious Content
A second component of the comparative framework asks what data psychoanalysts use to enable them to infer unconscious content that would be “almost inaccessible in any other way” (Freud, 1923/1955b).
We use the four questions in Table 2 to ask about the data being used. Answering them as far as we can, we note that although both Bion and Eissler essentially use Freud’s procedure and seem to be trying to guess at much the same sort of underlying issues, the data source of their inferences is radically different. Bion, but not Eissler, makes extensive use of his own feelings and thoughts, using them to reflect on his patient’s unconscious beliefs.
Questions to Assess the Levels of Data Used to Infer X
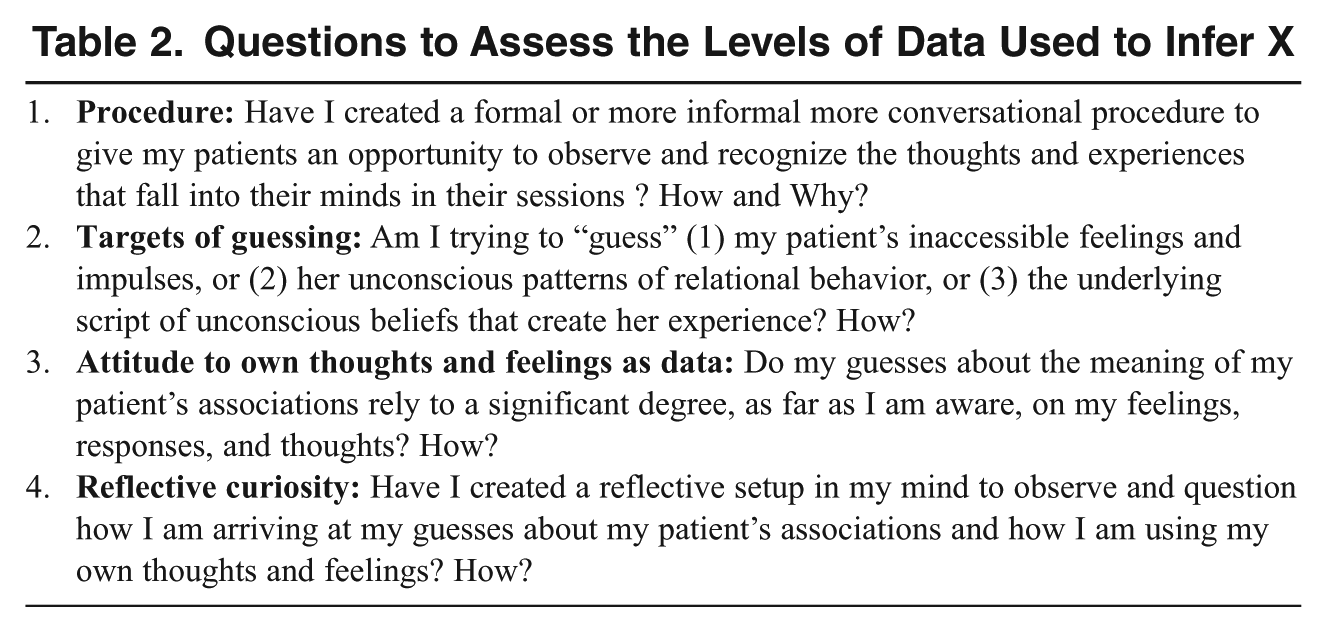
Figure 2 represents the three sources of data that analysts might use to make inferences as to their patients’ unconscious beliefs and impulses.
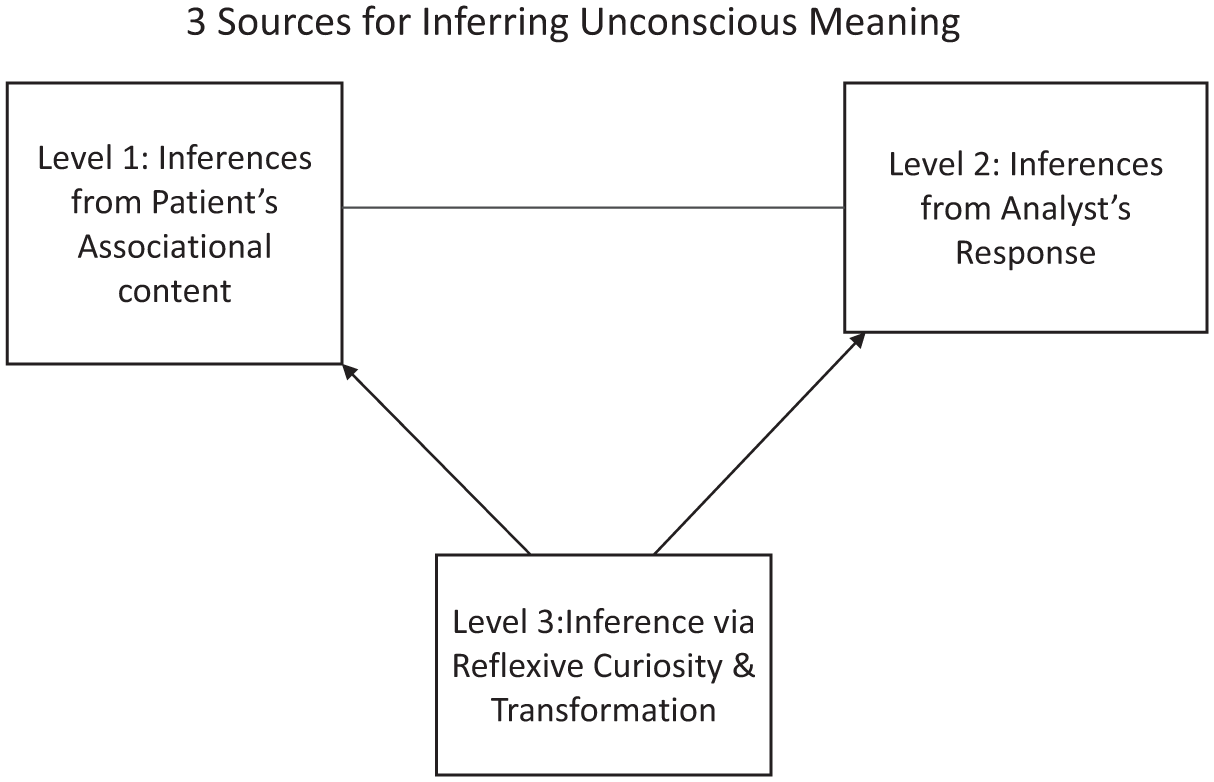
Three levels of data
Use of Level 1 was well illustrated by Eissler’s example. He focused on his patients’ associations as revealing repetitive patterns in his life and, perhaps with the aid of moments of resistance, embarrassment, slips, or errors or via inferring the meaning of symbols and dreams, he establishes deeper latent meanings. There is a wealth of literature on how psychoanalysts can infer fascinating insights in this way, from Freud on. Bion also used this level.
Use of Level 2 was absent in Eissler’s description of his session. He mentioned nothing about his thoughts and feelings in in his report, although it is not difficult for a reader to sense his frustration. Analysts working like Eissler, which includes many today, consider it a strength—not a failing—to try to manage not to act out their feelings. Whatever frustration Eissler might have had, given this approach, he might have argued it was not permissible to use such unreliable and subjective responses which, if focused on, might interfere with an accurate analysis of the patient. In contrast, Bion’s report extensively described his feelings and thoughts prompted in the sessions by being with and listening to Brian. He, clearly, supposed his feelings and thoughts to be important to note and reflected on and to be potentially relevant data for discovering “X.”
Note, its not a simple case of one is better than another. While Bion’s use of his own experience as data may make intuitive sense in the case described, some critics (like Green, 1993) of analysts who discuss their feelings extensively (e.g., Jacobs, 1993; Ogden, 1994) suggest that it can be an indulgence which carries significant risks (e.g., imposing one’s own wants and needs on those of the patient or failing to notice details that might otherwise emerge).
Logically, to use Level 3 requires use of Level 2. It refers to what might be called the transformation of raw data (Levels 1 and 2) into a meta-level—as when Bion describes how he brings what Bran is saying together with his own experience and his ideas about what may be giving rise to it which crystallizes when Brian mentions the old woman. Level 3 data are meta-constructed to transform Levels 1 and 2.
Having introduced the new way to compare analysts via their suppositions about the analytic situation, the procedure they establish and the sources of data they draw on, I now introduce its use for comparative purposes.
The Two Analyses of Mr. Z
“The Two Analyses of Mr. Z” (Kohut, 1979) is the most detailed available example of Kohut’s “revolutionary” way of working
6
and was written to illustrate it. Kohut describes how Mr. Z’s analysis took place in two instalments, each conducted five times a week and lasting about 4 years, which were separated by an interval of about 5½ years. The first instalment occurred when he “was viewing analytic material entirely from the point of view of classical analysis” but the second coincided with the time when he was “beginning to test a new frame of reference”:
“a new viewpoint, which, to state it briefly, allowed me to perceive meanings, or the significance of meanings, I had formerly not consciously perceived. This case thus allows me to demonstrate that the change in my theoretical outlook that had taken place during this time influenced decisively the focus of my perception of Mr. Z’s psychopathology and enabled me, to the great benefit of the patient, to give him access to certain sectors of his personality that had not been reached in the first part of his treatment.
I will refer to Mr. Z’s first analyst as K1 and to his second analyst as K2. As with the cases from Eissler and Bion discussed above, any conclusions we draw about K1 and K2’s method must rest on the information about the two analyses Kohut provides in the paper—in which presumably he selected the points he thought important.
Most of the important points in the text consist of accounts of the different readings of the “historical” information made in the two analyses constructed from Mr. Z’s memories of his childhood and his thoughts about his relationship with his mother and father. The key point was that very different and very relevant material about the past is said to have come up in the two analyses.
Of most significance, when writing about “the psychotic core, the central pre-psychological chaos” of Mr. Z’s mother’s personality, discovered in the second analysis, Kohut (1979) reports what he takes to be historical facts, which had not become known to the first analyst. For instance, he writes about how K2’s picture of Mr. Z’s mother was of the “the central hollowness of her self . . . covered over by a rigidly maintained hold on and control over her selfobjects whom she needed in order to shore up her self . . . .” The factual status of this picture is supported by Mr. Z recalling in the second analysis how to superficial acquaintances his mother
presented a picture of normal emotionality, even outsiders soon felt the lifelessness that lay underneath the appearance of normality . . . (and that) none of Mr. Z’s classmates and acquaintances, either from primary school or later, liked to visit his house, which contributed to his social isolation . . . . (pp. 15–16)
The new picture of the mother creates a different reading of the first year of analysis with K1 and, in Kohut’s (1979) view, explains why it was so difficult. Then Mr. Z had apparently exhibited “unrealistic, deluded grandiosity” and made “demands that the psychoanalytic situation should reinstate the position of exclusive control, of being admired and catered to by a doting mother.”
Kohut (1979) reports how K1 had understood his patient as exhibiting a “regressive mother transference” and made interpretations about Mr. Z’s deluded wishes. They were met with “intense resistances.” However, after about 18 months Mr. Z became calmer to the extent that the analyst (K1) now remarked to Mr. Z that the analytic work (i.e., the interpretations) was now bearing fruit. But Mr. Z disagreed. He thought that things were better not from the interpretations but because K1 was now behaving differently! He said he knew this because he recalled K1 saying to him, empathically, on one occasion that “Of course, it hurts when one is not given what one assumes to be one’s due” (pp. 15–16).
This observation, of course, is a sign of the change to come, which emerges quite quickly as Kohut (1979) describes the second analysis. Although the kind of data reported does not change so that in some ways the content of Kohut’s description of the second analysis reads very much like the first, what Kohut clarifies is that K2 listens and interprets from a “new viewpoint.” It allowed him “to perceive meanings, or the significance of meanings” in the material, that K1 had “formerly not consciously perceived.”
For example, the way K2 responded to a dream Mr. Z presented at the beginning of the second analysis is discussed. The dream involved “a dark-haired man in a rural landscape dressed in city clothes in a complex but harmonious way wearing a ring.” K2’s (new) perspective led him to infer that what this dream was revealing was Mr. Z’s wish for an unobstructed and harmonious relationship to an idealized father/analyst.
Kohut (1979) argues that although K1 had also noticed the intensity of this wish, he had believed it necessary to interpret this type of material confrontationally in terms of deluded grandiosity and Mr. Z’s wish to have his mother as a defensive effort to avoid hatred and rivalry, and so forth. Not so for K2. For him the dream was the expression of a wish for a different kind of self-object to the one he had experienced so far—not his mother but a different kind of (internal) father-analyst. Hearing things through this lens, K2 desisted from making any of what were called “condemning” interpretations used by K1. Consequently, Kohut argues, in the second analysis the issue faded away after a few weeks rather than being something analyst and patient got stuck on.
In the paper Kohut (1979) does discuss what he calls the puzzling question as to how it was that what he considers the crucial material about the psychotic mother had not appeared during Mr. Z’s first analysis. He writes,
To be sure, it had indeed appeared, but—what is even more incomprehensible—it had failed to claim our attention. I believe that we come closest to the solution of this puzzle when we say that a crucial aspect of the transference had remained unrecognized in the first analysis. Put most concisely: my theoretical convictions, the convictions of a classical analyst who saw the material that the patient presented in terms of infantile drives and of conflicts about them, and of agencies of a mental apparatus either clashing or co-operating with each other, had become for the patient a replica of the mother’s hidden psychosis, of a distorted outlook on the world to which he had adjusted in childhood, which he had accepted as reality—an attitude of compliance and acceptance that he had now reinstated with regard to me and to the seemingly unshakable convictions that I held. (pp. 15–16)
Although Mr. Z still became quite openly “self-centred, demanding, insisting on perfect empathy, and inclined to react with rage” whenever he felt his analyst was not ideal (Kohut, 1979, p. 11), the fractious interactions that had occurred in the first analysis were not repeated because K2 is described as understanding the self-centered state as “an analytically valuable replica of a childhood condition that was being revived in the analysis” and, importantly, as a positive development and reliable indication that “we were now moving in the right direction” (p. 12).
Arguing that K2’s broadened perception exerted a change in his attitude “vis-à-vis Mr Z,” Kohut also describes memories that Mr. Z brought to sessions about when he was 9. Considering this to be a positive evolution Kohut writes that he now thinks many previous interpretations (from K1) had either not been useful, or incorrect or harmful. Mr. Z’s unresolved fractious behavior to K1, therefore, should be understood as a product of the interpretations made to him. In the paper, Kohut makes clear his belief that in the second analysis no data at all materialized in the sessions to suggest Mr. Z’s memories were accompanied by what he thinks of as explicit evidence of the Oedipal conflicts that had captured K1’s attention—for example a sense of hopeless rivalry and defeat by his father. Rather, Kohut describes how in the new analysis Mr. Z insists he was proud of his loved father.
To compare K1’s and K2’s way of working, we can ask if, using the terms we did earlier for Eissler and Bion, they adopted different procedures, drew on different data, and had varied suppositions about the analytic situation.
When considered from these three comparative perspectives, the striking fact about Kohut’s accounts of the two analyses of Mr. Z is that in respect of both the data-level the analysts draw on and their models of how unconscious templates are revealed in the analytic situation, there are no substantial differences. Both analysts seem to be trying to guess the underlying unconscious script creating the patient’s experience in the present by seeking meaning in what they are being told by Mr. Z about his past—particularly his memories. Neither account includes detailed interchanges between patient and analyst and neither reports specific feelings and thoughts generated in the analyst during specific sessions. 7 In consequence neither account draws on examples of any thoughts or feelings the analysts’ might have noticed in particular sessions as they, perhaps, attended in evenly hovering attention.
Did the two analysts have different ways of supposing the way unconscious templates are revealed in the analytic situation?
On the hand, it is important to acknowledge that in the paper Kohut (1979) does, as apparent in the quotation above, refer to the puzzle as to why K1 had not noticed the psychotic mother that Mr. Z was struggling with and did refer to the plausible explanation that somehow when K1 was interpreting Mr. Z “as struggling with infantile drives and of conflicts about them, and of agencies of a mental apparatus either clashing or co-operating with each other,” K1 might have been becoming for the patient “a replica of the mother’s hidden psychosis.”
If K2 is an analyst who supposes transference templates to be revealed via the casting of the analyst in the analytic situation, as in the theater, then we would expect him to be on the alert for the possibility of being pictured by Mr. Z as a psychotic mother-person making intolerable demands or as a person in various other roles. If he also supposed that he could be somehow reacting to Mr. Z driven by some unconscious response of his own, then we would imagine he supposed templates are revealed via the Immersive Theater mode. With only the paper to go on, we cannot be sure if either are the case. However, to this reader it looks that although Kohut may have had the theoretical insight writing the paper to explain that Mr. Z (of course Kohut himself, in fact) may have experienced K1 as mad, due to his constant “condemning interpretations,” this is not central. Moreover, the lack of detailed exchanges or reports of any direct comments made to Mr. Z about his unconsciously experiencing either analyst as one thing or another, suggest, at the very least, that neither Kohut or the two analysts he portrays suppose transference templates are revealed in that way. 8 Rather, Kohut seems more concerned with reality than subjective experience—what the mother was really like as experienced by Mr. Z’s friends, and so forth, not how she was experienced with the reasons left open.
Readers can think this over examining Kohut’s paper themselves, but the point being made here is that both K1 and K2, like Eissler in his account of his work, appear to practice, in terms of the distinctions offered above, by supposing that transference templates are mainly revealed in the analytic situation characterized as a place where analyst and patient can view and discuss accounts of the patient’s life and memories (in other words, using the cinema metaphor, essentially as films projected onto the consulting room wall whose meaning can be disputed as by two film critics expressing different interpretations of the films).
From this viewpoint, therefore, the principal difference to emphasize between how K1 and K2 each practice is that they have different perspectives on the film plots in front of them. Oversimplifying, K1 saw Mr. Z as caught up with an unconscious rivalry with his father and his analyst, whereas K2 sees him more as trying to escape from a mad mother and gain recognition and love from his father along with his analyst. These differences in interpretation were believed by Kohut to derive from their differences in confronting their patient, leading K2 to forego “condemning” interpretations. But such differences existed inside the similarity of their suppositions about how the “X” (the transference template) in the analytic situation and how an analyst supposes it is revealed in the detail of sessions like Mr. Z’s, as well in their similarity in relying on only the first source of data to draw inferences about Mr. Z’s unconscious mental functioning.
Freud’s Suppositions
The point of Kohut’s paper on the two analyses of Mr. Z was to argue that K2’s theoretical approach of avoiding confrontation and considering alternate meanings of what he was told about his patient’s childhood was superior to that of K1—whose assumptions Kohut described as those of a classical analysis. It led him also to argue that what was needed was a change in practice away from the interpretation of the unconscious presence of infantile Oedipal conflicts as still disabling patients like Mr. Z’s adult life toward interpretation aimed at fostering more satisfactory (internal) selfobjects.
However, an alternative hypothesis is suggested by what we have learned from looking at K1 and K2 using the new framework. Could it be that for the purpose of helping Mr. Z to understand how trapped he was in the unconscious infantile Oedipal conflicts from which Freud argued we all suffer, there was a bad fit between the two sets of suppositions being discussed as evident in both his analyst’s practice and Mr. Z’s psychology as a patient?
In my view, Kohut as Mr. Z, felt deeply that he had never been convinced by K1 (as he experienced him) and thought that he and other patients like him needed an analyst they could experience differently. How could this happen? One possibility is that rather than adopt a whole new way of doing psychoanalysis leaving out the impact of infantile sexual conflicts, a new (third) analyst could revise his or her suppositions about the way transference templates are revealed and then interpreted in the analytic situation and the sources of data available to infer “X.”
The new framework is intended to facilitate thinking about differences and so providing alternatives. The hypothesis offered after looking at Mr. Z’s case is that it was Kohut’s (and, therefore, K1 and K2’s) suppositions that produced the impasse in the face of the clinical challenge he presented. “Cinema” and “first data level” suppositions, it seems, are vulnerable to the difficulties posed by a patient like Mr. Z. It seems likely he cast his first analyst ambivalently and as unfair and biased against him, perhaps in competition with him and certainly deeply insensitive to his need for love from him. The analyst’s interpretations, therefore, were never heard as emanating from a benevolent but neutral source. A similar sort of problem seems to have been present for Eissler’s patient, who, perhaps unconsciously, experienced his analyst as beating him up. 9
This hypothesis can be understood better by extending the comparative analysis of clinical practice to Freud’s conduct of the Ernst case (the Rat Man).
It has long been recognized that the crucial breakthrough in Freud’s understanding of transference as the dominant influence in the analytic situation starts to appear in the detail of his attempted explanation of his failure with Dora, which he saw as the outcome of neither understanding nor interpreting her transference-based experience of him. What has not, however, always been clear (Diercks, 2018) is exactly what Freud had understood.
In the crucial passage (translated from the German by Diercks in a slightly different way to Strachey), Freud describes the clinical situation in Dora’s case as influenced by a whole series of former psychic experiences that come alive “not as the past but as the present relationship to the person of the physician [italics added]” (Diercks, 2018, pp. 61–62). 10 In other words, in the terms introduced above, in the present in the session, the analyst as a person is felt by the patient to be what “X” is making him.
Expressed like that Freud clearly envisages the analytic situation not as cinema with two film critics conversing but as theater. He was being cast by Dora as an unpleasant and frightening person—literally being turned as a person (i.e., in his entirety) into persons as she experienced them in the past. 11 However, Freud’s own conversion to this new way of thinking about the analytic situation is not always maintained in his subsequent descriptions of practice, which may help us to understand why it has not caught on generally. Indeed when he describes working with Ernst (the Rat Man) a few years later, he is at first manifestly back in the cinema—listening to the material, creating his own understanding (film criticism) and trying to convince a resistant Ernst (another film critic who doubts the interpretations), that his construction of his childhood relationship to his father is true. 12
The likelihood that the shift Freud made is not universally recognized in practice is compounded by the fact that, when Freud set it out when he wrote up this case, he was preoccupied with enhancing his credibility by showing that his theories could be verified empirically. Therefore, rather than focusing on the revolutionary technical change required to analyze Ernst, Freud’s paper (which comes with his supporting notes) was largely preoccupied with setting out his quite complex and subtle hypothesis about the cause of Ernst’s symptoms and demonstrating that his construction was “true.”
In his account, Freud writes that in the sessions he noticed that Ernst repeatedly addressed him as “Captain”—that is as a feared cruel superior—and that this enabled him to grasp that Ernst was making a transference from the father to him, which was making things difficult. He seems to have tried to deal with this difficulty by persuasion, stressing his (neutral and objective) role as doctor, and so forth. At one point he even reports that to this end he had tried what we could today call reassurance, telling Ernst that “I myself had no taste whatever for cruelty, and certainly had no desire to torment him” (Freud, 1909/1955a, p. 166).
In other words, at this point in his account of the treatment, Freud could be characterized as viewing the analytic situation as cinema and trying to emphasize to his patient that he is an objective interpreter, an outsider to the film on the screen. This is also evident a few pages later when Freud reports that (to remove resistance as it were) he had tried again to reassure Ernst that “I myself was not fond of cruelty like Captain N., and that I had no intention of tormenting him unnecessarily” (Freud, 1909/1955a, p. 169). In other words, at this point, like Eissler or K1, Freud is like a nonaligned film critic putting hypotheses to Ernst that he has derived from Ernst’s stories and associations to events and memories.
But like both Eissler’s patient and Mr. Z with K1, Ernst wouldn’t have it. He insisted he did not remember or attach significance, for example, to the beating incident with his father, despite, Freud thought, the compelling logic it offered to support his hypothesis.
The case, as described, only turns round when Freud fully realizes, using the comparative terminology, that he and Ernst are not in the cinema but in the theater and that progress is being held up because Freud is not a person unconsciously cast by Ernst as helpful and neutral. Rather he is a person with all the attributes of the cruel captain/father who is feared and also suspected of wanting to take revenge on Ernst in the sessions. We learn that thoughts Ernst had and eventually had to reveal to Freud about Freud’s family added to Ernst’s shame and fear of retribution.
Freud’s account shows how all this clarified to him that Ernst’s dreams, slips, associations and behavior in many sessions were evidence of his unconscious casting of his analyst as a person who was against him:
Things soon reached a point at which, in his dreams, his waking phantasies, and his associations, he began heaping the grossest and filthiest abuse upon me and my family, though in his deliberate actions he never treated me with anything but the greatest respect. His demeanour as he repeated these insults to me was that of a man in despair. “How can a gentleman like you, sir,” he used to ask, “let yourself be abused in this way by a low, good-for-nothing fellow like me? You ought to turn me out: that’s all I deserve.” While he talked like this, he would get up from the sofa and roam about the room—a habit which he explained at first as being due to delicacy of feeling: he could not bring himself, he said, to utter such horrible things while he was lying there so comfortably. But soon he himself found a more cogent explanation, namely, that he was avoiding my proximity for fear of my giving him a beating. If he stayed on the sofa he behaved like someone in desperate terror trying to save himself from castigations of terrific violence; he would bury his head in his hands, cover his face with his arm, jump up suddenly and rush away, his features distorted with pain, and so on. He recalled that his father had had a passionate temper, and sometimes in his violence had not known where to stop. Thus, little by little, in this school of suffering, the patient won the sense of conviction which he had lacked—though to any disinterested mind the truth would have been almost self-evident. (Freud, 1909/1955a, p. 209)
Reading this passage and its concluding sentence, suggests that at this point Freud was unequivocally making suppositions about the analytic situation that we would characterize as theater.
So why has this shift not been widely recognized or taken on and used by North American analysts like Eissler and Kohut? One reason, as already suggested, is that it may be the way Freud wrote up the case of Ernst—not to clarify and publicize his new technique to his colleagues but to prove to doubters in the wider world the historical truth of his theory about the origin of Ernst’s difficulties in infantile sexual conflicts. Another reason may have been ambivalence. It is plain in Freud’s description of the case that both Freud and Ernst suffered embarrassment and pain in the sessions. They each sought to avoid inflicting suffering on the other. The vivid detail of Ernst’s beliefs was only revealed when Freud changed his suppositions about what was going on between them. It is also possible that Freud had an embarrassing inkling that he had been drawn in to beating Ernst up in his frustration to get through to him, even enacting the part of Father-Captain, as he had been cast. Moreover, we have argued elsewhere that Freud became troubled the more he realized that his method depended on his own, that is the analyst’s, unconscious—in fact on unconscious-to-unconscious communication (Tuckett et al., 2024). This was an inconvenient realization for the claim that psychoanalysis had a “scientific” base at a time it was trying to gain a foothold, particularly in North America in the atmosphere that was to produce the Flexner report. 13
Conclusions
Heinz Kohut was a major figure in transforming psychoanalysis in North America—theoretically, clinically and administratively. There is no doubt that much of this influence ushered in a new atmosphere of respect for difference and was highly beneficial. But, more generally, has his work enhanced or undermined psychoanalysis?
Kohut liked to make clear that he did not see himself as rejecting the main lines of Freud’s discoveries (Basch, 1984) and would, I think, be shocked to think his work might have been undermining. Moreover, to answer such a controversial question properly would require a much more profound study than the one offered here.
However, Kohut’s description of the second analyst treating Mr. Z portrays an analyst who developed a much more trusting and successful relationship with his patient than the first one. This first analyst is portrayed as captured by his classical theories. The second, not so. The clear implication is the need for a theoretical and clinical shift. Moreover, Kohut’s portrayal of the more interpersonal analysis required for narcissistic and similar patients, given the “widening scope” of psychoanalytic work in North America, seems to have a significant current appeal—especially when compounded by the other discontents associated with critiques of classical or ego psychology psychoanalysis that are crudely labeled as “relational” approaches. All this is a revolution. Or at least a radical updating.
Therefore, insofar as we treat Kohut’s discontent and the clinical and theoretical revolution he inspired as an example of a wider trend in clinical psychoanalysis, the possibility I have highlighted that his discontent emerged not from his analyst’s rigid commitment to classical theory and technique but from the specific suppositions within which they practiced it, may be worth further consideration.
In other words, are the problems Kohut saw, and many others see, with traditional psychoanalysis as an authoritarian, insensitive, out of touch, out of date practice that fails to take account empathetically of patients’ needs for affirmation, the result of both a theoretical and inferential error? The inferential error is to be blind to the vulnerability of the “cinema” approach to the analytic situation and the theoretical error is to deemphasize the role of unconscious psychic reality in determining experience. Authoritarianism, to take one example, is not an inherent aspect of Freud’s clinical procedures (the fundamental rule and evenly hovering attention, which necessarily implies an attitude of technical neutrality). Those procedures are unique to psychoanalysis and are the method Freud designed to reveal the otherwise inaccessible and unwanted. What makes his procedures authoritarian are not the procedures themselves, but the suppositions psychoanalysts bring to their practice and the context in which they do so. While “cinema” suppositions and a reliance on Level 1 data can work very well in some clinical situations, practice based solely on them is vulnerable to impasse, like Freud’s with Dora and Ernst, and then, perhaps, into a descent into authoritarianism and countertransference enactments whenever patients bring to their sessions unconscious castings of their analyst that prevent the analyst being seen as a helpful film critic with interesting ideas.
In short, while practicing clinical psychoanalysis will always remain challenging, in my view Kohut’s discontents and his solutions to them, do not in any way undermine the case to continue putting front and center of our work the revolutionary assumptions about the core of psychoanalysis raised at the beginning of this paper that Freud put forward just over 100 years ago.
Footnotes
1
2
For those interested it can be noted that Freud’s idea about transference as an ongoing template can be expressed in modern neuroscientific terms as a Bayesian “updating” problem, the organism failing to adjust to “predictive coding” error (Friston, 2010).
3
Bearing in mind that unlike in the lengthy workshops we devoted to trying to understand an analyst’s suppositions in our project, in which the analyst could be questioned, in these cases guesses about suppositions are based only on their reports published for a different purpose.
4
See ![]() , pp. 255–256) for a discussion of significant translation issues underlying our use of the word cast. In the Standard Edition the German verb besetzen and noun Bessetzung become in English cathect and cathexis. They are used when Freud is discussing transference. Alternative translations in English are to occupy (occupied) or to cast into a role (that exists).
, pp. 255–256) for a discussion of significant translation issues underlying our use of the word cast. In the Standard Edition the German verb besetzen and noun Bessetzung become in English cathect and cathexis. They are used when Freud is discussing transference. Alternative translations in English are to occupy (occupied) or to cast into a role (that exists).
5
6
It is now well known that the two analyses described in the Mr. Z paper were, in fact, created by Kohut from his view of his own analysis in the United Stated and a self-analysis presented as a (fictional) second analysis by a new analyst—probably drawing on analyses conducted by Kohut and his group and published in the volume edited by Goldberg (1978)—although none of these case descriptions provide any more detailed accounts of the “to and fro” of the new approach. The emphasis is on the analyst’s new understanding of material. Apparently Kohut constructed the account to illustrate his views of how he subsequently came to think his own analysis should have been done (Angueli, 2015; Bromberg & Aron, 2019; Brothers, 2015; Cocks, 2002; Kirsner, 1982; Lichtenberg, 2008; Strozier, 1999, ![]() ). However, in this paper I proceed on the basis of Kohut’s paper alone.
). However, in this paper I proceed on the basis of Kohut’s paper alone.
7
There is a place towards the end of the paper where Kohut (as K2) describes feeling empathic for Mr. Z and also allows us to gather, much as we can from Eissler’s descriptions of his work, that the first analyst (K1) felt frustrated towards Mr. Z while the second analyst gradually felt more positive. These, however, are general dispositions, probably important, rather than examples of specifically session content generated data.
8
Above I described how K1 did report his patient telling him that in his opinion he (K1) had changed (as a person in the analysis) for the better but nothing is said about the implication that this picture implies a different previous picture. Neither is it reported as to whether this new picture was resilient.
9
To be clear again “cinema” can be very effective with the right patient and a successful case with cinema suppositions described by Busch (2013) is discussed in ![]() .
.
10
In the Standard Edition, the English reads a little less directly, “a whole series of psychological experiences are revived, not as belonging to the past, but as applying to the person of the physician at the present moment” (Freud, 1905/1953, p. 116).
11
12
Early on in Ernst’s analysis Freud had already pieced together his hypothesis—Ernst’s difficulty in his relationship to men (such as “the captain” who was his army superior) was driven by unconscious aspects of his relationship to his father, which Freud elaborated particularly in relation to an incident at age 4, when Ernt’s father had given him a severe beating for some sexual misdemeanour to which Ernst responded so strongly that it never happened again.
13
A report published in 1910 argued there was a total absence of scientific standards for medical education, clinical practise, and therapeutic devices in the United States. Along with the federal Pure Food and Drugs Act of 1906 the Flexner reports changed the course of medicine, and the effects, both positive and negative, are still felt today. The report standardized medical education, supposedly based on scientific principles and demonstrable facts. Practices were declared scientifically unsupportable (although no actual research was done to back up many statements) and legally excluded from clinical practise. Doctors also had certain equipment removed from their offices and taken to “museums of quackery.”